A cost benefit analysis of varicella vaccination in South Korea
Young Hwa Lee, Young June Choe

TL;DR
This study evaluates the cost-benefit of one-dose and two-dose varicella vaccination programs in South Korea, showing both are more cost-effective than no vaccination.
Contribution
The study provides the first economic evaluation of varicella vaccination in South Korea using updated local data.
Findings
One-dose and two-dose varicella vaccination programs both showed cost-benefit compared to no vaccination.
The one-dose program had a higher benefit-cost ratio (1.43) than the two-dose program (1.28).
Sensitivity analyses confirmed the robustness of the cost-benefit results.
Abstract
The introduction of varicella vaccination has significantly reduced the burden of chickenpox in many countries, but outbreaks still occur in populations with high vaccination coverage. To address this, some countries, including the United States, Germany, and Japan, have adopted a two-dose varicella vaccination recommendation. Economic evaluations are crucial for assessing vaccine recommendations; however, there are limited studies exist in Asian countries. Thus, our study aimed to evaluate the cost-benefit of one-dose and two-dose varicella vaccination programs compared to no vaccination in South Korea, incorporating updated data on disease burden and costs. We utilized data from South Korea’s health databases to estimate varicella burden and vaccination records. Decision tree analysis was employed to compare costs and benefits of vaccination strategies over a ten-year period for the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
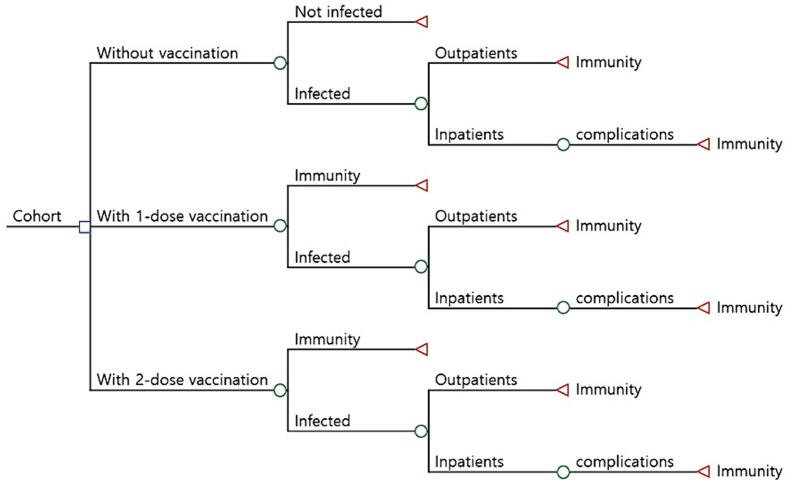 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHerpesvirus Infections and Treatments · Animal Virus Infections Studies · Vector-Borne Animal Diseases
Introduction
1
Since the introduction of varicella vaccine, the one-dose vaccination program has decreased the burden of chickenpox and its associated costs in many countries [1]. This program achieved a reduction of approximately 83 % in varicella cases compared to the pre-vaccination era, and a 66 % decrease in varicella-related deaths in the United States [2], [3]. Despite these achievements, varicella outbreaks persistently emerge in populations with high vaccination coverage, imposing significant health and economic burdens on public health [4]. To further mitigate the varicella disease burden, countries like U.S. [5], Germany [6], and Japan [7] have endorsed a routine two-dose varicella vaccination recommendation.
Economic evaluations play a pivotal role in assessing vaccine recommendations. Previous cost-effectiveness studies on one-dose varicella vaccination were based on pre-vaccination varicella health burdens, costs, vaccine efficacy, and vaccination coverage [8], [9]. They projected that a fully implemented varicella vaccination program would prevent 93 % of all cases, resulting in net costs to the healthcare system but overall savings for society [8]. Similar results were observed in other US-based studies [9], [10]. A recent study from Mexico concluded that universal varicella vaccination is cost-effective, with strategies involving one or two doses resulting in significant annual savings and reductions in disease burden over a 20-year period [11]. However, these assessments, conducted over different geographic regions, offer limited guidance for policy changes in Asian countries. They assumed higher reductions in disease incidence than observed, lacked updated data on varicella disease burden, vaccine effectiveness, and adverse events post-program implementation.
In South Korea, varicella vaccination has been recommended for children in high-risk groups since 1988 [12]. Subsequently, with the implementation of universal varicella vaccination through the National Immunization Program (NIP) in 2005, a single dose of varicella vaccine has been advised for all children aged 12–15 months. Among the available options, four live attenuated varicella vaccines exist, three of which are based on the Oka strain, while one is based on the MAV strain [1]. Since varicella became a notifiable infectious disease in July 2005, the Republic of Korea transitioned from using the pediatric communicable diseases sentinel surveillance system to a mandatory surveillance system. According to the Infectious Disease Control and Prevention Act, physicians treating varicella patients must report the cases to local public health centers within 24 h [13]. Additionally, public health centers are required to report these cases to the KDCA through municipal or provincial internet-based surveillance systems.
To inform policy decisions, we aimed to evaluate the cost-benefit of both one-dose and two-dose varicella vaccination programs in comparison to the absence of vaccination, incorporating updated disease burden estimates and costs for South Korea. We also analyzed the incremental benefit-cost and cost-effectiveness ratios of the second dose. Ultimately, the objective was to provide decision-makers with evidence-based recommendations to improve varicella control and prevent outbreaks in South Korea.
Methods
2
We utilized data from the Health Insurance Review and Assessment Service (HIRA) linked with immunization registry in South Korea. Covering over 98 % of the Korean population, national health insurance operates as a single-payer system, providing comprehensive medical information, including sociodemographic characteristics, from both inpatient and outpatient records nationwide. Claim data diagnosed as varicella (ICD-10, B01) from the Health Insurance Review and Assessment Service (HIRA) database between 2012 and 2022 for the cohort born in 2012 were used to estimate the burden of varicella disease, along with the vaccination records collected from the National Infectious Diseases Surveillance database run by the Korea Disease Control and Prevention Agency (KDCA). The KDCA contributed immunization registry data, encompassing vaccination details, diagnosis dates, series, and vaccine types.
Annual incidence rates and hospitalization rates of the one-dose and two-dose vaccinated and medical treatment costs were calculated from this data, however, the incidence rates of the unvaccinated were obtained from the US study conducted by Zhou et al.(2008) [10], because, after the introduction of the national universal one-dose varicella vaccination program in 2005, there were only a small number of unvaccinated children in South Korea, 12,139 (2.8 %) of the total 484,047, being likely to have unusual medical characteristics or already infected prior to vaccination.
To compare the costs and benefits between 2022 and 2032 of the three varicella vaccination strategies for the 2022 birth cohort of 277,401 children – no vaccination, one-dose vaccination (at 12–15 months old) and two-dose vaccination (at 4–6 years old), a decision tree analysis was employed (Fig. 1). In the decision tree, a child could be vaccinated one or two times, or not vaccinated. After vaccination, he or she could get infected with varicella according to the effectiveness of vaccine or not. The annual incidence rates by ages assumed in this study were shown in Table 1. If infected, he or she could have moderate symptoms and be treated as an outpatient or could have severe symptoms with complications such as pneumonia, encephalitis, meningitis and keratitis and be hospitalized as an inpatient. The hospitalization rates assumed in this study were shown in Table 2. Direct costs were calculated as costs for services and materials and indirect costs were estimated by using the capital approach – time and wage, along with transportation fares. Outpatient, inpatient, prescription costs were included in medical treatment costs, and these were assumed to be the same in regardless of the vaccination status. Vaccination costs were calculated by using the proportion of administration between public and private sector from our data, due to the difference of procurement costs. These estimated costs were shown in Table 3. Benefits were calculated as the saving costs of reduced varicella cases. All values were evaluated as discounted present value of 2022. The values of time taken for vaccination, inpatient, outpatient and travel, and transport fares were obtained from Korea Health Panel (2008) [14]; wages and economic activity participation rate were from The Economically Active Population Survey (the Ministry of Employment and Labor, 2022) [15]; price indices for health and transport were from The Consumer Price Survey (Statistics Korea, 2022) [16].Fig. 1. Simplified decision tree.Table 1. Varicella annual incidence rates with and without vaccination (2012 birth cohort).Age (year)Unvaccinated†1-dose Vaccinated2-dose Vaccinated055.6−−198.45.23.5298.417.310.4398.419.010.0498.425.810.2581.235.710.1681.237.39.3781.228.58.3881.27.33.2981.23.92.31019.13.81.7Total874.3183.869.0*Data are varicella cases per 1,000 population.†Data from JID 2008:197 (Suppl 2), Zhou et al.Table 2. Probabilities of hospitalizations rates.Unvaccinated1-dose Vaccinated2-dose VaccinatedOutpatients94.398.399.1In patients5.71.70.9Total100.0100.0100.0Table 3Direct costs and indirect costs for varicella-related events (per case).Direct costIndirect costTotal Cost(direct + indirect)InpatientsMedical treatment cost832.3500.3OutpatientsMedical treatment cost35.943.0Vaccine cost a^,^b^,^c24.615.440.0Public11.512.023.5Private27.016.043.0aProportion of vaccination facility: public (public health center) 15.1 %, private (hospital, clinic) 84.9 %.bExchange rate, 1,250 Korean won for one US dollar.cDirect vaccination costs were collected from 「Infectious Disease Control And Prevention Act」, Korea Disease Control and Prevention Agency, 2022.8.5. Prive cost consists of public cost and actual medical expense.
Sensitivity analyses were performed to assess the effect on the benefit-cost ratios (BCRs) by varying variables such as vaccine coverage rate, vaccine effectiveness, hospitalization rate, price of vaccine, and discount rate. The ranges of each variable were assumed to reflect the real world in South Korea.
Results
3
Estimated costs and benefits for the 2022 birth cohort of 277,401 children over 10 years were summarized in Table 4. If no vaccination program is implemented, there will be 220,222 varicella cases and 2.0 million for one-dose vaccination program and 17,359 cases and 9.6 million, 173,900 cases would be decreased and 17.9 million, 202,863 cases would be prevented and 8.3 million and only would only save 15,712,968.91,957,278.5630,242.1Direct costs of varicella14,722,794.11,854,636.0598,534.2Indirect costs of varicella990,174,8102,642.431,707.8 1- or 2-dose vs. unvaccinatedCases prevented, no.173,900202,863Cases prevented, %79.0 %92.1 %Cost of vaccination, 12,868,158.114,124,259.3Savings in indirect costs, 13,755,690.415,082,726.8Direct BCR2.181.28Total BCR1.430.84Total net present value (net saving), 23.913.9 2-dose vs. 1-doseCases prevented, no.28,963Cases prevented, %62.5 %Cost of vaccination, 1,256,101.8Savings in indirect costs, 1,327,036.4Direct BCR0.25Total BCR0.16Total net present value (net saving), −240.6*Exchange rate, 1,250 Korean won for one US dollar.
Sensitivity analyses for the total BCR for the vaccination strategies showed that almost similar result as the above base case. Being compared with no vaccination program, one-dose vaccination program was cost-benefit, except for cases where vaccine effectiveness drops to 13.0 %, the effectiveness of one-dose varicella vaccine in South Korea [17], or proportion of inpatients drops to 1.7 %. Two-dose vaccination is not cost-benefit than one-dose vaccination in any given conditions. The total BCR of the two-dose vaccination versus no vaccination maintains the range between 0.50 and 1.41; The total BCR could be larger than 1.00 if proportion of inpatients increases or vaccine cost drops, significantly. Vaccine coverage rate and discount rate had little impact on the total BCR (Table 5).Table 5. Sensitivity analysis for relevant parameters.VariableBase-caseRangeTotal BCR1 vs 02 vs 02 vs 1Vaccine coverage rate100 %95–100%1.43–1.510.84–0.890.16–0.17 Vaccine effectiveness1-dose vaccination79.0 %13.0–92.1 %0.79–1.56(0.84)0.01–0.902-dose vaccination92.1 %79.0–99.0 %(1.43)0.78–0.870.03–0.23 Proportion of inpatientsUnvaccinated5.7 %1.7–10.0 %0.79–2.120.50–1.21(0.16)1-dose vaccination1.7 %0.9–3.0 %1.39–1.46(0.84)0.13–0.212-dose vaccination0.9 %0.5–1.7 %(1.43)0.840.15–0.17Vaccine cost, $41.524.0–56.01.02–2.390.60–1.410.11–0.27Discount rate5 %3–7 %1.35–1.520.82–0.870.16
Discussion
4
This study highlights the substantial societal cost savings and high benefit-cost ratios associated with both one-dose and two-dose varicella vaccination programs compared to no vaccination program in South Korea. The one-dose program yields approximately 1.43 saved for every dollar spent. Similarly, the two-dose program results in approximately 1.28 saved for every dollar spent. These findings demonstrate the favorable benefit-cost ratio of varicella vaccination programs, achieving significant public health benefits by reducing morbidity associated with varicella, while also generating substantial cost savings. Our research aligns with economic analyses conducted in the U.S., indicating that compared to no vaccination, both the one-dose program (with a societal BCR of 4.37) and the two-dose program (BCR of 2.73) are estimated to be cost-saving from a societal perspective; however, when compared to the one-dose program, the incremental addition of a second dose does not yield cost savings (societal incremental BCR of 0.56) [10]. The findings may vary depending on the country's epidemiological context, healthcare expenses, consideration of herpes zoster impact, and the type of vaccine formulation (e.g., standalone varicella vaccine versus combination with measles-mumps-rubella vaccine). Research conducted in the UK suggests that introducing a 2-dose universal varicella vaccination is a cost-effective option compared to no vaccination, despite differences in healthcare costs compared to the US, and the use of the MMR-V combination vaccine [18]. Although South Korea has low medical care costs [19], and is densely populated [20], and despite the absence of MMR-V formulations, our results should be interpreted within the context of the country when compared to others. Nevertheless, the findings indicate a net economic benefit of the varicella program.
While the economic analysis indicates that the second-dose varicella vaccination was not cost-saving compared to the one-dose program, the decision to recommend a routine two-dose vaccination program in the U.S. considered various factors beyond cost-effectiveness [10], [21]. These included ongoing disease burden, transmission dynamics, the potential for severe disease and transmission to high-risk individuals, as well as the demonstrated efficacy of the second dose in enhancing immunity and disease protection [22], [23], [24]. Such factors should be also considered in the Korean context. A national cohort study conducted in Korea evaluated the efficacy of one-dose and two-dose varicella vaccination against laboratory-confirmed varicella [25]. The study revealed a vaccine effectiveness (VE) of 16.8 % for one-dose vaccination, while two-doses showed a VE of 98.6 %. In another study, within the 2011 birth cohort comprising 421,070 newborns, one-dose vaccination demonstrated a VE of 86.1 % in the first year and 49.9 % over a 6-year follow-up, indicating a 7.2 % annual decline [26]. A dynamic transmission model, calibrated using age-specific varicella incidence data and vaccine coverage in Korea, revealed moderate effectiveness of the single-dose vaccine [27]. In the scope of vaccinology, where primary failure played a crucial role in breakthrough infections among children who received only one dose, it is essential to discuss the potential benefits of implementing a two-dose vaccination strategy for public health purposes. A 2012–2013 cross-sectional seroepidemiological study in Korea found that while overall varicella seroprevalence was high, it was significantly lower in adolescents aged 10–19 compared to older age groups, highlighting the need for strategies to enhance varicella immunity in teenagers. [28].
This study had several limitations. Due to the lack of varicella incidence data before the introduction of the national vaccination program, such as the incidence rates of the unvaccinated, that this study may not fully reflect the exact epidemiologic conditions of the unvaccinated in Korea. Furthermore, the change in the varicella vaccine distributed in Korea was not considered. The vaccine used mainly in the 2012 birth cohort used in this study is not currently distributed. As a result, there may be changes in incidence and hospitalization rates due to the use of a different vaccine from the past. Moreover, it is important to acknowledge that our analysis does not account for potential vaccine adverse reactions, which may impact the overall cost-effectiveness assessment. In addition, we acknowledge the potential for underreporting in our study, which may affect the accuracy of our estimates and should be considered when interpreting the results. A study found that the recent increase in reported varicella cases is influenced by improved reporting after varicella was included in the NIP system [29]. Despite these limitations, our study provides valuable insights into the costs and benefits of such a strategy. While our model may serve as a template for other countries considering varicella vaccination programs, it's crucial to adapt the analysis to each country's unique healthcare delivery setting and epidemiological context. Our sensitivity analysis underscores the importance of discount rates and vaccine prices in determining the cost-benefit of the second dose. Overall, the findings underscore the importance of vaccination in reducing the burden of varicella disease and improving public health outcomes.
In conclusion, our findings suggest that implementing either a one-dose or two-dose varicella vaccination – when considering direct BCR – regimen could result in cost reductions and improved cost-benefit compared to no vaccination. This indicates that allocating resources to varicella vaccination programs could result in considerable advantages, both in terms of economic savings and public health outcomes.
CRediT authorship contribution statement
Young Hwa Lee: Writing – review & editing, Writing – original draft, Resources, Project administration, Methodology, Investigation, Funding acquisition, Formal analysis, Data curation, Conceptualization. Young June Choe: Writing – review & editing, Writing – original draft, Visualization, Validation, Supervision, Conceptualization.
Declaration of competing interest
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: Young June Choe reports financial support was provided by SK Bioscience Co Ltd. If there are other authors, they declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lee Y.H.Choe Y.J.Lee J.Kim E.Lee J.Y.Hong K.Global varicella vaccination programs Clin Exp Pediatr 6520225555623645719810.3345/cep.2021.01564 PMC 9742762 · doi ↗ · pubmed ↗
- 2Nguyen H.Q.Jumaan A.O.Seward J.F.Decline in mortality due to varicella after implementation of varicella vaccination in the United States N Engl J Med 35220054504581568958310.1056/NEJ Moa 042271 · doi ↗ · pubmed ↗
- 3Seward J.F.Watson B.M.Peterson C.L.Mascola L.Pelosi J.W.Zhang J.X.Varicella disease after introduction of varicella vaccine in the United States, 1995–2000 JAMA 28720026066111182969910.1001/jama.287.5.606 · doi ↗ · pubmed ↗
- 4Lopez A.S.Guris D.Zimmerman L.Gladden L.Moore T.Haselow D.T.One dose of varicella vaccine does not prevent school outbreaks: is it time for a second dose?Pediatrics 1172006 e 1070 e 10771674080910.1542/peds.2005-2085 · doi ↗ · pubmed ↗
- 5Marin M.Meissner H.C.Seward J.F.Varicella prevention in the United States: a review of successes and challenges Pediatrics 1222008 e 744e 7511876251110.1542/peds.2008-0567 · doi ↗ · pubmed ↗
- 6Siedler A.Rieck T.Tolksdorf K.Strong additional effect of a second varicella vaccine dose in children in Germany, 2009–2014 J Pediatr 1732016202206.e 22699570310.1016/j.jpeds.2016.02.040 · doi ↗ · pubmed ↗
- 7Hattori F.Kozawa K.Miura H.Kawamura Y.Higashimoto Y.Yoshikawa A.Trend in varicella patients 4 years after implementation of universal two-dose varicella vaccination in Japan Vaccine 382020733173363300867110.1016/j.vaccine.2020.09.038 · doi ↗ · pubmed ↗
- 8Lieu T.A.Cochi S.L.Black S.B.Halloran M.E.Shinefield H.R.Holmes S.J.Cost-effectiveness of a routine varicella vaccination program for US children JAMA 27119943753818283587 · pubmed ↗