Recurrent Left-Sided Hepatic Hydrothorax Leading to Liver-Mediated Dyspnea
Dhaval Trivedi, Kin Li, Sana Ahmed, Franklyn Fenton, Saleem Shahzad

TL;DR
This paper presents a rare case of left-sided hepatic hydrothorax in a 70-year-old woman with cirrhosis, causing shortness of breath without ascites.
Contribution
The novelty lies in reporting a rare left-sided hepatic hydrothorax case without ascites in a cirrhosis patient.
Findings
Left-sided hepatic hydrothorax can occur in cirrhosis patients without ascites.
Shortness of breath may be caused by hepatic hydrothorax in cirrhosis.
This case highlights the need for broader diagnostic consideration in cirrhosis-related dyspnea.
Abstract
Cirrhosis is a common liver condition caused by several etiologies including alcohol use disorder, infectious hepatitis, and metabolic dysfunction associated with liver disease. Although common symptomatic complications of cirrhosis include malaise, gastrointestinal bleeding, and abdominal distension, shortness of breath is a less common phenomenon that may occur. Hepatic hydrothorax (HH) is an uncommon cause of shortness of breath that is believed to be caused by the accumulation of ascitic fluid in the pleural space. While most cases of HH occur with ascites and the right side, we hereby present a case of a 70-year-old female with left-sided HH without ascites.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
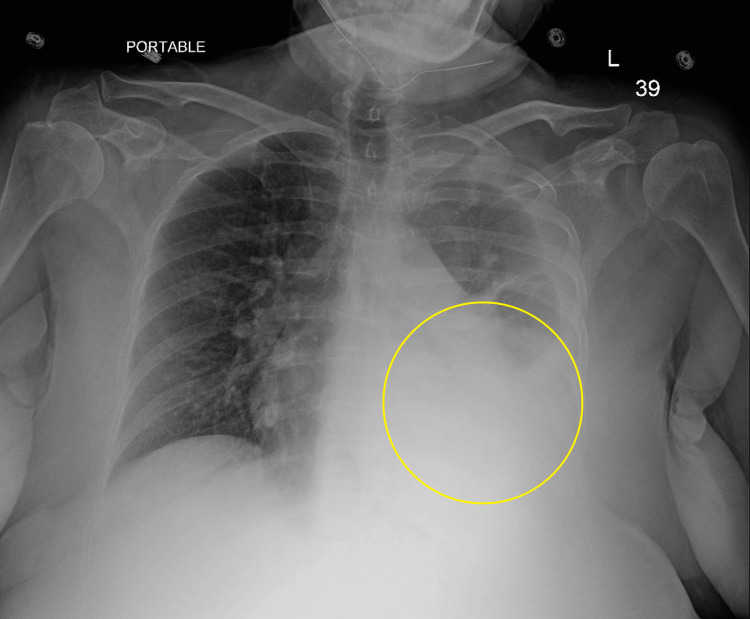 Figure 1
Figure 1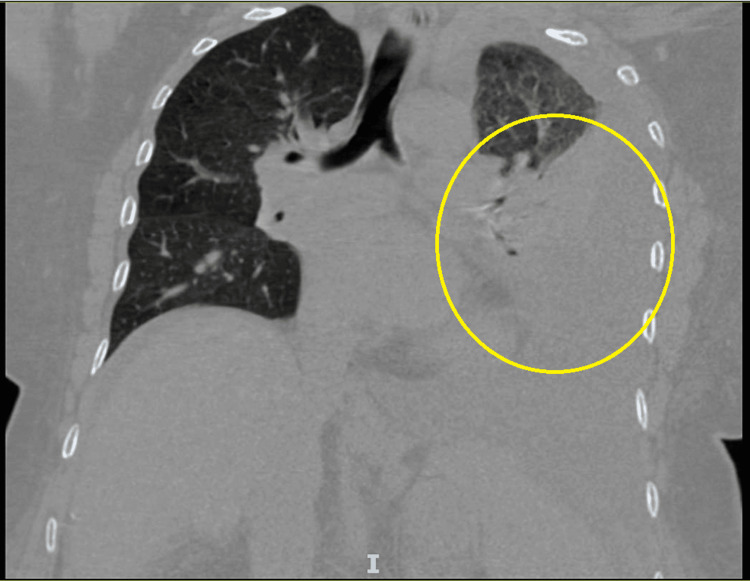 Figure 2
Figure 2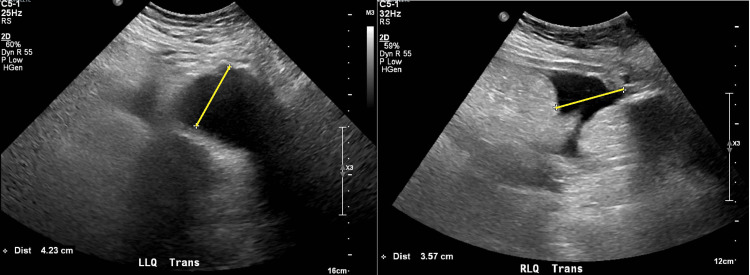 Figure 3
Figure 3| Laboratory Value | Patient's Value | Reference Range |
| White Blood Cell | 3.2 | 3.5-11.0 x 10^3/uL |
| Hemoglobin | 13.4 | 11.5-14.5 g/dL |
| Platelets | 58 | 150-400 x 10^3/uL |
| Sodium | 137 | 136-145 mmol/L |
| Potassium | 3.3 | 3.5-5.1 mmol/L |
| Chloride | 103 | 98-107 mmol/L |
| Carbon Dioxide | 23 | 22-29 mmol/L |
| Blood Urea Nitrogen | 10 | 8-23 mg/dL |
| Creatinine | 17 | 0.51-0.95 mg/dL |
| Glucose | 0.57 | 74-106 mg/dL |
| Aspartate Transaminase | 79 | <40 U/L |
| Alanine Transaminase | 28 | <40 U/L |
| Alkaline Phosphatase | 112 | <200 U/L |
| Total Bilirubin | 3.4 | 0.1-1.2 mg/dL |
| Direct Bilirubin | 0.6 | 0.0-0.3 mg/dL |
| Plasma Albumin | 2.7 | 3.5-5.2 g/dL |
| Activated Partial Thromboplastin Time | 37.9 | 25.1-36.5 seconds |
| Prothrombin Time | 19.3 | 9.4-21.5 seconds |
| International Normalized Ratio | 1.7 | 0.9-1.2 ratio |
| Laboratory Value | Patient's Value | Transudative Reference Range |
| Fluid/Serum Protein (g/dL) | 2.0/6.6 | < 0.5 |
| Fluid/Serum Lactate Dehydrogenase (U/L) | 86/287 | < ⅔ the upper limit of normal serum |
| Laboratory Value | Patient's Value | Transudative Reference Range |
| Serum Albumin | 2.2 | 3.5-5.2 g/dL |
| Fluid Albumin | 1.058 | <1 g/dL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital Diaphragmatic Hernia Studies · Pleural and Pulmonary Diseases · Medical Imaging and Pathology Studies
Introduction
Dyspnea is a common pulmonary complication that can be caused by pulmonary or cardiac diseases such as heart failure, pneumonia, or chronic obstructive pulmonary disease. While many other conditions such as anemia or mental disorders may present similarly, hepatic causes of shortness of breath are uncommon [1]. Hepatic hydrothorax (HH) describes the presence of greater than 500 milliliters of fluid in the pleural space as sequelae of liver dysfunction in the absence of renal, cardiac, and pulmonary pathologies. This type of presentation is usually noted in the setting of decompensated liver failure alongside portal hypertension and ascitic fluid accumulation. Although most cases of HH typically present with ascites, some cases may present more insidiously without typical signs of ascites [2].
Previous studies have reported incidence rates of HH in the setting of cirrhosis and portal hypertension range between 5% and 16%. In previous retrospective case series, patients with HH typically presented with a right-sided pleural effusion (73%). However, left-sided (17%) and bilateral pleural effusions (10%) also occurred infrequently. In the majority of these cases, ascites were also a commonly associated finding with only some case series reporting 9% of patients without any ascites [3,4]. However, left-sided HH without ascites is rarely reported. In this case presentation, we report a 70-year-old female who presented with left-sided HH without any ascites.
Case presentation
A 70-year-old female with a history of hypertension, type 2 diabetes mellitus, treated hepatitis C (genotype 3a), metabolic dysfunction-associated steatotic liver disease (MASLD), and cirrhosis associated with grade 1 esophageal varices presented to the Emergency Department with complaints of abdominal pain and leg swelling for one week with new-onset shortness of breath for three days. The abdominal pain was epigastric, prandial, and positional with radiation to her right upper quadrant. The pain was unrelieved with acetaminophen. The shortness of breath was previously only associated with exertion, but now occurs at rest.
In the Emergency Department, her vital signs were normal, and physical examination revealed epigastric tenderness, lower extremity non-pitting edema, and decreased breath sounds in the left lower lung field. An initial chest X-ray (CXR) was performed which revealed a left-sided pleural effusion (Figure 1, yellow circle). Initial labs (Table 1) were remarkable for leukopenia, thrombocytopenia, hypokalemia, hypoalbuminemia, hyperbilirubinemia, transaminitis, and elevated prothrombin time (PT)/international normalized ratio (INR). CT abdomen and pelvis revealed a nodular contour of the liver, splenomegaly with multiple prominent vascular collaterals, moderate ascites, and gastroesophageal varices (Figure 2, yellow circle).
Chest X-rayYellow circle: pleural effusion
CT ChestYellow circle: pleural effusion
As seen in Table 1, initial labs were remarkable for leukopenia, thrombocytopenia, hypokalemia, hypoalbuminemia, hyperbilirubinemia, transaminitis, and elevated PT/INR. CT abdomen and pelvis revealed nodular contour of the liver, splenomegaly with multiple prominent vascular collaterals, moderate ascites, and gastroesophageal varices (Figure 2). Abdominal ultrasound was performed for the evaluation of ascitic fluid evaluation, but low volume anechoic free fluid was found.
However, abdominal ultrasound was performed for the evaluation of ascitic fluid but only revealed low-volume free fluid (Figure 3, yellow lines) with a demonstration of large left pleural effusion. Given the concern for new-onset heart failure, a transthoracic echocardiogram was ordered, which revealed a normal systolic ejection fraction. Additionally, as the patient met sepsis criteria, a septic workup was performed and ceftriaxone and azithromycin were initiated for community-acquired pneumonia coverage. Septic workup was found to be negative with normal procalcitonin and antibiotics were subsequently stopped.
Abdominal Ultrasound for Ascites EvaluationLLQ trans: left lower quadrant transabdominal; RLQ trans: right lower quadrant transabdominal
Due to persistent shortness of breath, diagnostic and therapeutic thoracentesis was performed. Post-procedure CXR revealed persistent but decreased left-sided pleural effusion. The culture and cytology on the fluid sample were unremarkable. The fluid protein was noted to be 2.2 g/dL and the fluid lactate dehydrogenase was 86 g/dL. Analysis using Light's criteria revealed the sample to be transudative, as both the fluid-to-serum protein ratio and the fluid-to-lactate dehydrogenase ratio were less than 0.5 and two-thirds of the upper limit of normal, respectively (Table 2).
The following day, CXR was once again repeated due to shortness of breath complaint, which revealed increased left-sided pleural effusion. Repeat diagnostic and therapeutic thoracentesis was performed with subsequent SPAG (serum pleural-ascites gradient) studies (Table 3). The serum albumin was 2.2 g/dL and the fluid albumin was 1.058 g/dL, which revealed a SPAG of 1.142 g/dL. SPAG studies revealed cirrhosis as an etiology for effusion. Technetium-99m sulfur colloid nuclear scan was unavailable for nuclear evaluation for HH. Given the concern for HH as an etiology for pleural effusion, diuresis therapy was initiated with spironolactone 100 mg daily and furosemide 40 mg twice daily, which provided symptomatic relief. Ultimately, the patient was discharged with spironolactone 200 mg daily and furosemide 40 mg twice daily, which was subsequently halved at an outpatient hepatology visit. One month post-discharge and initiation of diuresis, repeat CXR showed complete resolution of pleural effusion.
Discussion
In patients presenting with HH, mortality is high with some case series indicating a 57% mortality rate within 12 months and 4-5 months in those with refractory cases [2]. In cases where patients undergo transjugular intrahepatic portosystemic shunt (TIPS), mortality extends to 845 days, and those with transplants indicate the longest survival rates [3].
HH is typically a diagnosis of exclusion in which underlying cardiopulmonary or renal disease has been excluded. Although most patients with HH may have cirrhosis and ascites, some patients may present with HH as the first sign of liver failure and without ascites. In our patient, she had known cirrhosis without a history of ascites. While her initial CT of the abdomen and pelvis showed large pleural effusion and moderate ascites, there was only minimal free fluid in the abdomen on further abdominal ultrasonography.
The exact mechanisms for the development of HH are not well known. However, several theories have been postulated including hypoalbuminemia, structural defects, and osmotic and hydrostatic pressure differentials within the azygos and lymphatic systems [5]. The most accepted theory is the direct passage of ascitic fluid from the peritoneal to the pleural cavity through diaphragmatic defects, which are referred to as pleuroperitoneal communications. Predominantly occurring on the right side, due to the embryological development of the diaphragm, these microscopic defects have been described as discontinuities of collagen within the tendinous portion of the diaphragm [6]. These defects have been classified into four morphological types of various severity including type 1 with no obvious defect, type 2 with blebs within the diaphragm, type 3 with broken defects or fenestrations in the diaphragm, and type 4 with multiple gaps in the diaphragm [7].
Diagnosis of HH typically involves a combination of imaging studies and pleural fluid testing. HH is usually first seen on chest radiographs. In patients with suspected HH, a thoracentesis is typically performed for fluid analysis. HH typically will have a transudative effusion based on Light’s criteria. However, the use of serum-pleural albumin gradient has also been suggested as another diagnostic criterion for HH as some studies showed all patients with HH had SPAG measuring >1.1 g/dL [8]. An echocardiogram should also be performed to rule out any cardiac etiologies and abdominal ultrasounds to assess the liver, portal and hepatic veins, ascites, and kidneys. In cases where the diagnosis of HH is uncertain, intraperitoneal injection of radioisotopes of 99mTc-human serum albumin may demonstrate migration from the peritoneal cavity into pleural space and confirm the diagnosis of HH. The most optimal timing for this study is typically performed after therapeutic thoracentesis.
The management of HH is nuanced. In those with an initial diagnosis of HH, treatment should be focused on eliminating the cause of ascites. The use of sodium restriction and the use of diuretics are typically a mainstay in the initial management of ascite reduction [9]. In refractory HH, or roughly 21-26% of medically treated patients, the only definitive treatment is liver transplantation [9,10]. While awaiting transplantation, the goal is to reduce the symptomatic burden and the prevention of pulmonary complications through interventions such as diuresis, thoracentesis, chest tube placement, pleural catheters, TIPS, and surgical interventions (pleurodesis, diaphragmatic repair, or pleural-venous shunting) [11,12]. Our case demonstrated a case of recurrent atypical left-sided hydrothorax without ascites, which was initially treated with aggressive diuresis and sodium restriction. Although our patient had a resolution of HH with mainstay therapy, consideration for liver transplantation was and should be further discussed in the multidisciplinary approach to improve long-term outcomes in patients' mortality and morbidity.
Conclusions
In conclusion, HH remains a challenging complication of liver disease with a high mortality rate, particularly in refractory cases. The condition often requires a nuanced approach to diagnosis and management, incorporating imaging studies, fluid analysis, and exclusion of other potential causes. Initial management typically involves sodium restriction and diuretics, while definitive treatment for refractory cases hinges on liver transplantation. The case discussed underscores the complexity of HH, highlighting the need for a multidisciplinary approach to optimize patient outcomes, reduce symptomatic burden, and improve survival rates through advanced interventions such as TIPS and liver transplantation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The differential diagnosis of dyspnea Dtsch Arztebl Int Berliner D Schneider N Welte T Bauersachs J 83484511320162809806810.3238/arztebl.2016.0834 PMC 5247680 · doi ↗ · pubmed ↗
- 2Hepatic hydrothorax: a narrative review Pulm Ther Pippard B Bhatnagar M Mc Neill L Donnelly M Frew K Aujayeb A 241254820223575180010.1007/s 41030-022-00195-8PMC 9458779 · doi ↗ · pubmed ↗
- 3Hepatic hydrothorax: clinical features, management, and outcomes in 77 patients and review of the literature Medicine (Baltimore) Badillo R Rockey DC 1351429320142479716810.1097/MD.0000000000000025 PMC 4632908 · doi ↗ · pubmed ↗
- 4Hepatic hydrothorax: an updated review on a challenging disease Lung Chaaban T Kanj N Bou Akl I 39940519720193112970110.1007/s 00408-019-00231-6 · doi ↗ · pubmed ↗
- 5Hepatic hydrothorax Ann Hepatol Lv Y Han G Fan D 33461720182931140810.5604/01.3001.0010.7533 · doi ↗ · pubmed ↗
- 6Detection of diaphragmatic defect as the cause of severe hepatic hydrothorax with magnetic resonance imaging Am J Gastroenterol Zenda T Miyamoto S Murata S Mabuchi H 22882289931998982041810.1111/j.1572-0241.1998.00639.x · doi ↗ · pubmed ↗
- 7The morphology of diaphragmatic defects in hepatic hydrothorax: thoracoscopic finding J Thorac Cardiovasc Surg Huang PM Chang YL Yang CY Lee YC 14114513020051599905410.1016/j.jtcvs.2004.08.051 · doi ↗ · pubmed ↗
- 8Left hepatic hydrothorax without ascites BMJ Case Rep Garin D Voirol U Vaucher J Grandmaison G 25842717202410.1136/bcr-2023-258427 PMC 1080685038199650 · doi ↗ · pubmed ↗