Impact of atrial tachyarrhythmias on paravalvular regurgitation post-transcatheter aortic valve implantation: recognition and management
Jingyao Yang, Yu Du, Yujie Zhou, Zhijian Wang

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
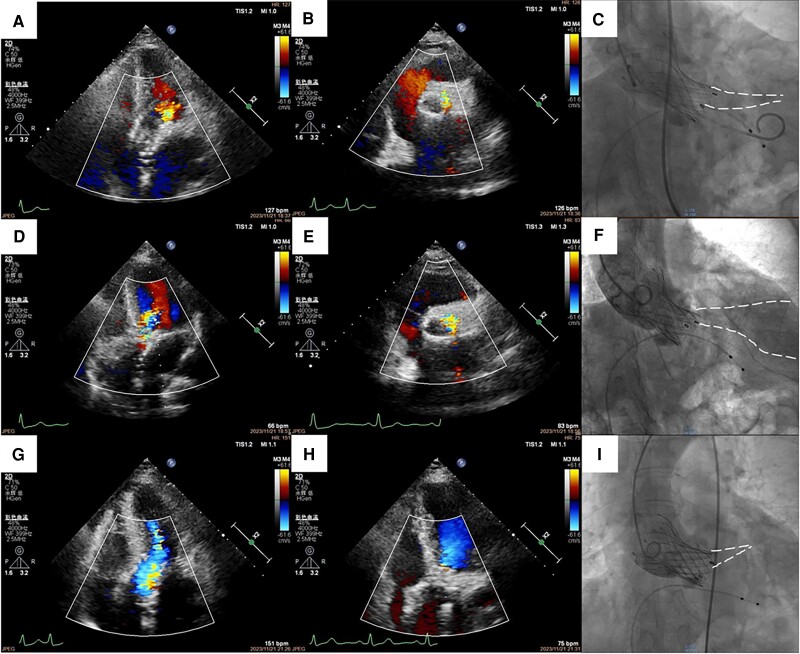 Figure 1
Figure 1- —Beijing Municipal Natural Science Foundation10.13039/501100005089
- —National Natural Science Foundation of China10.13039/501100001809
- —The Capital Health Research and Development of Special10.13039/501100010270
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Cardiac Arrhythmias and Treatments · Cardiac pacing and defibrillation studies
A 70-year-old woman with severe aortic stenosis was admitted for transcatheter aortic valve implantation (TAVI). The patient had a type I bicuspid aortic valve with right–left cusp fusion. Intra-operative transthoracic echocardiography (TTE) and aortography after prosthesis (Taurus NXT#26, Peijia Medical) implantation showed mild aortic paravalvular regurgitation (PVR) (Figure 1A–C; Supplementary material online, Videos S1–S3), while the electrocardiogram showed atrial tachyarrhythmias. However, after removing the left ventricular guidewire and femoral artery sheath, repeat TTE showed significant deterioration in the prior PVR (Figure 1D and E; Supplementary material online, Videos S4 and S5), when the patient was in sinus rhythm with a normal heart rate. Therefore, re-access via femoral artery was performed, followed by aortography confirming a moderate-to-severe PVR from aortic right–left cusp fusion (Figure 1F; Supplementary material online, Video S6). After implanting a second prosthesis (Taurus NXT#26, Peijia Medical), TTE showed trace PVR while atrial tachyarrhythmias recurred (Figure 1G; Supplementary material online, Video S7). To ensure accurate assessment of PVR, propafenone 70 mg was administered intravenously. Finally, both the intra-operative TTE and aortography showed trace PVR (Figure 1H and I; Supplementary material online, Videos S8 and S9) when the patient was in normal rhythm and heart rate.
Evaluation of PVR during TAVI procedure using TTE relies heavily on colour Doppler jet characteristics, easily affected by abnormal haemodynamics (i.e. arrhythmias).^1^ To ensure an accurate assessment of PVR, pharmacological stabilization of haemodynamics is indispensable, and integration of other echocardiographic and invasive haemodynamic findings is also helpful.
Supplementary Material
ytae346_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Zoghbi WA , Asch FM, Bruce C, Gillam LD, Grayburn PA, Hahn RT, et al Guidelines for the evaluation of valvular regurgitation after percutaneous valve repair or replacement: a report from the American Society of Echocardiography developed in collaboration with the Society for Cardiovascular Angiography and Interventions, Japanese Society of Echocardiography, and Society for Cardiovascular Magnetic Resonance. J Am Soc Echocardiogr 2019;32:431–475.30797660 10.1016/j.echo.2019.01.003 · doi ↗ · pubmed ↗