Duodenal Varices Presenting as Lower Gastrointestinal Bleeding
Olachi Egbo, Bassel Dakkak, Onyinye S Ugonabo, Christopher Magiera

TL;DR
This paper discusses the challenges of treating duodenal varices, a serious condition causing severe gastrointestinal bleeding.
Contribution
The paper highlights the need for improved understanding and treatment strategies for duodenal varices.
Findings
Duodenal varices are linked to high morbidity and mortality due to severe bleeding.
The case emphasizes the importance of advancing knowledge and treatment approaches for this condition.
Abstract
Duodenal varices pose a significant clinical challenge due to their association with severe gastrointestinal bleeding. This condition requires attention because of its acute severity, high morbidity, and mortality rates. The presented case underscores the importance of advancing both knowledge and treatment approaches for duodenal varices. This pursuit is aimed not only at improving immediate clinical outcomes but also at deepening our understanding of complications related to portal hypertension.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
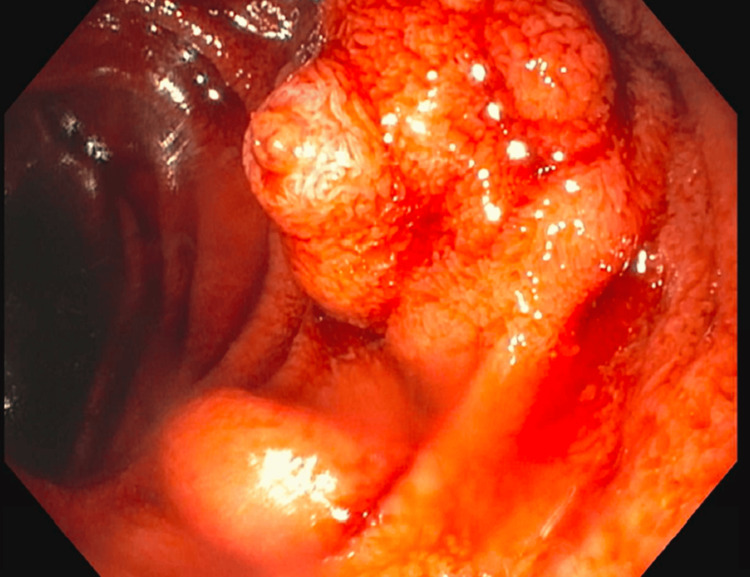 Figure 1
Figure 1| Test Name | Value | Reference Range |
| White blood cell count | 4.1 | 4.5–10 × 109 cells/L |
| Hemoglobin | 11.8 | 14–17 g/dL |
| Blood urea nitrogen | 7 | 7–20 mg/dL |
| Creatinine | 0.67 | 0.6–1.3 mg/dL |
| Prothrombin time (PT) | 13 | 11–13 seconds |
| International normalized ratio (INR) | 1.3 | 0.8–1.2 |
| Lactic acid | 3.8 | 0.5–2.2 mmol/L |
| Alanine transaminase (ALT) | 94 | 7–56 IU/L |
| Aspartate transaminase (AST) | 314 | 10–40 IU/L |
| Alkaline phosphatase | 140 | 30–130 IU/L |
| Bilirubin (total) | 2.8 | 0.1–1.2 mg/dL |
| Ethanol | 154 | 0–10 mg/dL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLiver Disease and Transplantation · Abdominal vascular conditions and treatments · Gastrointestinal Bleeding Diagnosis and Treatment
Introduction
Portal hypertension occurs when the portal venous pressure abnormally increases, subsequently causing collateral connections between the portal and systemic circulations, primarily resulting in visibly enlarged veins called varices [1]. Ectopic varices are characterized as enlarged portosystemic collateral veins situated in atypical locations outside the gastroesophageal area [2]. Duodenal varices are ectopic varices that make up 1-3% of all varices found in patients with cirrhosis. While this proportion may appear modest, the notable aspect is the high mortality rate associated with duodenal varices, which can escalate to as much as 40% [3]. This condition was initially reported by Alberti in 1931 [4]. Duodenal varices arise primarily from chronic liver diseases such as cirrhosis and commonly occur in the duodenal bulb and the second portion of the duodenum [5]. The treatment approach includes a combination of endoscopic therapy, radiological intervention, and surgery [5]. Our case focuses on a patient with liver cirrhosis experiencing duodenal variceal bleeding manifesting as lower gastrointestinal bleeding, which was effectively managed with sclerosing therapy and a transjugular intrahepatic portosystemic shunt (TIPS).
Case presentation
A 53-year-old male patient presented with painless bright red rectal bleeding and dizziness a few hours before admission. He has a known history of decompensated alcoholic cirrhosis but was lost to follow-up. Other medical history includes hypertension and obstructive sleep apnea on CPAP therapy. His alcohol history was significant for the consumption of approximately 12 fl oz of hard seltzer drinks daily, with his last drink being a day before presentation. He denied any hematemesis, coffee-ground emesis, or previous gastrointestinal hemorrhage. His first esophagogastroduodenoscopy (EGD) in 2014 showed no varices. His home medications include amlodipine 10 mg, metoprolol succinate 100 mg, furosemide 40 mg, and spironolactone 100 mg. Vitals were significant for sinus tachycardia with a heart rate of 124 bpm and borderline low blood pressure at 104/64 mmHg. On examination, there was bright red rectal bleeding. Significant laboratory results showed a decrease in hemoglobin levels, elevated blood ethanol, lactic acid, and liver enzymes (see Table 1). Computed tomography (CT) angiography of the chest, abdomen, and pelvis showed hepatic steatosis, signs of portal hypertension, and possible right portal vein stenosis or thrombosis. He was started on a proton pump inhibitor (PPI), an octreotide infusion, and transfused one unit of packed red blood cells.
An EGD revealed moderate portal hypertensive gastropathy, small esophageal varices without stigmata, and actively bleeding duodenal varices (see Figure 1). The bleeding was successfully controlled with sclerosing therapy. To reduce the risk of rebleeding, the patient also had a TIPS and balloon-occluded retrograde transvenous obliteration (BRTO). He was discharged after four days in stable condition, and his home medications were resumed. Two weeks post-discharge, he attended his follow-up appointment and reported no recurrence of rectal bleeding.
EGD findings of bleeding duodenal varices. EGD: esophagogastroduodenoscopy.
Discussion
Gastrointestinal (GI) bleeding is divided into upper and lower bleeding. Lower GI bleeding is defined as bleeding that starts below the ligament of Treitz and usually presents as bright red blood per rectum. Bleeding above the ligament of Treitz usually presents as melena or hematemesis. However, if the bleeding is brisk, it may present as hematochezia [6]. Duodenal varices can be due to extrahepatic or intrahepatic causes. While liver cirrhosis accounts for the most common intrahepatic cause, extrahepatic causes can include portal hypertension, thrombosis, obstructive tumors, arteriovenous fistula, and pancreatitis [5, 7, 8]. Sadum et al. reported a case of duodenal variceal hemorrhage after a sleeve gastrectomy [9].
Duodenal varices represent a challenging clinical entity, as identifying these lesions as the origin of bleeding can be difficult. They are relatively rare compared to esophageal varices, and their uncommon location in the duodenum makes them less likely to be considered. Establishing a diagnosis may require multiple successive endoscopies (EGDs) [10]. Unlike esophageal varices, duodenal varices are not frequently screened for, leading to potential delays in diagnosis and management. Duodenal varices present with rare but fatal gastrointestinal bleeding. The diagnosis of duodenal varices is predominantly confirmed through endoscopy [11]. CT and magnetic resonance imaging are useful for visualizing the portal venous system and assessing the extent of liver disease. Doppler ultrasound is also beneficial for evaluating blood flow in the portal vein and detecting varices. Finally, capsule endoscopy is a less invasive technique that can be used in patients where conventional endoscopy is not feasible or inconclusive [11].
The treatment options for duodenal varices can be divided into endoscopic, interventional radiology procedures, and surgery. Endoscopic therapeutic modalities include endoscopic band ligation, endoscopic injection sclerotherapy, endoscopic tissue adhesive (ETA), and combination therapy. Singh et al. reported ETA treatment with cyanoacrylate glue that resulted in successful obliteration of the duodenal varices [12]. While the injection of cyanoacrylate is considered a viable endoscopic treatment for bleeding duodenal varices, there are technical challenges associated with glue injection, such as determining the optimal method for accessing the vessel when it is situated in the second part of the duodenum [13]. A meta-analysis by Yipeng et al. [14] reported an overall treatment success of 81.2% among patients who had endoscopic intervention. However, adverse events noted include endoscopic treatment-induced ulcer, portal vein thrombosis, biliary obstruction, pulmonary embolism, abdominal pain, and sepsis [14].
Compared to endoscopic therapy, interventional radiology procedures like TIPS decompress the portal system and are especially beneficial in cases of unsuccessful endoscopic treatment [15]. TIPS has its limitations, including shunt occlusion, a significant mortality rate, and hepatic encephalopathy [16]. BRTO assesses the portal vein retrogradely through the gastrorenal shunt and uses occlusion balloons to stagnate sclerosant material within the varix. It is used as a therapeutic adjunct or alternative to TIPS. Percutaneous transhepatic obliteration (PTO) works in a similar way to BRTO. Double balloon-occluded embolotherapy (DBOE) combines both BRTO and PTO and may be a better treatment option than BRTO [2]. DBOE approaches from both the feeding and draining veins, thus reducing the risk of bleeding compared to BRTO. Plug-assisted retrograde transvenous obliteration (PARTO) was introduced in 2013 by Gwon et al. [17]. It is also known as a modified BRTO and uses a vascular plug and gelatin sponge instead of an indwelling balloon catheter [18]. Though most reported cases of successful PARTO were in gastric varices, Lee et al. [19] reported a case of duodenal varices that was successfully treated with PARTO. This modified method, though having a shorter procedure time compared to BRTO, is incapable of achieving complete occlusion with a mesh material and cannot be applied to varices with a gastrorenal shunt exceeding 18 mm due to constraints in the size of the vascular plug [19]. Adjunct radiological interventions after endoscopic intervention depend on the clinical status of the patient and generally improve mortality.
Lastly, surgical procedures like duodenal resection and extrahepatic portosystemic shunts are performed in rare cases where endoscopic and interventional radiological treatments are not feasible or effective, such as in the case of extrahepatic portal venous obstruction [2, 7].
Conclusions
In summary, duodenal varices are a challenging entity in diagnosis and treatment. They should be considered in the differential diagnosis for any patient presenting with lower gastrointestinal bleeding, alongside other causes of lower gastrointestinal bleeding. Diagnosing ectopic varices requires high clinical vigilance. Although non-invasive tests are available to detect ectopic varices, endoscopy remains the main method to confirm the diagnosis. Early detection is crucial to prevent life-threatening bleeding. The current choice of treatment modality depends on the clinical scenario and may include interventional radiology (TIPS and BRTO), combined with endoscopic methods. Further studies are needed to determine the best approach for treatment.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Endoscopic band ligation of bleeding duodenal varices Cureus Dzwonkowski M Iqbal U Kaufer SW Khan YI Kumar K 014202210.7759/cureus.22009 PMC 891351435340508 · doi ↗ · pubmed ↗
- 2Clinical characteristics and treatment for patients presenting with bleeding duodenal varices Dig Endosc Kakizaki S Toyoda M Ichikawa T 2752812220102117547910.1111/j.1443-1661.2010.01007.x · doi ↗ · pubmed ↗
- 3Clinicopathological features and treatment of ectopic varices with portal hypertension Int J Hepatol Sato T Akaike J Toyota J Karino Y Ohmura T 960720201120112199487910.4061/2011/960720 PMC 3170857 · doi ↗ · pubmed ↗
- 4Duodenal variceal bleeding successfully treated with transjugular intrahepatic portosystemic shunt: a case report and review of the literature Turk J Gastroenterol Attila T Kolbeck KJ Bland ZM Wang A Rodriguez SA 284290192008 https://pubmed.ncbi.nlm.nih.gov/19119491/19119491 · pubmed ↗
- 5Successful management of a bleeding duodenal varix by endoscopic banding Singapore Med J Tan NC Ibrahim S Tay KH 723725462005 https://pubmed.ncbi.nlm.nih.gov/16308648/16308648 · pubmed ↗
- 6Diagnosis of gastrointestinal bleeding: a practical guide for clinicians World J Gastrointest Pathophysiol Kim BS Li BT Engel A Samra JS Clarke S Norton ID Li AE 467478520142540099110.4291/wjgp.v 5.i 4.467PMC 4231512 · doi ↗ · pubmed ↗
- 7Ectopic varices: anatomical classification, hemodynamic classification, and hemodynamic-based management Tech Vasc Interv Radiol Saad WE Lippert A Saad NE Caldwell S 1581751620132383067310.1053/j.tvir.2013.02.004 · doi ↗ · pubmed ↗
- 8Life-threatening bleeding from duodenal varices due to pancreatic arterio-venous malformation: role of emergency pancreatoduodenectomy Hepatogastroenterology Perera MT Shimoda M Kato M Abe A Yamazaki R Sawada T Kubota K 15531556552008 https://pubmed.ncbi.nlm.nih.gov/19102341/19102341 · pubmed ↗