Cholecystitis and Cardiomyopathy in an Immunocompetent Patient With Cytomegalovirus Infection: A Case Report
Hieu M Vo, Jerry M Sheppard

TL;DR
A 53-year-old man with no immune issues developed cholecystitis and heart issues linked to a cytomegalovirus infection.
Contribution
Highlights CMV as a rare cause of cholecystitis and cardiomyopathy in immunocompetent individuals.
Findings
CMV infection was linked to subacute cholecystitis and cardiomyopathy in an immunocompetent patient.
Abnormal liver enzymes and fever suggested viral involvement despite no cardiac symptoms.
Co-infection or cross-reactivity with WNV and EBV was indicated by positive serology.
Abstract
In this case report, we present a 53-year-old immunocompetent male exhibiting cholecystitis and cardiomyopathy related to cytomegalovirus (CMV) infection. The initial presentation pointed toward cholecystitis, including epigastric pain, chronic dysgeusia, dyspepsia, and cholelithiasis on ultrasound. A cholecystectomy was performed, and tissue analysis showed subacute cholecystitis. Postsurgical daily fever spikes prompted subsequent evaluation, which revealed CMV infection along with cardiomyopathy as evidenced by a reduced left ventricular ejection fraction, despite no suggestive clinical symptoms. Gastrointestinal symptoms, along with elevated liver enzymes, indicated possible congestive hepatopathy. Preceding symptoms also suggested a viral etiology, including a protracted fever and a possible transient Bell’s palsy. Medical management for viral myocarditis was initiated, and the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1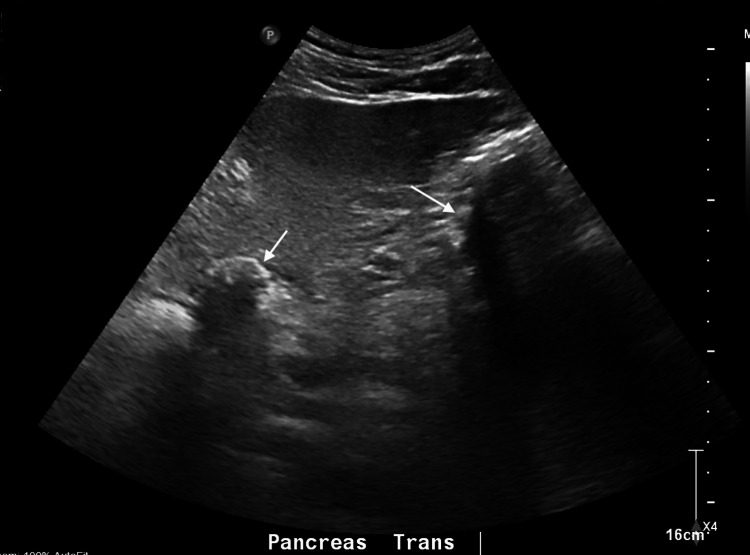 Figure 2
Figure 2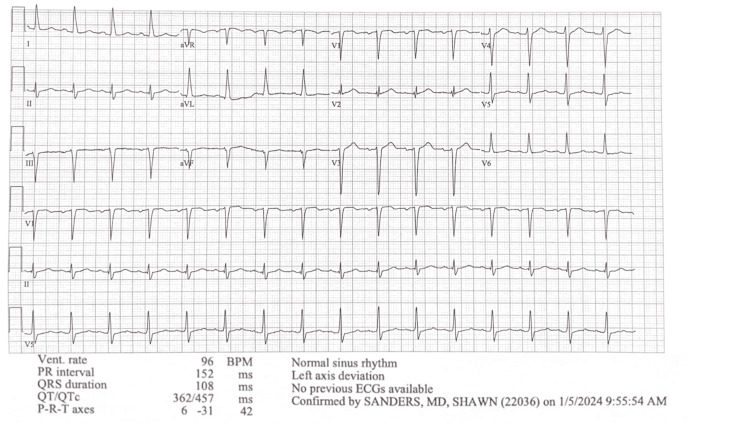 Figure 3
Figure 3| Test | Value | Reference range |
| WBC | 14.4 K/uL | 5-10 K/uL |
| AST | 128 U/L | 17-59 U/L |
| ALT | 194 U/L | 21-72 U/L |
| Alkaline phosphatase | 305 U/L | 38-126 U/L |
| Test | Value | Reference range |
| WBC | 9.6 K/uL | 5-10 K/uL |
| AST | 206 U/L | 17-59 U/L |
| ALT | 285 U/L | 21-72 U/L |
| Alkaline phosphatase | 251 U/L | 38-126 U/L |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCytomegalovirus and herpesvirus research · Herpesvirus Infections and Treatments · Kawasaki Disease and Coronary Complications
Introduction
The prevalence of cytomegalovirus (CMV) infection ranges from 60% to 70% in developed countries to nearly 100% in developing regions, correlating positively with age [1]. In a U.S.-based study, CMV seroprevalence increased from 36% among six- to 11-year-olds to 91% in those over 80 [2]. Transmission occurs through body fluids, including sexual exposure, close contact, or perinatal exposure [3]. Primary infection in immunocompetent individuals often remains asymptomatic but may result in a self-limiting presentation. It can be life-threatening in immunocompromised patients. Common symptoms of primary CMV infection include prolonged fever, fatigue, night sweats, myalgia, and headache. Common laboratory findings include atypical lymphocytes, leukocytosis, and elevated serum transaminases [4]. CMV infection, although rare in immunocompetent individuals, can affect virtually every organ in the body, including gallbladder, heart, lung, brain, liver, and others. Similar presentations can occur due to Epstein-Bar virus (EBV) or West Nile virus (WNV), precluding definitive diagnosis due to possible co-infection or cross-reactivity with the testing reagents.
This case report describes a patient with CMV infection manifesting as gallbladder and cardiac involvement. The viral workup also indicates likely past infections of EBV, but it is uncertain whether WNV positivity is due to an active or past infection.
Case presentation
A 53-year-old male patient presented to the emergency department with a five-day history of epigastric abdominal pain, fever, nausea, and vomiting. He was in acute distress but alert. His vitals were: blood pressure 115/81, heart rate 95, respiratory rate 18, temperature 98.5°F (36.9°C), SpO_2_ 100%. Examination revealed right upper quadrant (RUQ) tenderness to palpation. Computed tomography (CT) of the abdomen with contrast showed fatty liver and cholelithiasis, but no sign of acute cholecystitis (Figure 1). There was no history of alcohol use disorder. Significant lab findings included elevated white blood cell count (WBC) with lymphocytic predominance and elevated liver enzymes with normal bilirubin (Table 1). He denied recent travel, tick bites or exposure to rabbits, cows, or other exotic animals.
CT scan of the abdomen.The CT scan of the abdomen shows gallstones (white arrow) with the presence of fatty liver. There is no evidence of RUQ inflammation or bile duct dilation. CT: computed tomography, RUQ: right upper quadrant.
Five days prior, he was evaluated in the local emergency department for a three-week history of fatigue, anorexia, cough, chills, diaphoresis, and fluctuating fever, peaking at 104°F. His vitals were: blood pressure 112/99, heart rate 119, respiratory rate 19, temperature 101.5°F (38.6°C), and SpO_2_ 98%. He was not in acute distress. Three weeks before the onset of symptoms, he experienced transient right-sided facial numbness and jaw movement difficulty. The exam at the time was significant for mild posterior oropharyngeal erythema. The screening for COVID-19, influenza, streptococcus infection, and mononucleosis was negative. Lab findings were significant for elevation in aspartate aminotransferase (AST), alanine aminotransferase (ALT), and alkaline phosphatase (ALP), but normal white blood cell count (WBC) (Table 2). Because he is a hunter, he was given doxycycline and Rocephin for a possible tick-borne illness.
Given his gastrointestinal symptoms, including dysgeusia, a long history of indigestion, and cholelithiasis on abdominal ultrasound (Figure 2), the patient underwent cholecystectomy, which revealed subacute and chronic cholecystitis from a pathology exam. Post-surgery, his abdominal pain and dysgeusia improved, but he continued to experience high-grade fever spikes, fatigue, diaphoresis, chills, anorexia, and persistent leukocytosis with lymphocytic predominance, along with conjunctival erythema. A subsequent extensive viral workup with cerebrospinal fluid (CSF) analysis showed a CMV IgM of 137 AU/mL (reference range: <35 AU/mL) and a CMV DNA viral load of 99.7 IU/mL (reference range: 0 IU/mL). EBV IgM was positive with an indeterminate EBV DNA viral load. Surprisingly, WNV IgM was also positive. The hepatitis panel was negative. An echocardiogram showed global hypokinesis with a left ventricular ejection fraction (LVEF) of 30-35%, despite the absence of dyspnea, orthopnea, syncope, or chest pain throughout the course of his illness up to this point. His wife reported that he preferred to sleep on the couch during this prolonged illness, but he is unsure if it is due to orthopnea. The electrocardiogram (Figure 3) and cardiac positron emission tomography (PET) were negative. Viral myocarditis was suspected to be the underlying cause of his abnormal echocardiogram. It is possible that his cholecystitis is also virally mediated.
Ultrasound of the RUQ of the abdomen.There are stones (white arrows) with acoustic shadowing within the gallbladder and a fatty liver. RUQ: right upper quadrant.
Electrocardiogram showed normal sinus rhythm with left axis deviation. Other findings were within normal limits.
For viral myocarditis in immunocompetent patients, the mainstay of treatment is to manage acute heart failure with reduced ejection fraction, as antiviral therapy has uncertain efficacy [5]. Per guideline-directed medical therapy, he was put on Aldactone and Toprol, as these, along with angiotensin-converting enzyme inhibitors (ACEIs), have been shown to reduce the extent of myonecrosis, morbidity, and mortality [6,7]. The patient was discharged and will follow-up with his cardiologist, infectious disease specialist, and primary care physician.
Post-discharge, the patient continued to have diaphoresis, low-grade fever controlled with Tylenol, and new-onset orthopnea. Repeated lab tests two weeks after discharge showed normalization of leukocytosis and liver function tests. A repeat echocardiogram showed no change in LVEF. He still had some fatigue.
Three months after discharge, his echocardiogram still showed a reduced LVEF of 30-35%. He still reports increasing fatigue and a 7-lb weight loss in the past month. He denies lower extremity edema, orthopnea, paroxysmal nocturnal dyspnea, or palpitations. Long-term close follow-up is needed with medication titration since the recovery of cardiac function can take months or years.
Discussion
CMV infection is usually subclinical in the immunocompetent population, but it may manifest with flu-like symptoms and can involve multiple organs. It should be part of the differential diagnosis in case of protracted, fluctuating fever and other flu-like symptoms. Other findings consistent with a viral etiology include a recent history of possible mild right-sided Bell's palsy, isolated liver enzyme elevation, and lymphocyte-predominant leukocytosis. His history of spending time and sharing drinks with his grandchildren can be a potential exposure factor. While the initial presentation at the ED suggested possible cholecystitis from cholelithiasis, the preceding protracted fever and flu-like symptoms indicated a viral infection as a likely etiology. The echocardiogram’s findings of moderate-severe cardiomyopathy with an LVEF of 30-35% and global hypokinesis were unexpected, given the absence of cardiac symptoms, including chest pain, dyspnea, orthopnea, or syncope, until post-discharge. The echocardiogram was ordered due to isolated liver enzyme elevation and fatigue, which could be due to congestive hepatopathy and low cardiac output. This underscores the potential need to include an echocardiogram in a viral infection workup, even in the absence of obvious cardiac symptoms, which could be delayed. Retrospectively, the cholecystitis change seen in the pathology report could be attributed to chronic congestion due to a reduced ejection fraction, although we do not know how long the patient has had cardiomyopathy.
The case demonstrates the diagnostic dilemma in determining the true cause of cardiomyopathy and cholecystitis without a pathology study, due to the multiple positive results in the viral panel. The high CMV viral load indicates active infection, while the positive EBV IgM with indeterminate EBV polymerase chain reaction (PCR) suggests possible cross-reactivity or past infection. WNV IgM can persist for up to eight years in 23% of study participants [8]. Together with a case report [9] demonstrating the presence of viral cardiomyopathy with an isolated positive WNV IgM, WNV could be the cause of this patient’s presentation. In addition, protracted flu-like symptoms are common in both CMV and WNV infections. Thus, an invasive biopsy may be necessary for a definitive diagnosis, but it is not often performed.
Conclusions
The expected outcome of acute myocarditis depends on the severity of the initial presentation. With mild disease, patients usually have a good prognosis with partial or complete recovery. The fulminant disease often leads to cardiogenic shock with high mortality. Some may continue to have subclinical disease, which later becomes more symptomatic with dilated cardiomyopathy. In viral myocarditis, early treatment with ACEIs and BBs can reduce morbidity and mortality. Close follow-up with a cardiologist is crucial since recovery can take months to years.
This case illustrates the potential complexity in diagnosing and managing patient with CMV infection due to its cardiac and gallbladder involvement. The multiple positive lab findings for CMV, EBV, and WNV may represent possible co-infection or cross-reactivity with diagnostic reagents. Fortunately, the lack of a definitive diagnosis does not change the general management needed to optimize recovery in viral cardiomyopathy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cytomegalovirus Stat Pearls (Internet) 8 2023 Gupta M Shorman M Treasure Island, FL Stat Pearls Publishing 2023 https://www.ncbi.nlm.nih.gov/books/NBK 459185/29083720 · pubmed ↗
- 2Seroprevalence of cytomegalovirus infection in the United States, 1988-1994 Clin Infect Dis Staras SA Dollard SC Radford KW Flanders WD Pass RF Cannon MJ 114311514320061702913210.1086/508173 · doi ↗ · pubmed ↗
- 3Cytomegalovirus infection in pregnancy: an update Eur J Obstet Gynecol Reprod Biol Navti OB Al-Belushi M Konje JC 21622225820213345451010.1016/j.ejogrb.2020.12.006 · doi ↗ · pubmed ↗
- 4Primary cytomegalovirus infection in immunocompetent adults in the United States: a case series ID Cases Nolan N Halai UA Regunath H Smith L Rojas-Moreno C Salzer W 1231261020172915907010.1016/j.idcr.2017.10.008PMC 5684088 · doi ↗ · pubmed ↗
- 5Cytomegalovirus infection in immunocompetent and immunocompromised individuals-a review Current Drug Targets-Immune, Endocrine & Metabolic Disorders Vancikova Z Dvorak P 179187 Sharjah Bentham Science Publishers 200112476798 · pubmed ↗
- 6Therapies to limit myocardial injury in animal models of myocarditis: a systematic review and meta-analysis Basic Res Cardiol Silverblatt JA Ziff OJ Dancy L 4811420193167388510.1007/s 00395-019-0754-x PMC 6823299 · doi ↗ · pubmed ↗
- 7Viral myocarditis Stat Pearls (Internet) Kang M Chippa V An J Treasure Island, FL Stat Pearls Publishing 2023 https://www.ncbi.nlm.nih.gov/books/NBK 459259/29083732 · pubmed ↗
- 8Persistence of detectable immunoglobulin M antibodies up to 8 years after infection with West Nile virus Am J Trop Med Hyg Murray KO Garcia MN Yan C Gorchakov R 99610008920132406248110.4269/ajtmh.13-0232 PMC 3820351 · doi ↗ · pubmed ↗