Deciphering the Reactivity of Autoantibodies Directed against the RNP-A, -C and 70 kDa Components of the U1-snRNP Complex: “Double or Nothing”?
Daniel Bertin, Benjamin Babacci, Alexandre Brodovitch, Cléa Dubrou, Xavier Heim, Jean Louis Mege, Nathalie Bardin

TL;DR
This study explores how different autoantibodies against the U1-snRNP complex can help distinguish between mixed connective tissue disease and systemic lupus erythematosus.
Contribution
The study introduces the RNP index as a more informative diagnostic tool for MCTD versus SLE.
Findings
The RNP index showed higher sensitivity and specificity for MCTD compared to SLE.
No preferential association of IgG or IgM autoantibodies was found between SLE and MCTD.
Analyzing autoantibody proportions in U1-snRNP is more informative than analyzing individual autoantibodies.
Abstract
Background: The positivity of anti-RNP autoantibodies as biological criteria for the diagnosis of mixed connective tissue disease (MCTD) has recently divided the rheumatology community. Autoantigenicity of the U1-snRNP complex tends to generate multiple autoantibodies against RNP-A, -C and -70 KDa or Sm proteins. The aim of this study is to identify the most informative autoantibodies in clinical practice, in particular, to contribute to differential diagnosis between MCTD and systemic lupus erythematosus (SLE). Methods: Sera from 74 patients positive for anti-RNP autoantibodies were selected over a period of one year of laboratory practice. Autoantibodies directed against extractable nuclear antigen, RNP proteins (A, C, 70 KDa) and 40 kDa fragments of RNP-70 KDa were investigated by using quantitative fluoroenzymatic assay and Western blot analysis. Results: Among the 74 patients, 40…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
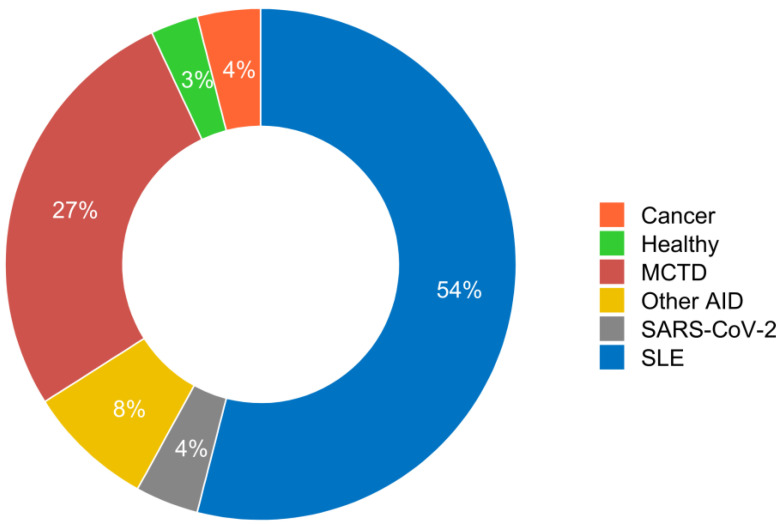 Figure 1
Figure 1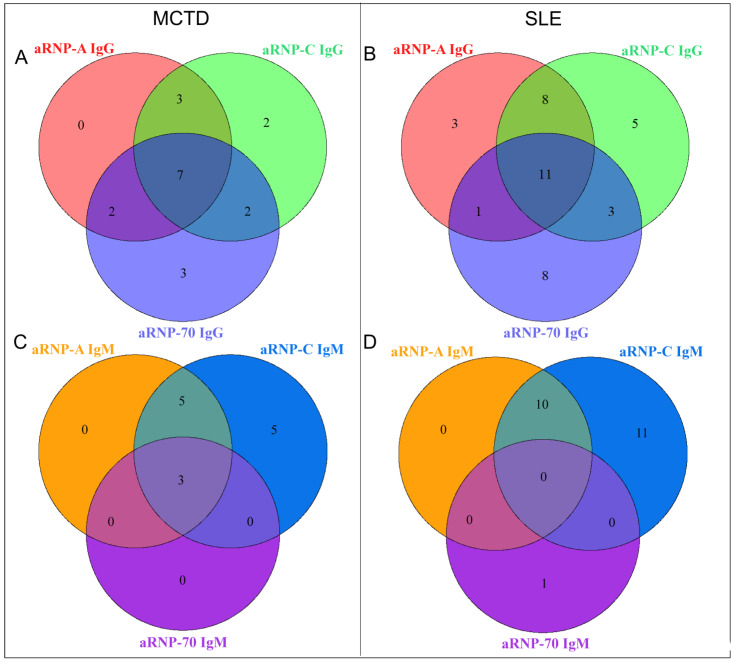 Figure 2
Figure 2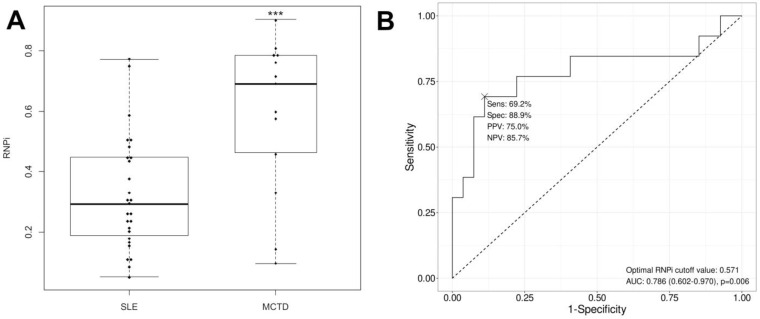 Figure 3
Figure 3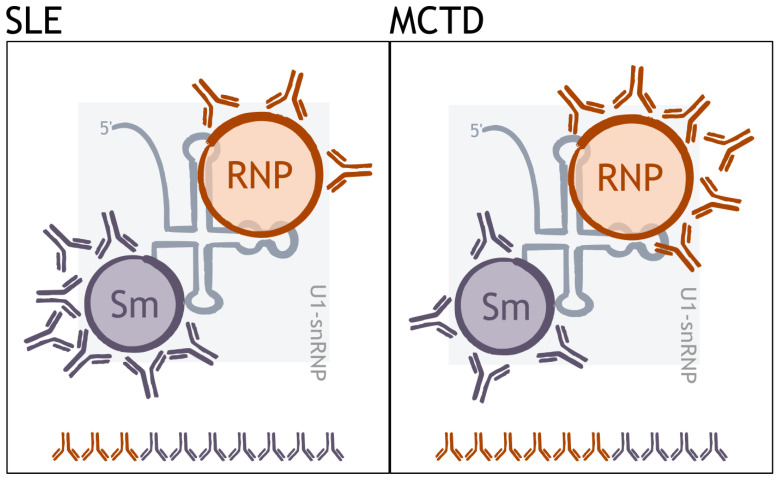 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSystemic Lupus Erythematosus Research · Viral Infections and Immunology Research · Inflammatory Myopathies and Dermatomyositis
1. Introduction
The diagnosis of mixed connective tissue disease (MCTD) remains a major challenge today. Autoantibodies directed against RNP (anti-RNP) and against Sm (anti-Sm), which belong to the family of antinuclear autoantibodies (ANAs), are of paramount importance in clinical practice. Hence, the positivity of anti-RNP is the only biological criterion for mixed connective tissue disease (MCTD) [1], but it is also detected in other autoimmune diseases such as systemic lupus erythematosus (SLE), scleroderma (SSc), Gougerot-Sjögren syndrome (GSS), rheumatoid arthritis (RA) and polymyositis/dermatomyositis (PM/DM) [2]. Anti-Sm are included in the serological criteria of SLE [3] because of their high specificity.
These autoantibodies are directed against small nuclear molecules formed by the association between polypeptides and ribonucleic acid. Anti-RNP interacts with proteins (70 kDa, A, C) that are associated with U1-RNA and Sm proteins to form U1 small nuclear ribonucleoprotein (U1-snRNP) [4]. Anti-Sm antibodies are directed against seven proteins, including B, B’ and D3, which form the common core of small nuclear ribonucleoprotein particles. RNPs are components of the spliceosome, an RNP complex composed of the five snRNPs [5]. The spliceosome is involved in the splicing of precursor mRNA (pre-mRNA) into mature mRNA, ready for translation into proteins. The targets of anti-RNP consist of three proteins, i.e., RNP-70, RNP-A and RNP-C, with some structural and functional differences. Briefly, RNP-70 presents a greater length. Both RNP-A and RNP-70 are capable of direct RNA binding because, unlike RNP-C, they possess an RNA recognition motif [6]. In terms of their functions, RNP-70 initiates spliceosome assembly by early binding to the 5′ splice site of the pre-mRNA and also allows RNP-C to bind to the U1-RNP. RNP-A modulates the initiation of polyadenylation while RNP-C allows for the formation of a transient complex of the spliceosome and stabilizes the RNA/U1-snRNP interaction [7]. During apoptosis, RNP-70 is specifically cleaved by the enzyme caspase-3, resulting in a C-terminally truncated 40 kDa fragment [8,9] which can be targeted by autoantibodies that are more specifically associated with MCTD than other anti-RNP-70 autoantibodies [10].
Several classification criteria have been proposed for the diagnosis of MCTD, all of which include the detection of anti-RNP as the sole serological criterion [1,11,12]. However, the following question remains: what is the added value of subtyping anti-RNP autoantibodies?
According to clinical interest, the detection of anti-RNP is currently carried out in the immunology laboratory and includes an analysis step by indirect immunofluorescence followed, if positive, by the identification of the nuclear target [13,14]. Routinely, anti-RNP autoantibodies are directed against a mixture of RNP-70, RNP-A and RNP-C and belong to the IgG isotype, which is the one usually analyzed [15]. The interest of subtyping anti-RNP autoantibodies for a faster and more specific diagnosis has not yet been established because of conflicting studies in the literature.
The aim of this study was to test and identify the most contributory anti-RNP autoantibodies subtype in clinical practice, especially to aid in the differential diagnosis between MCTD and SLE. The results were then analyzed in relation to the patients’ clinical and immunological data.
2. Material and Methods
2.1. Patients
All patients with suspected autoimmune diseases who were referred for ANA testing to the Immunology Laboratory of the University Hospital of Marseille between 1 February 2020 and 1 February 2021, and who were positive for IgG anti-RNP autoantibodies, were retrospectively included in this study. Patients with less than 100 µL of serum were excluded.
2.2. Clinical Data
This retrospective study exclusively analyzed data issued from health care, and all serum samples were part of a declared Biobank (DC 2012_1704). This study was approved by the Medical Evaluation Board and Health Data Committee of Assistance Publique-Hôpitaux de Marseille, Marseille, France (under GDPR number 2021-108), and fulfilled local requirements for data collection and data protection.
Based on information collected from medical records, 74 patients were classified into five clinical groups according to their disease, including cancer, infectious diseases, SLE, MCTD and other autoimmune diseases. SLE patients met the 2019 EULAR/ACR classification criteria [3], and MCTD patients met the Alarcón–Segovia criteria [1].
2.3. Immunoassays
2.3.1. ANA Testing
ANAs in patients’ sera were detected using a commercially available ANA HEp-2 indirect immunofluorescence assay (Kallestad HEp-2 Cell Line Substrate, 12-well slides, Bio-Rad Laboratories, Hercules, CA, USA). ANAs were visually assessed by two experienced observers using a fluorescence microscope (Leica DM-2000, Leica Microsystems, Wetzlar, Germany). The fluorescence pattern and titer were recorded for each sample.
2.3.2. Extractable Nuclear Antigen Antibody Testing
Fluorescence enzyme immunoassays (EliA^™^, Phadia 250, Thermo-Fisher Scientific, Phadia AB, Uppsala, Sweden) were used according to the manufacturer’s instructions to detect IgG autoantibodies directed against RNP, dsDNA, SSA/Ro, SSB/la, SmD, centromere B, Scl-70 and Jo-1 nuclear autoantigens. They were also used to detect IgG and IgM autoantibodies directed against RNP components, namely, RNP-A, RNP-C, RNP-70 and SmBB’ antigens. IgG EliA™ are commercially available and comply with the European In-vitro Diagnostics Regulation (IVDR), whereas IgM EliA™ have been developed by the manufacturer for research purposes only. Fluorescence was quantified using a calibration curve, and the results were expressed in U/mL. For samples with high levels of IgG anti-RNP-A, -RNP-C, -RNP-70, -SmD or -SmBB’ autoantibodies (outside the quantification range), the serum was diluted until the concentration was within the quantification range of the method. A cut-off of 10 U/mL was used for all autoantibodies except for anti-dsDNA IgG and anti-SmBB’ IgG/IgM, where the cut-off was 15 U/mL and 40 U/mL, respectively.
2.3.3. Testing the 40 kDa Fragment of RNP-70
Nuclear extracts from HeLa cells were prepared and separated by SDS-polyacrylamide gel electrophoresis and, subsequently, proteins from the extracts were transferred to a nitrocellulose membrane by Western blotting and cut into strips for the analysis of patient sera. Blocked strips were incubated with 1:100 diluted patient serum in a casein hydrolysate solution. After washing in PBS-Tween, the blots were incubated for one hour with a 1:30,000 diluted alkaline phosphatase-labeled goat anti-human IgG. After washing, the blot strips were developed with NBT/BCIP solution. The molecular weight of the 40 kDa fragment of RNP-70 was determined by alignment and comparison with the bands on the standard blot strips.
2.4. Calculation of the RNP Index
To further investigate the proportions of IgG autoantibodies directed against the RNP and Sm components of the U1-snRNP complex, and to compare them between SLE and MCTD, we combined the serum levels of anti-RNP-A, -C, -70 (aRNP-A, -C, -70), anti-SmD (aSmD) and SmBB’ (aSmBB) IgG autoantibodies into a single RNP index (RNPi), calculated as follows:
2.5. Statistical Analysis
Statistical analysis was performed using R software version 3.6.0 (R Foundation for Statistical Computing). Continuous variables were compared using Student’s t-test when appropriate (otherwise, the Mann–Whitney test), and categorical data were compared using the χ^2^ test when appropriate (otherwise, the Fisher test). Odds ratios (and their 95% confidence intervals) were estimated for each variable using univariate logistic regression. All tests were two-tailed. p < 0.05 was retained for significance.
3. Results
3.1. Clinical Description of Patients Positive for Anti-RNP
Seventy-four patients who were positive for RNP were included. There were 10 men (13.5%) and 64 women (86.5%) with a mean age of 45.2 ± 16.8 years. Clinically, 40 patients (54%) were diagnosed with SLE and 20 (27%) with MCTD. In addition, six patients (8.1%) had other autoimmune diseases (including one dermatomyositis, one psoriatic arthritis, one systemic sclerosis, one Hashimoto’s disease and two undifferentiated connective tissue disease), three patients (4.05%) had SARS-CoV-2 infection, three patients (4%) had cancer and two patients (2.7%) were classified as healthy with no suspected associated disease (Figure 1). Because of the small number of patients in the other groups, the statistical comparison for the subsequent results will be made only between patients with SLE and those with MCTD. Organ involvement in MCTD and SLE patients is described in Supplementary Table S1.
3.2. Differential Diagnosis between MCTD and SLE Based on Immunological Data
The immunological data initially analyzed included anti-nuclear autoantibodies (AAN), IgG anti-dsDNA autoantibodies, IgG autoantibodies against extractable nuclear antigens (ENA), including autoantibodies directed against RNP, SSA/Ro (60 kDa), SSB/La, Sm, centromere, Scl-70 and Jo-1. Both qualitative (Table 1) and quantitative (Table 2) analyses of the results showed a significant difference between patients with MCTD and SLE regarding anti-dsDNA IgG and anti-Sm IgG autoantibody positivity. The prevalence (p = 0.011 with OR = 6.49 and p = 0.011 OR = 5.67, respectively) and titers (p < 0.0001 and p = 0.005, respectively) of these autoantibodies were significantly higher in patients with SLE than in patients with MCTD. No difference in anti-RNP levels (whatever their subtype) was observed between patients with SLE and those with MCTD (Table 1). Irrespective of the group of patients, we can note the absence of autoantibodies against centromere, Scl-70 and Jo-1.
3.3. Differential Diagnosis between MCTD and SLE Based on the Detection of Autoantibodies against RNP Components
The detection of IgG and IgM autoantibodies directed against RNP components 70, A and C was then performed by the fluoroimmunoenzymatic assay. The detection of IgG autoantibodies against a 40 kDa fragment of RNP-70 was performed by a Western blot assay.
Irrespective of the quantitative (Table 1) or qualitative (Table 2) analyses, no difference was found between patients with SLE and MCTD regarding autoantibodies against RNP proteins (or 40 kDa RNP-70 fragment).
To further analyze the results, we attempted to combine the results obtained for RNP proteins. We first performed a study of different serological profiles against RNP components, exploring all possible associations, as shown in Figure 2. No difference was found between patients with SLE and MCTD (Figure 2). We then proposed an RNP index calculation, RNPi, as described in Section 2 “Materials and Methods”, which takes into account the RNP and Sm components within the U1-snRNP complex (Table 2). Interestingly, RNPi was significantly higher in MCTD patients than in SLE patients (p = 0.011, Table 1), and this result was also found in a subset of patients who were both anti-Sm- and anti-RNP-positive (p < 0.001, Figure 3A). In this subset of patients, RNPi above 0.571 discriminated MCTD from SLE with good performance (sensitivity: 69.2%, specificity: 88.9%, positive predictive value: 75%, negative predictive value: 85.7%, Figure 3B).
4. Discussion
Autoantigenicity of the U1-snRNP complex generates several autoantibodies against RNP-70, RNP-A, RNP-C and Sm proteins [16]. In order to discriminate between patients with MCTD and SLE, we propose the calculation of an original RNP index (RNPi), reflecting the proportion of autoantibodies produced against the different components within the U1-snRNP complex. This index, which is significantly higher in MCTD than in SLE, indicates a major autoantigenicity against the RNP components in MCTD and constitutes an attractive tool for its diagnosis. This ability of RNPi to discriminate between MCTD and lupus is also found in the subset of patients with both anti-Sm and anti-RNP, in whom it might be expected that the diseases would be more difficult to distinguish due to the presence of biological markers for both diseases.
In a well-documented cohort of patients selected on the basis of anti-U1-snRNP positivity, we found that 27% were diagnosed with MCTD, 54% with SLE and other clinical conditions as reported in the literature [2,17]. The immunological data initially analyzed showed a lack of autoantibodies against centromere B, Scl-70 and Jo-1 in the MCTD patients, but this has also been reported in MCTD cohorts of similar size [18] and does not prevent patients from having clinical signs of scleroderma or myositis, thus allowing a diagnosis of MCTD to be made. We also showed that anti-dsDNA and anti-Sm autoantibodies are significantly associated with SLE. Our data, in agreement with data in the literature [3], are insufficient for differential diagnosis in certain cases, especially in patients with MCTD who are positive for these discriminating autoantibodies.
In order to improve the diagnosis of MCTD, we investigated autoantibodies selectively directed against the individual RNP components, namely, 70, A and C. We found no preferential clinical association for autoantibodies directed against RNP-70, A or C, irrespective of the IgG or IgM isotype, nor for IgG autoantibodies directed against the 40 kDa fragment of RNP-70. The few studies reported in the literature show inconsistent results. Older studies described a preferential association with anti-RNP-70 in MCTD, whereas anti-RNP-A/C was associated with SLE [19,20,21]. Recently, Ahmad et al. concluded that the detection of anti-RNP-70 is not of clinical interest [22]. In addition, previous studies have shown that high levels of anti-RNP are associated with MCTD. In contrast, we have shown that anti-RNP levels do not contribute to the differential diagnosis. Consistent with this, Alves et al. reported that many patients with high anti-RNP levels did not have MCTD, whereas patients with MCTD had either low levels or no evidence of anti-RNP [23]. Additionally, some authors [24,25] reported that IgM anti-U1 snRNP titers were significantly higher in the SLE population than in the MCTD population, but we did not find such a result for the IgM isotype. These inconsistent results may be related to the number of patients and the techniques used.
In our study, the evaluation of different serological profiles of the anti-RNP autoantibodies did not reveal any clinical association. In contrast, the proportion of autoantibodies directed against the RNP component within the U1-snRNP complex showed a significantly higher RNP index in patients with MCTD than in those with SLE (Figure 4). This result demonstrates a higher autoimmunogenicity of RNP proteins in MCTD than in SLE. The use of anti-RNP positivity as a criterion for MCTD has recently divided the rheumatology community. Some studies have questioned the relevance of these autoantibodies, as patients without anti-RNP and with typical symptoms have been reported in the literature [23,26]. In addition, a genetic association between the HLA haplotype and anti-RNP autoantibodies has been reported in MCTD, confirming the interest in detecting these autoantibodies [27,28]. In line with this, our results highlight a preferential autoantigenicity against RNP components in MCTD compared to SLE and raise the question of the evaluation of autoantibodies. Which autoantibodies against RNPs should we be looking for? The data suggest that because autoantibodies are produced against a multimolecular complex appearing as a true autoantigenic mosaic, the analysis of each autoantibody separately is not appropriate; rather, the analysis of the proportion of autoantibodies produced against the components of the U1-snRNP complex is more informative.
A major limitation of our study is the size of the cohort. Further studies are needed to test the RNP index in a larger cohort of patients to confirm the diagnosis of MCTD. Patient follow-up could be informative about the interest of this index as a predictor of the evolution of the disease.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Alarcón-Segovia D. Mixed connective tissue disease and overlap syndromes Clin. Dermatol.19941230931610.1016/S 0738-081X(94)90336-08076270 · doi ↗ · pubmed ↗
- 2Benito-Garcia E. Schur P.H. Lahita R. American College of Rheumatology Ad Hoc Committee on Immunologic Testing Guidelines Guidelines for immunologic laboratory testing in the rheumatic diseases: Anti-Sm and anti-RNP antibody tests Arthritis Rheum.2004511030104410.1002/art.2083615593352 · doi ↗ · pubmed ↗
- 3Aringer M. Costenbader K. Daikh D. Brinks R. Mosca M. Ramsey-Goldman R. Smolen J.S. Wofsy D. Boumpas D.T. Kamen D.L. 2019 European League Against Rheumatism/American College of Rheumatology classification criteria for systemic lupus erythematosus Ann. Rheum. Dis.2019781151115910.1136/annrheumdis-2018-21481931383717 · doi ↗ · pubmed ↗
- 4Pomeranz Krummel D.A. Oubridge C. Leung A.K.W. Li J. Nagai K. Crystal structure of human spliceosomal U 1 sn RNP at 5.5 A resolution Nature 200945847548010.1038/nature 0785119325628 PMC 2673513 · doi ↗ · pubmed ↗
- 5Wilkinson M.E. Charenton C. Nagai K. RNA Splicing by the Spliceosome Annu. Rev. Biochem.20208935938810.1146/annurev-biochem-091719-06422531794245 · doi ↗ · pubmed ↗
- 6Maris C. Dominguez C. Allain F.H.-T. The RNA recognition motif, a plastic RNA-binding platform to regulate post-transcriptional gene expression FEBS J.20052722118213110.1111/j.1742-4658.2005.04653.x 15853797 · doi ↗ · pubmed ↗
- 7Kondo Y. Oubridge C. van Roon A.-M.M. Nagai K. Crystal structure of human U 1 sn RNP, a small nuclear ribonucleoprotein particle, reveals the mechanism of 5′ splice site recognition Elife 20154 e 0498610.7554/e Life.0498625555158 PMC 4383343 · doi ↗ · pubmed ↗
- 8Casciola-Rosen L.A. Miller D.K. Anhalt G.J. Rosen A. Specific cleavage of the 70-k Da protein component of the U 1 small nuclear ribonucleoprotein is a characteristic biochemical feature of apoptotic cell death J. Biol. Chem.1994269307573076010.1016/S 0021-9258(18)47343-77983001 · doi ↗ · pubmed ↗