Underwater modified strip biopsy for colorectal polyp invading into the appendiceal orifice
Miyuki Iwasaki, Kenichiro Okimoto, Naoki Akizue, Yuki Ota, Takashi Taida, Tomoaki Matsumura, Jun Kato, Naoya Kato

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
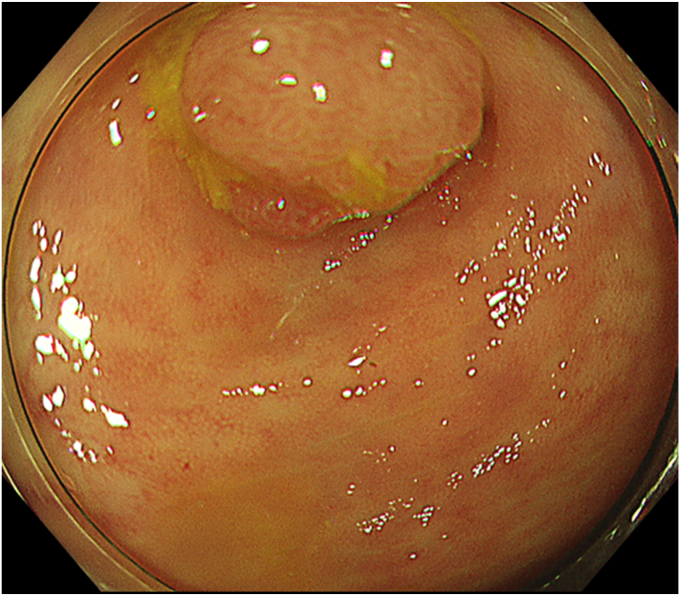 Figure 1
Figure 1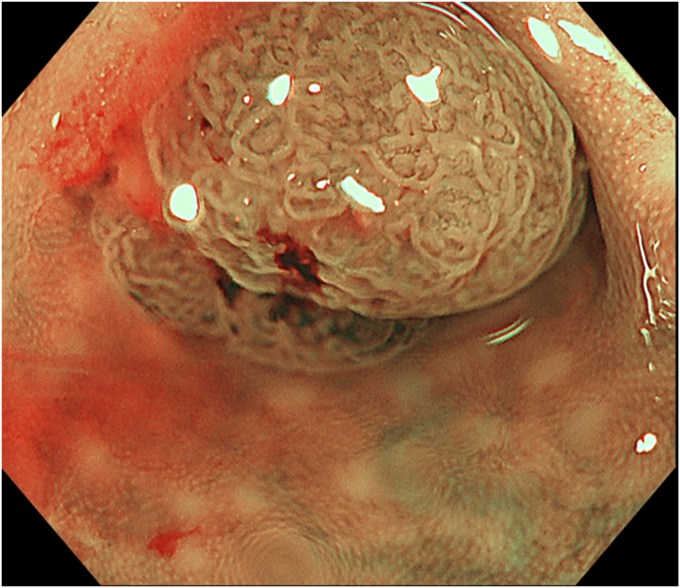 Figure 2
Figure 2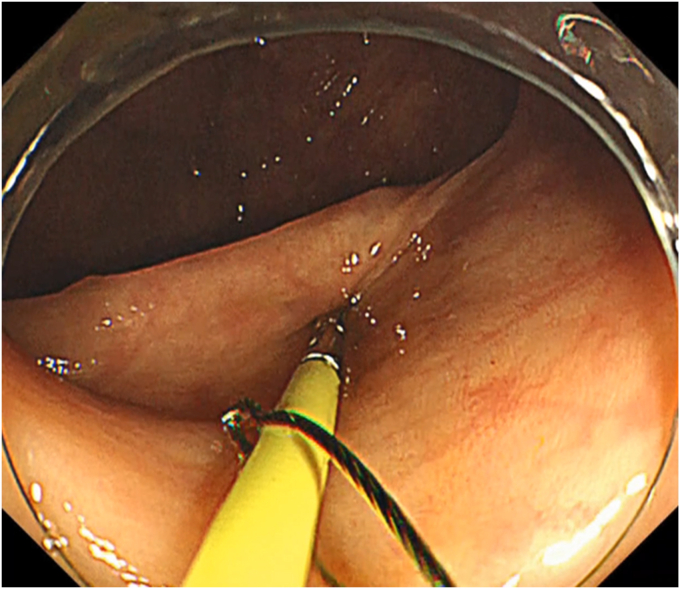 Figure 3
Figure 3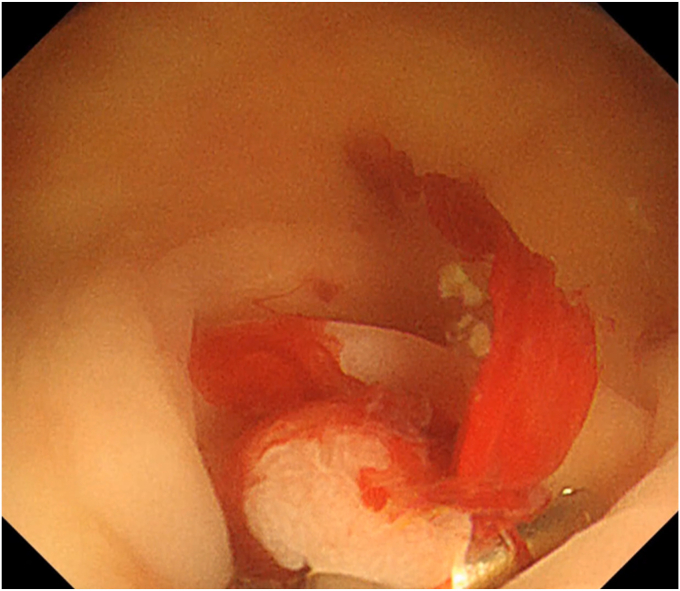 Figure 4
Figure 4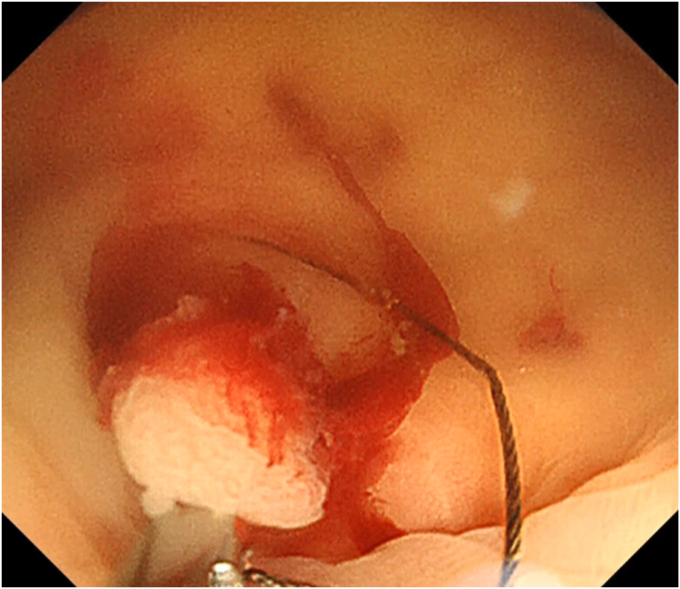 Figure 5
Figure 5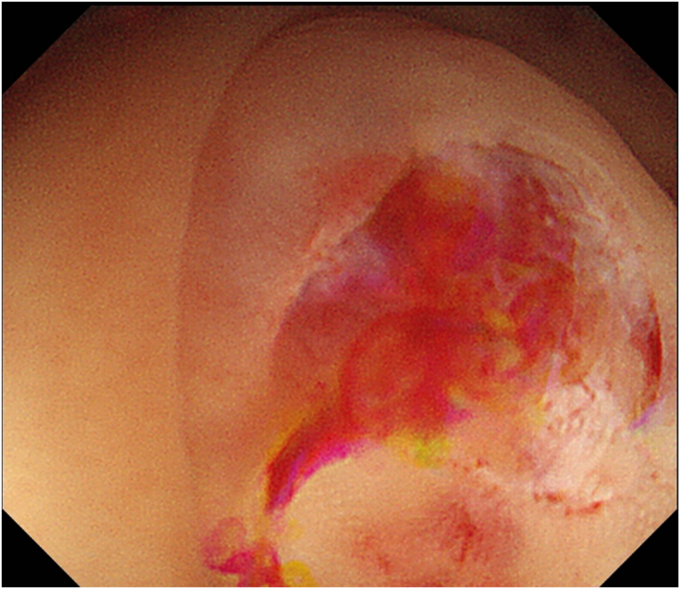 Figure 6
Figure 6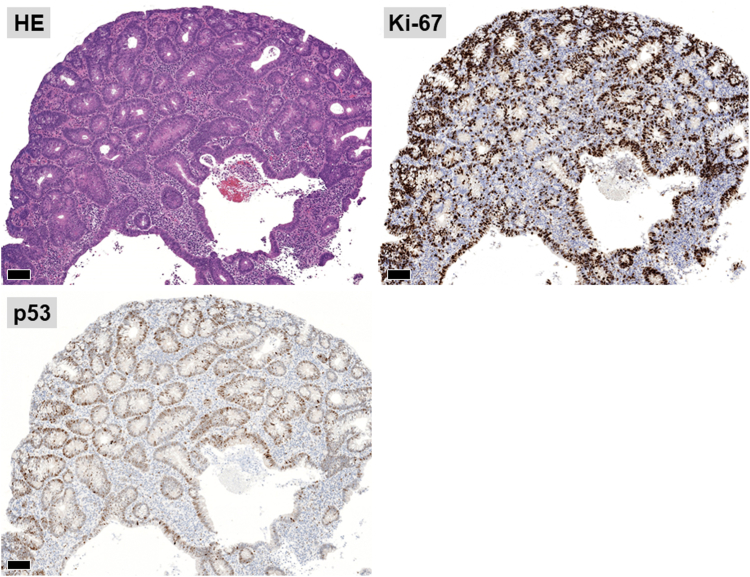 Figure 7
Figure 7Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPsychological Treatments and Disorders · Medical research and treatments
Introduction
For colorectal EMR, polyps invading into the appendiceal orifice are one of the difficult cases.1^,^2 The location of the appendiceal orifice, the shape of the cecum, the thinness of the cecum wall, and fibrosis of the submucosal layer are also factors that make EMR difficult and increase the risk of accidental injury.2 Various endoscopic resections methods for polyps invaded into the appendiceal orifice have been reported.1 Recently, there have been some reports of endoscopic full thickness resection of polyps at the appendiceal orifice, but severe adverse events such as appendicitis, stricture, perforation, and bleeding have been reported.3 Eventually, there is no consensus on the treatment of such polyps. Here, we present the case in which such a polyp was resected via underwater modified strip biopsy (Video 1, available online at www.videogie.org).
Case Presentation
The patient was a 60-year-old man. The elevated 6-mm polyp invading into the appendiceal orifice was identified, but it was difficult to observe the entire polyp with CO_2_ insufflation (Fig. 1). The polyp showed Japan Narrow-Band Imaging (NBI) Expert Team type 2A, which was suspected to be an adenoma (Fig. 2). To observe the entire polyp supported by a strip biopsy technique, the procedure was performed using GIF-2TQ260M (Olympus Medical Systems, Tokyo, Japan), but it was still difficult to observe the entire polyp with CO_2_ insufflation. Therefore, we performed the procedure with underwater conditions using the floating effect. As the first step of the resection, the forceps (TechGrasper; MC Medical, Tokyo, Japan) was passed through the snare (AGS polypectomy Snare H; Hangzhou AGS MedTech Co, Ltd, Zhejiang, China; snare shape hexagonal, open width 10 mm) (Fig. 3). The polyp was observed and grasped by forceps with underwater condition, then pulled out toward the lumen (Fig. 4). Owing to the underwater condition, the polyp floated into the lumen and was easy to grasp and to confirm the polyp’s distal margin. The lesion was resected en bloc by cold snare polypectomy (CSP) (Fig. 5). the procedure time from passing forceps through the snare to resection is about 5 minutes. After resection, it was confirmed endoscopically that there was no residual tumor (Fig. 6). The pathology revealed the tumor to be a high-grade tubular adenoma (Fig. 7, scale bar 100 μm). The proliferative cell zone, positive for Ki-67, extended broadly from the superficial layers to the base of the glands, indicating enhanced proliferative activity. Conversely, p53 exhibited a wild-type pattern, with sporadic and discontinuous positive staining observed. The resection margins (both horizontal and vertical) were unclear. We scheduled follow-up magnifying endoscopy and biopsy from the resected scar 1 year after the treatment (at the time of the article, 1 year has not elapsed since the treatment).Figure 1. The polyp of the appendiceal orifice. White-light image of the polyp.Figure 2. The polyp was classified with Japan NBI Expert Team type 2A suspected to be an adenoma.Figure 3. The procedure of underwater modified strip biopsy. The forceps was passed through the snare.Figure 4. The polyp was grasped by forceps with underwater condition and was pulled out toward the lumen.Figure 5. The polyp was resected by cold snare polypectomy.Figure 6. After resection, it was confirmed endoscopically that there was no residual lesion.Figure 7. The pathology showed that the tumor was high-grade tubular adenoma, and the resection margins were unclear (pHMX, pVMX).
Discussion
GIF-2TQ260M is not widely available. It is a dual-channel, multi-bending scope available in Japan since July 2005. The scope has dual working channels and 2 bending sites (scope tip diameter 11.7 mm, channel diameter 3.2 mm/3.2 mm, working length 1030 mm). Although the endoscope is usually for upper GI tract, total colonoscopy was considered possible at the time of previous examination. Strip biopsy was originally a method in which normal saline is injected into the submucosa, which is then fixed with grasping forceps and resected by snare with an electric current.4^,^5 In this case, in addition to the advantage of the floating effect with underwater condition6 to confirm margin, the original strip biopsy was modified in that CSP was applied. Although endoscopic submucosal dissection and endoscopic full-thickness resection, including full-thickness resection device,7 could be other alternatives for polyps at the appendiceal orifice, safer en bloc resection is preferable, especially for small or no malignant lesions. Surgical resection including appendectomy with limited cecal resection is also too invasive for those lesions. As the safety of CSP has been demonstrated in several meta-analyses,8^,^9 forceps traction allowing a cold snare to be used was thought to contribute to reducing the risk such as perforation in this particular case. We have reported that underwater CSP for diminutive and small colorectal adenomas was safe and effective from the perspective of pathological complete resection.10 Using the floating effect under underwater conditions and using the strip biopsy technique can facilitate the elevation of lesions. As a result, it became easier to visualize the margins. This, in turn, contributed to a more reliable en bloc resection.
Conclusions
Underwater modified strip biopsy could be one of the options for the resection of colorectal polyp invading into the appendiceal orifice.
Disclosure
The authors disclosed no financial relationships relevant to this publication.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tarek H.H.James M.C.Appendix orifice polyps: a study of 691 lesions at a single institution Int J Colorectal Dis 3420197117183070138410.1007/s 00384-019-03251-z · doi ↗ · pubmed ↗
- 2Sukit P.Hiroyuki T.Supakij K.Difficult colorectal polypectomy: technical tips and recent advances World J Gastroenterol 292023260026153721339810.3748/wjg.v 29.i 17.2600 PMC 10198056 · doi ↗ · pubmed ↗
- 3Liselotte W.Z.Julius M.Bettina S.Adverse events of endoscopic full-thickness resection: results from the German and Dutch nationwide colorectal FTRD registry Gastrointest Endosc 9720237807893641044710.1016/j.gie.2022.11.005 · doi ↗ · pubmed ↗
- 4Tada M.Karita M.Yanai H.Development of strip-off biopsy (in Japanese with English abstract)Gastroenterol Endosc 261984833839
- 5Karita M.Tada M.Okita K.Endoscopic therapy for early colon cancer: the strip biopsy resection technique Gastrointest Endosc 371991128132203259610.1016/s 0016-5107(91)70669-x · doi ↗ · pubmed ↗
- 6Shiotsuki K.Imai K.Hotta K.Underwater endoscopic mucosal resection for complete R 0 removal of an adenoma extending deep into a colonic diverticulum Endoscopy 522020 E 374E 3753221979510.1055/a-1134-4668 · doi ↗ · pubmed ↗
- 7Yervant I.Mohammed B.Talal S.Endoscopic full-thickness resection of polyps involving the appendiceal orifice: a multicenter international experience Endoscopy 54202216243339571410.1055/a-1345-0044 · doi ↗ · pubmed ↗
- 8Shinozaki S.Kobayashi Y.Hayashi Y.Efficacy and safety of cold versus hot snare polypectomy for resecting small colorectal polyps: systematic review and meta-analysis Dig Endosc 3020185925992967585710.1111/den.13173 · doi ↗ · pubmed ↗