Rectal pulse granuloma: a rare condition presenting as a subepithelial lesion
Cong Yuan, Xue-Mei Lin, Chun-Hui Xi, Dan Sun, Xiao-Bo Wang, Guo-Dong Yang, Xian-Fei Wang

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
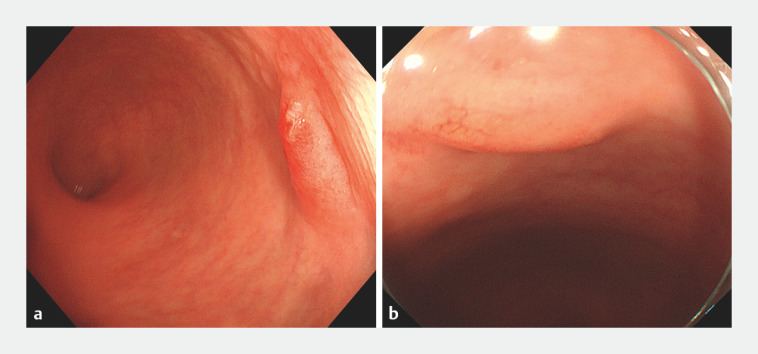 Fig. 1
Fig. 1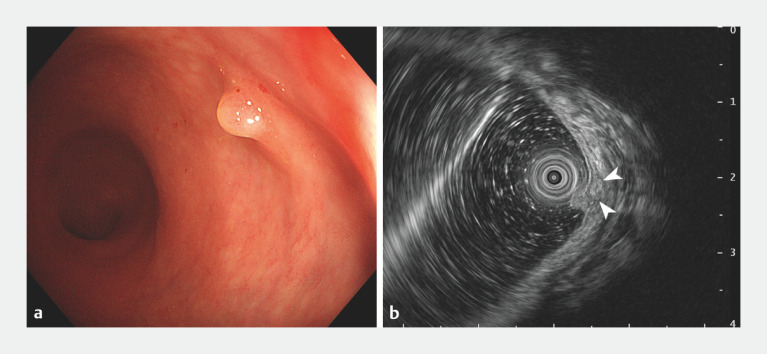 Fig. 2
Fig. 2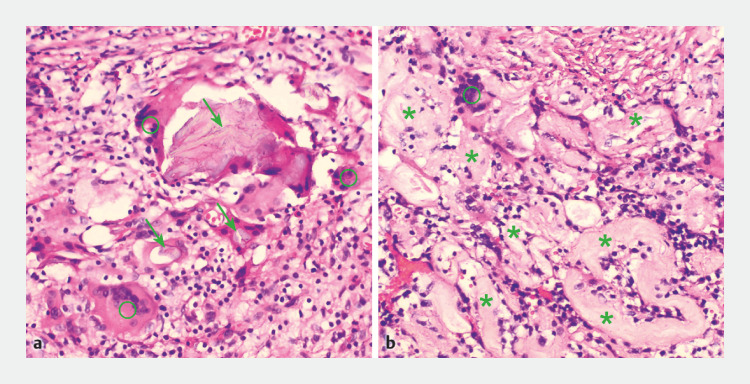 Fig. 3
Fig. 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTumors and Oncological Cases · Vascular Malformations and Hemangiomas · Oral and Maxillofacial Pathology
A pulse granuloma is a rare benign entity that typically occurs in the oral cavity 1 . Herein, we report a case of a subepithelial lesion (SEL) located in the distal rectum, which was diagnosed as a rectal pulse granuloma after its removal by endoscopic submucosal dissection (ESD).
A 66-year-old man with no significant medical history underwent colonoscopy for adenoma screening. Colonoscopy revealed multiple polyps, along with a subepithelial protrusion in the distal rectum, which was approximately 0.7 cm in size, with erosive changes of the overlying mucosa ( Fig. 1 a ). The patient underwent endoscopic polypectomy 1 week later, at which time the erosive mucosa was noted to have recovered completely ( Fig. 1 b ). After 10 weeks, the patient underwent further tests, with white-light endoscopy now showing an ill-defined submucosal bulge with a convex polyp on its surface ( Fig. 2 a ). Endoscopic ultrasound (EUS) revealed a 5.2 × 3.1-mm heterogeneous mass originating from the submucosal layer ( Fig. 2 b ). The lesion was removed by ESD ( Video 1 ). Histologic analysis revealed acute and chronic inflammatory cells, foreign-body giant cells, plant-like matter, and convoluted hyaline rings, supporting the diagnosis of a pulse granuloma with a foreign-body reaction ( Fig. 3 ), consistent with a pulse granuloma. The patient was discharged following ESD, without any complications.
Endoscopic images showing a distal rectal subepithelial lesion: a as a subepithelial protrusion with erosive changes of the overlying mucosa; b 1 week later, with no evidence of the erosive overlying mucosa.
Appearance of the lesion 10 weeks later on: a colonoscopy, showing an ill-defined submucosal bulge with a polyp on its surface; b on endoscopic ultrasonography, showing a 5.2 × 3.1-mm heterogeneous mass originating from the submucosal layer (arrowheads).
Histopathologic appearance of the resected lesion showing a granulomatous inflammatory process, with numerous foreign-body giant cells (circles), plant-like matter (arrows), and convoluted hyaline rings (stars), suggestive of a pulse granuloma (hematoxylin and eosin [H&E] staining, magnification × 200).
Endoscopic submucosal dissection of a subepithelial lesion initially seen as a subepithelial protrusion in the distal rectum on colonoscopy and confirmed to be originating from the submucosal layer on endoscopic ultrasound; histopathology of the resected specimen showed it to be a pulse granuloma.Video 1
Since it was first described in the lung in 1969 by Knoblich 2 , pulse granuloma has been reported in the oral and nasal cavity, skin, knee, fallopian tube and ovary, and intrahepatic portal vein 1 3 . It can also occur in the stomach, small intestine, colorectum, peritoneum, and mesentery 1 4 5 . A pulse granuloma is characterized by a chronic granulomatous reaction to a foreign body of vegetable origin 4 . In the present case, the mucosal damage seen above the lesion may have been the path by which the foreign bodies penetrated into the submucosal layer. As a rare lesion, familiarity with this entity’s distinctive histopathologic features may avoid a delayed diagnosis or misdiagnosis.
Endoscopy_UCTN_Code_CCL_1AD_2AG
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pereira TC Prichard JW Khalid M Rectal pulse granuloma Arch Pathol Lab Med 200112582282310.5858/2001-125-0822-RPG 11371241 · doi ↗ · pubmed ↗
- 2Knoblich R Pulmonary granulomatosis caused by vegetable particles. So-called lentil pulse pneumonia Am Rev Respir Dis 1969993803895812763 · pubmed ↗
- 3Yeo NK Eom DW Lim HW Vegetable or pulse granuloma in the nasal cavity Clin Exp Otorhinolaryngol 2014733433710.3342/ceo.2014.7.4.33425436056 PMC 4240494 · doi ↗ · pubmed ↗
- 4Fabro M Fabro S Rde Sales RS Pulse granuloma: a rare condition mimicking a gastric tumor Radiol Bras 20164927227310.1590/0100-3984.2015.005827777486 PMC 5073399 · doi ↗ · pubmed ↗
- 5Hayat M Rumman A Pulse granuloma: a rare gastric pseudotumor Am J Gastroenterol 202211770710.14309/ajg.000000000000163735020625 · doi ↗ · pubmed ↗