Aortic Valve Infective Endocarditis Complicated by Annular Abscess: Antibiotics in the Abscess Cavity
Zaki Haidari, Shehla Ufaq Ahmad, Stephan Knipp, Iskandar Turaev, Mohamed El Gabry

TL;DR
This study examines whether using local antibiotics in abscess cavities during surgery for aortic valve endocarditis reduces recurrence and improves outcomes.
Contribution
The study evaluates the effectiveness of local antibiotic use in preventing recurrent endocarditis after surgical treatment of annular abscesses.
Findings
Local antibiotics in the abscess cavity did not reduce the rate of recurrent endocarditis.
There was no significant difference in reoperation rates between the groups.
Mortality rates were similar in both the local antibiotic and control groups.
Abstract
Objectives: Infective endocarditis of the aortic valve complicated by annular abscess is a challenging problem and often requires patch reconstruction after surgical debridement of the abscess cavity. Filling the remaining cavity with antibiotics is advocated to prevent recurrent endocarditis. This study aimed at evaluating the role of local antibiotics in patients with aortic valve infective endocarditis complicated by annular abscess. Methods: Between January 2012 and December 2021, all consecutive patients with aortic valve infective endocarditis complicated by annular abscess undergoing cardiac surgery and annular patch reconstruction were included. Patients receiving local antibiotics were compared with patients without local antibiotics. The primary endpoints were the incidence of recurrent endocarditis, re-operation, and mortality during two-year follow-up. Results: A total of 41…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
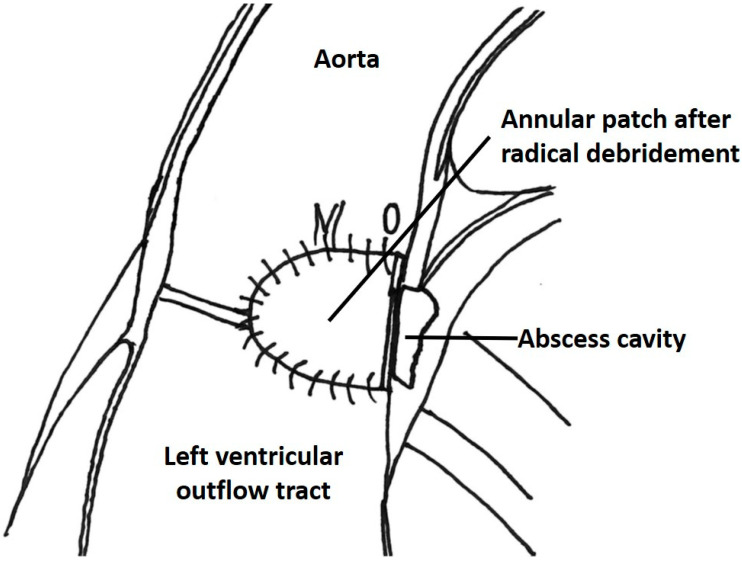 Figure 1
Figure 1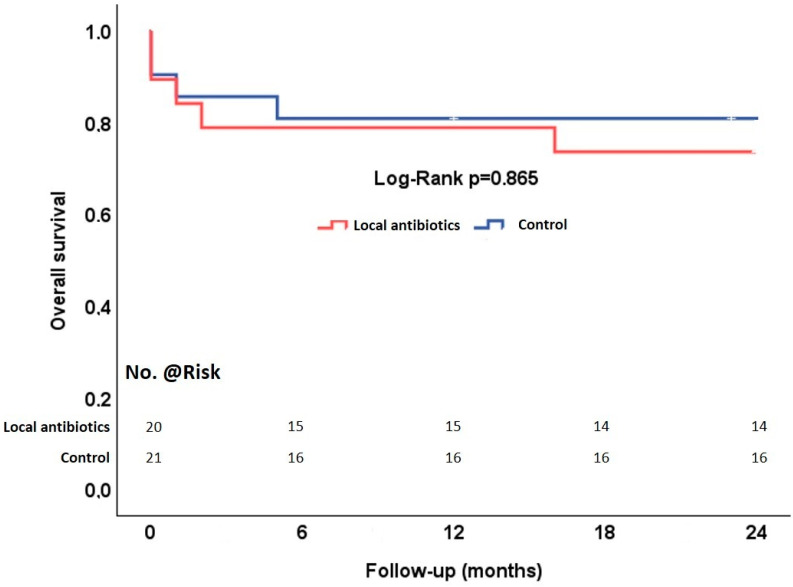 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfective Endocarditis Diagnosis and Management · Streptococcal Infections and Treatments · Infectious Aortic and Vascular Conditions
1. Introduction
Cardiac surgery in patients with aortic valve infective endocarditis is associated with increased mortality and morbidity [1], especially in complicated cases such as annular abscess [2,3]. Radical surgical debridement of the abscess cavity is necessary to prevent recurrent endocarditis [4]. However, radical surgical debridement can result in tissue defects leading to the necessity for annular patch reconstruction to anchor a prosthetic valve. Additionally, the application of local antibiotics in the remaining abscess cavity has been proposed to prevent recurrence of infective endocarditis [5,6,7] and improve outcome [8]. In this study, we aimed to evaluate the effect of local antibiotic application in the remaining abscess cavity on clinical outcome in patients with aortic valve infective endocarditis complicated by annular abscess and a need for annular patch reconstruction.
2. Materials and Methods
2.1. Patients
Eligible candidates for this retrospective comparative study were patients with definitive infective endocarditis [9] of the aortic valve undergoing cardiac surgical therapy from January 2012 to December 2021. Out of these, 71 patients were found to have annular abscess receiving annular patch reconstruction. Annular abscess was defined as paravalvular cavity with infectious or necrotic tissue in the aortic annulus or root, or as aortoventricular discontinuity. Patients undergoing replacement of the intervalvular fibrous body were excluded. The study was reviewed and approved by the institutional ethics committee (Protocol number: 23-11446-BO, approval date: 28 September 2023) and written informed consent was waived due to retrospective study design.
2.2. Surgical Technique
Standard aortic and caval cannulation techniques were applied. Cardioplegic arrest was achieved by crystalloid cardioplegia (Custodiol, Dr. Franz Koehler Chemie, Bensheim, Germany). After resection of the infected aortic valve leaflets, the aortic annulus was inspected for the presence of abscess. In cases with annular abscess, the abscess cavity was opened and all macroscopically infected tissue was removed. After irrigation with diluted povidone–iodine solution, the defect was excluded with autologous or bovine pericardial patch, respectively (Figure 1). Application of local antibiotics in the remaining abscess cavity was at the discretion of the operating surgeon. In cases with local antibiotics, the remaining cavity was filled with a mixture of antibiotic (dependent on the causative microorganism antibiogram) and fibrin glue before the closure of the defect. Finally, aortic valve replacement was performed. Concomitant procedures were performed as indicated. All instruments, synthetic material, and prostheses were soaked in vancomycin solution during operations.
2.3. Postoperative Care
Postoperatively, all patients were transferred to the cardiac surgical intensive care unit (ICU) with invasive hemodynamic monitoring and guideline-directed antibiotic and supportive therapy. Follow-up was conducted by outpatient visits or telephone follow-up, and data on survival and valve-related complications were collected.
2.4. Endpoints
The primary endpoints of the study were the incidence of recurrent infective endocarditis, reoperation, and mortality at two-year follow-up. Recurrent infective endocarditis was defined as relapse or reinfection according to guidelines. Secondary endpoints included postoperative organ failure (circulatory, pulmonary and renal), and ICU and hospital stay.
2.5. Statistical Analysis
SPSS software version 29 (SPSS Inc., Chicago, IL, USA) was used to analyze the data. Continuous variables were reported as median and interquartile range (IQR) and compared with the Mann–Whitney test. Categorical data were expressed as number of patients and frequencies and compared using the chi-square or Fisher exact test. Kaplan–Meier curves were employed to evaluate overall survival rates and the two groups were compared using the log-rank test. A p-value < 0.05 was considered statistically significant.
3. Results
3.1. Baseline Characteristics
From January 2012 through December 2021, 211 patients underwent cardiac surgery for infective endocarditis of the aortic valve. In 79 (34%) patients, an annular abscess was found by intraoperative inspection. A patch reconstruction of the aortic annulus was performed in 41 patients. In 20 patients, a mixture of antibiotics and fibrin glue was used to fill the remaining abscess cavity. In the remaining 21 patients (control group), the abscess cavity was left empty. The preoperative demographics and clinical and inflammatory status of the two groups are given in Table 1. The most commonly identified causative microorganism for infective endocarditis (Table 2) was staphylococcus aureus. The most common location of the annular abscess was at the level of the non-coronary cusp insertion (Table 3). There were no significant differences in demographics, hemodynamic, and pulmonary status, the levels of preoperative inflammatory parameters, causative microorganism or location of the abscesses between the two groups.
3.2. Operative Characteristics
Table 4 presents the operative characteristics of the two groups. All patients underwent at least aortic valve replacement. In the control group, three patients underwent aortic root replacement using a conduit. Concomitant valvular procedures were performed more frequently in the control group, without statistical significance. Concomitant coronary artery bypass grafting was performed in six patients, four in the local antibiotics group, and two in the control group (p = 0.41). Cardiopulmonary bypass and aortic cross-clamp times were longer in the local antibiotics group but did not reach statistical significance.
3.3. Endpoints
The endpoints are summarized in Table 5. Thirty-day mortality was 12% overall, 15% in the local antibiotics group, and 10% in the control group (p = 0.66). The causes of early mortality were septic multiorgan failure in three cases and cardiac failure in two cases. Two-year mortality increased to 27% overall, 30% in the local antibiotics group, and 24% in the control group (Figure 2). Recurrent infective endocarditis occurred in one patient in the local antibiotics group and in one patient in the control group (p > 0.99). Both patients underwent reoperation. The time interval between the index operation and the recurrence of infective endocarditis in the local antibiotics group was 19 months and 40 days in the control group.
The incidence of postoperative organ failure (circulatory, respiratory and renal) requiring (temporary) support or replacement did not differ between the two groups. There were also no differences in the ICU and hospital stay between the groups.
4. Discussion
Annular abscess remains a frequent complication of aortic valve infective endocarditis and requires surgical debridement. The subsequent tissue defect often requires patch reconstruction to anchor the valve prosthesis and to exclude the remaining cavity from the circulation. In this study, we evaluated the effect of applying local antibiotics in the remaining abscess cavity on outcome, especially on the rate of recurrent infective endocarditis. We found that the rate of recurrent infective endocarditis is low after radical surgical debridement and annular patch reconstruction and that the application of local antibiotics did not affect the recurrence rate or survival during two-year follow-up.
Annular abscess is strictly a consequence of an uncontrolled infection causing a mycotic aneurysm of the sinuses of Valsalva. Uncontrolled infection can also result in fistulous communication between the aortic root and the left ventricular outflow tract (paravalvular aortic regurgitation) or to other cardiac chambers such as the right atrium and the right ventricle (Gerbode defect). Suspicion of abscess formation should rise with regards to any patient with aortic valve endocarditis on guideline-directed antibiotics and persistent fever, elevated inflammatory parameters, or cutaneous or embolic phenomena. Other signs of annular abscess include prolongation of PR interval or development of complete heart block. Multimodality imaging plays an important role when evaluating a patient with aortic valve infective endocarditis complicated by annular abscess [10].
The prevalence of aortic valve infective endocarditis complicated by annular abscess varies between 12% and 50% [11,12,13]. Abscess formation is an independent predictor of short-term mortality and is reported to be twice as high compared to patients without annular abscess [1]. Furthermore, recurrent infective endocarditis is higher in patients with annular abscess compared to patients without annular abscess [14]. Therefore, it is of crucial importance to eradicate infection by radical surgical debridement and exclusion by patch reconstruction. The addition of local antibiotics in the remaining abscess cavity has been suggested to prevent recurrence. In addition, the risk of residual infected tissue seems to be low after radical surgical debridement. Furthermore, a mixture of antibiotics with fibrin glue in the remaining excluded abscess cavity may only provide temporary protection against reactivation of infection. Moreover, the presence of fibrin glue may impede the penetration of antibiotics in the surrounding tissue, mitigating the effect of such therapy. Although local antibiotics showed effectivity in the prevention of sternal wound infection [15], development of antibiotic-eluting or bacterial-resistant patches and valvular prosthesis may be a more effective strategy in the prevention of recurrent infective endocarditis in this high-risk population [16,17,18,19].
In this study, we selected only patients in whom a patch reconstruction was performed. Patients with small annular abscesses were treated by direct closure of the abscess cavity. The cohort comprises high-risk patients with large annular abscesses, who required patch reconstruction. The control group included three patients with additional aortic root replacement in which local antibiotics could not be applied. Exclusion of these patients did not change the outcome. Therefore, we decided not to exclude these patients from the analysis.
5. Limitations
To our best knowledge, this is the first study evaluating the role of local antibiotics in aortic valve infective endocarditis complicated by annular abscess. Although the baseline demographics, clinical and inflammatory status and operative characteristics of the two groups were comparable, bias cannot completely be excluded due to retrospective study design and limited sample size. Therefore, larger and randomized controlled studies are required before definitive conclusions can be drawn.
6. Conclusions
Local antibiotics in the remaining abscess cavity after radical debridement and patch reconstruction of the aortic annulus in patients with aortic valve infective endocarditis seems not to reduce the rate of recurrent endocarditis, reoperation, or mortality.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Habib G. Erba P.A. Iung B. Donal E. Cosyns B. Laroche C. Popescu B.A. Prendergast B. Tornos P. Sadeghpour A. Clinical presentation, aetiology and outcome of infective endocarditis. Results of the ESC-EORP EURO-ENDO (European infective endocarditis) registry: A prospective cohort study Eur. Heart J.2019403222323210.1093/eurheartj/ehz 62031504413 · doi ↗ · pubmed ↗
- 2Leontyev S. Davierwala P.M. Krögh G. Feder S. Oberbach A. Bakhtiary F. Misfeld M. Borger M.A. Mohr F.W. Early and late outcomes of complex aortic root surgery in patients with aortic root abscesses Eur. J. Cardiothorac. Surg.20164944745510.1093/ejcts/ezv 13825870220 · doi ↗ · pubmed ↗
- 3David T.E. Regesta T. Gavra G. Armstrong S. Maganti M.D. Surgical treatment of paravalvular abscess: Long-term results Eur. J. Cardiothorac. Surg.200731434810.1016/j.ejcts.2006.10.03617140802 · doi ↗ · pubmed ↗
- 4Delgado V. Ajmone Marsan N. de Waha S. Bonaros N. Brida M. Burri H. Caselli S. Doenst T. Ederhy S. Erba P.A. 2023 ESC Guidelines for the management of endocarditis Eur. Heart J.2023443948404210.1093/eurheartj/ehad 19337622656 · doi ↗ · pubmed ↗
- 5Farhat F. Durand M. Delahaye F. Jegaden O. Prosthetic valve sewing-ring sealing with antibiotic and fibrin glue in infective endocarditis. A prospective clinical study Interact. Cardiovasc. Thorac. Surg.20076162010.1510/icvts.2006.14488117669758 · doi ↗ · pubmed ↗
- 6Karck M. Siclari E. Wahlig H. Sperling U. Schmid C. Haverich A. Pretreatment of prosthetic valve sewing-ring with the antibiotic/fibrin sealant compound as a prophylactic tool against prosthetic valve endocarditis Eur. J. Cardiothorac. Surg.1990414214610.1016/1010-7940(90)90185-32139788 · doi ↗ · pubmed ↗
- 7Mc Giffin D.C. Davies J.E. Kirklin J.K. Reconstructing the infected aortic root with antibiotic impregnated biological glue J. Card. Surg.20142934034210.1111/jocs.1229224433228 · doi ↗ · pubmed ↗
- 8Watanabe G. Haverich A. Speier R. Dresler C. Borst H.G. Surgical treatment of active infective endocarditis with paravalvular involvement J. Thorac. Cardiovasc. Surg.199410717117710.1016/S 0022-5223(94)70466-X 8283880 · doi ↗ · pubmed ↗