Ceftaroline-Induced Thrombocytopenia: A Case Report
Diego Ortiz-Mendiguren, Ian Crespo-Orta, Mark Miranda-Márquez, Nicole Rivera-Bobe, Glorivette San Vicente-Morales

TL;DR
A 69-year-old man developed severe low platelet count after taking ceftaroline, emphasizing the need to recognize this rare drug side effect.
Contribution
This case report highlights ceftaroline-induced thrombocytopenia, a rare but critical adverse drug reaction.
Findings
Ceftaroline caused a rapid and severe drop in platelet count from 204,000 to 4,000 x 10³/μL within a day.
Prompt recognition and intervention prevented major complications despite anticoagulation therapy and bleeding risk.
Abstract
Drug-induced thrombocytopenia is a rare but significant adverse effect of certain medications, with the potential for severe bleeding, thrombosis, and death. This report discusses a rare case of severe thrombocytopenia induced by ceftaroline in a 69-year-old male with a history of atrial fibrillation on rivaroxaban and allergies to amoxicillin and sulfa drugs. Following the initiation of ceftaroline for left lower extremity purulent cellulitis, his platelet count dropped from 204,000 to 4,000 x 10³/μL within a day. Given the low platelet levels, anticoagulation therapy, and bleeding risk, immediate interventions and prompt recognition prevented major complications, highlighting the importance of recognizing drug-induced thrombocytopenia in clinical practice.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
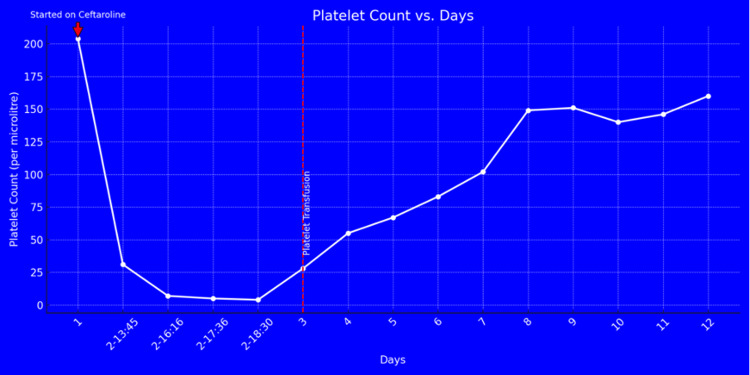 Figure 1
Figure 1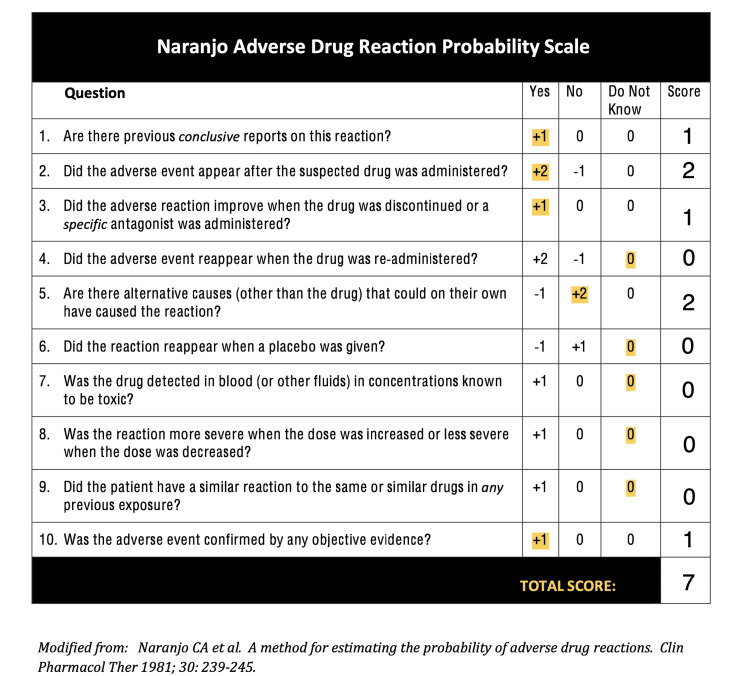 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHeparin-Induced Thrombocytopenia and Thrombosis · Antimicrobial Resistance in Staphylococcus · Antibiotics Pharmacokinetics and Efficacy
Introduction
Drug-induced thrombocytopenia (DIT) is a rare but significant adverse effect of certain medications, with an incidence of approximately 10 cases per 1,000,000 people per year and a prevalence of about 25% in critically ill patients. Thrombocytopenia, characterized by a decreased number of platelets, can lead to severe bleeding or thrombosis. DIT often presents as an acute and severe decrease in platelet count, typically below 50 x 10³/μL, increasing the risk of spontaneous hemorrhages [1].
Common drugs causing DIT include beta-lactam antibiotics (e.g., penicillin, cephalosporins), NSAIDs, antiviral agents, chemotherapeutic agents, and antiplatelet drugs. The mechanisms of DIT include reduced platelet production due to bone marrow suppression and accelerated platelet destruction, which can be immune-mediated or non-immune, typically presenting five to 10 days post-exposure, with platelet counts often falling below 20,000 x 10³/μL [2].
Clinical symptoms range from asymptomatic to life-threatening hemorrhages. It is crucial to differentiate DIT from other causes like heparin-induced thrombocytopenia (HIT), ITP, and thrombotic thrombocytopenic purpura (TTP), as management strategies vary. Management involves prompt recognition, discontinuation of the offending drug, supportive care, and sometimes steroids or intravenous immunoglobin (IVIG). Diagnostic workup includes CBC, blood smear analysis, and tests for antiplatelet antibodies [1-2]. This report discusses a rare case of severe thrombocytopenia induced by ceftaroline in a 69-year-old male.
Case presentation
A 69-year-old male with atrial fibrillation on rivaroxaban and a history of allergies to amoxicillin and sulfa drugs presented with partially treated left lower extremity purulent cellulitis. Given purulence and previous antibiotic treatment, ceftaroline was chosen. He was admitted to the ward and started on ceftaroline. A routine CBC revealed a platelet count drop from 204,000 to 30,000 x 10³/μL the following day. Repeat lab work during the day showed continued down-trending to 7,000 x 10³/μL. Given the concern of platelet clumping, a repeat laboratory on citrate was performed, which revealed platelets at 4,000 x 10³/μL.
Vital signs were notable for a heart rate of 74 beats per minute, blood pressure of 110/65 mmHg, and respiratory rate of 18 breaths per minute. The physical exam showed no petechiae or signs of bleeding. Labs revealed reticulocytes at 2.3%, elevated haptoglobin at 293 mg/dL, bilirubin within normal limits, elevated fibrinogen at 738 mg/dL, and mildly increased lactate dehydrogenase (LDH) at 239 u/L. The coagulation profile showed international normalized ratio (INR) prolongation at 1.74 (on rivaroxaban), and the peripheral smear was without schistocytes.
Given the severe thrombocytopenia, the primary care team immediately notified the hematology-oncology service. A PLASMIC score of 4 indicated a low probability of TTP, and there was no recent exposure to heparin products. Given the acute presentation, IV steroids with dexamethasone, removal of the probable offending agent, and a platelet transfusion were recommended. Ceftaroline was discontinued as it was the only new medication the patient had recently started, raising concern for medication-induced thrombocytopenia. Due to the decreasing platelet trend, anticoagulation therapy, and very high risk of bleeding, the patient was transferred to the medical intensive care unit for a higher level of care.
Following the discontinuation of ceftaroline, the infectious disease service recommended transitioning the patient to ciprofloxacin and vancomycin. After stopping ceftaroline and changing the antibiotics, the patient's platelet levels gradually increased over the next few days. By day 8, the platelet count had risen to 150 x 10³/μL and continued to improve over time (Figure 1). The Naranjo adverse drug reaction scale scored ceftaroline at 7, suggesting it was the probable cause of the thrombocytopenia.
Platelet count and days: Following the initiation of ceftaroline, the platelet count steeply declined from the patient's baseline levels, reaching a minimum of 4 x 10³/μL. The platelet count then gradually increased, demonstrating recovery after the discontinuation of ceftaroline, platelet transfusion, and initiation of steroids.
Discussion
In the hospital setting, acutely ill patients are known to develop thrombocytopenia, defined as an acute drop of platelets below 150 x 10³/μL [3]. Thrombocytopenia is often asymptomatic but can present with bleeding complications such as petechiae, epistaxis, easy bruising, purpura, bleeding gums, and even life-threatening hemorrhage [4]. Consequently, identifying the cause of a rapidly dropping platelet count is crucial, as it can significantly impact patient outcomes.
Ceftaroline-induced thrombocytopenia is a rare side effect, with only a handful of documented cases [4]. It is essential to consider this possibility in patients experiencing a sudden platelet drop shortly after starting the medication. Differentiating between Heparin-induced thrombocytopenia (HIT), Idiopathic Thrombocytopenic Purpura (ITP) is essential, and Thrombotic Thrombocytopenic Purpura (TTP), as their management strategies differ significantly. Drug-induced thrombocytopenia often results in more severe platelet count reductions compared to other causes, with levels below 20,000 x 10³/μL associated with a higher risk of bleeding. This rapid decline, with platelets dropping from 200,000 to 30,000 x 10³/μL in just one day, is consistent with what we observed in our patient. On the Naranjo scale (Figure 2), a score of 7 suggests ceftaroline as the probable cause of thrombocytopenia [5].
Naranjo Adverse Drug Reaction Probability ScaleModified from [5]
The exact mechanisms by which ceftaroline-induced thrombocytopenia is caused are not fully understood, but multiple possibilities exist. Beta-lactam antibiotics, particularly first to third-generation cephalosporins, can cause a form of thrombocytopenia through an immune-mediated reaction [4,6-8]. The beta-lactam ring in these antibiotics can bind to free haptens in the bloodstream, forming hapten-antibody complexes that act as antigens, triggering antibody production [4]. These antibodies are then thought to target and destroy platelets. Another possible explanation is that ceftaroline might also cause decreased platelet production through myelosuppression, although this requires further investigation [9-10].
Prompt recognition and management are essential to prevent serious complications. Including prompt cessation of the offending drug (ceftaroline in this case) and initiating appropriate treatment based on the underlying cause of the thrombocytopenia.
Conclusions
This case highlights the critical need for awareness of drug-induced thrombocytopenia. Early identification and treatment can significantly improve patient outcomes, particularly in those on anticoagulants with an already increased bleeding risk.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Drug-induced thrombocytopenia: mechanisms and laboratory diagnostics Semin Thromb Hemost Danese E Montagnana M Favaloro EJ Lippi G 2642744620203156312710.1055/s-0039-1697930 · doi ↗ · pubmed ↗
- 2Drug-associated thrombocytopenia Hematology Am Soc Hematol Educ Program Bakchoul T Marini I 576583201820183050436010.1182/asheducation-2018.1.576PMC 6246020 · doi ↗ · pubmed ↗
- 3How to approach thrombocytopenia Hematology Am Soc Hematol Educ Program Stasi R 191197201220122323358010.1182/asheducation-2012.1.191 · doi ↗ · pubmed ↗
- 4Cefepime: a novel cause of thrombocytopaenia BMJ Case Rep Muhammad S Ahmad S Khan BA Yousaf A 15202210.1136/bcr-2021-243749 PMC 876796435039337 · doi ↗ · pubmed ↗
- 5Liver tox: clinical and research information on drug-induced liver injury Liver Tox: Clinical and Research Information on Drug-Induced Liver Injury Bethesda (MD)National Institute of Diabetes and Digestive and Kidney Diseases 2019 https://www.ncbi.nlm.nih.gov/books/NBK 548069/
- 6Thrombocytopenia with sodium cephalothin therapy Ann Intern Med Gralnick HR Mc Ginniss M Halterman R 401404771972 https://www.acpjournals.org/doi/pdf/10.7326/0003-4819-77-3-401434089910.7326/0003-4819-77-3-401 · doi ↗ · pubmed ↗
- 7Immune thrombocytopenia induced by cephalosporins specific for thiomethyltetrazole side chain J Clin Pathol Lown JA Barr AL 70070140198710.1136/jcp.40.6.700-b PMC 11410713611401 · doi ↗ · pubmed ↗
- 8Hematoma of the iliopsoas muscle due to thrombocytopenia resulting from the administration of a third-generation cephalosporin Ann Hematol Onodera M Fujino Y Inoue Y Kikuchi S Endo S 8258268920102001204410.1007/s 00277-009-0872-x · doi ↗ · pubmed ↗