Assessment of Public Awareness of Cellulitis in Al-Qunfudhah Region, Saudi Arabia
Medhat Taha, Mazen Mohammed Minaji Alzelaei, Ali Mohammed Salem Al-Qarni, Mohammed Ahmed Muhanni Al-Ammari, Hassan Shulaymi Thakir Algamdi, Abdullah Amer Ibrahim Almaeidi, Hassan Abdu Ali Al-Faqih

TL;DR
This study assesses public awareness of cellulitis in Saudi Arabia's Al-Qunfudhah region, finding higher awareness among educated and employed individuals.
Contribution
The study provides region-specific insights into public understanding of cellulitis and factors influencing awareness.
Findings
Most participants correctly identified cellulitis as a skin and soft tissue infection.
Awareness was significantly associated with higher education and employment status.
Participants emphasized the role of healthcare providers in improving awareness.
Abstract
Background: The term "cellulitis" is frequently used to describe a non-necrotizing inflammation of the skin and subcutaneous tissues that is typically caused by an acute infection and does not affect the muscles or fascia. Warmth, erythema, tenderness, swelling, and localized pain are the hallmarks of cellulitis. Life-threatening and debilitating outcomes from cellulitis include necrotizing fasciitis, necrotizing hypodermitis, abscess formation, septic shock, and, in extreme cases, death. The current study aimed to assess public awareness of cellulitis in the Al-Qunfudhah region, Saudi Arabia. Methods: A descriptive cross-sectional study was conducted targeting all residents in Al-Qunfudhah, Saudi Arabia, during the period from January to March 2024. Data were collected using a pre-structured online questionnaire. The study questionnaire included participants' demographic data,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
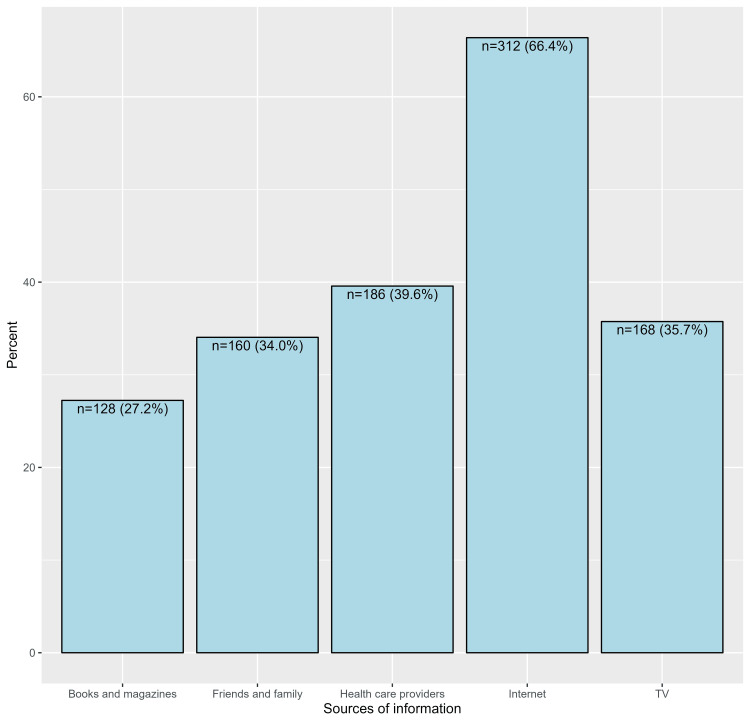 Figure 1
Figure 1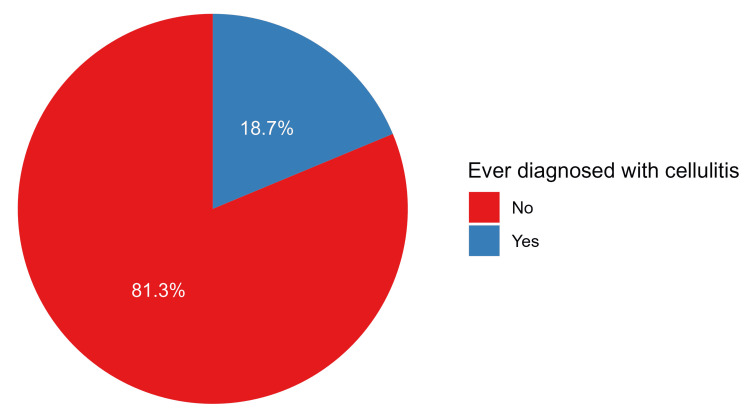 Figure 2
Figure 2| Characteristic | N (%) |
| Gender | |
| Male | 347 (73.8%) |
| Female | 123 (26.2%) |
| Age (years) | |
| 18 to 25 | 174 (37.0%) |
| 26 to 35 | 145 (30.9%) |
| 36 to 45 | 105 (22.3%) |
| 46 to 55 | 35 (7.4%) |
| >55 | 11 (2.3%) |
| Educational levels | |
| Illiterate | 1 (0.2%) |
| Primary | 10 (2.1%) |
| Middle school | 11 (2.3%) |
| Secondary | 90 (19.1%) |
| University | 321 (68.3%) |
| Diploma | 4 (0.9%) |
| Master's | 26 (5.5%) |
| PhD | 7 (1.5%) |
| Employment status | |
| Non-employed | 219 (46.6%) |
| Employed | 251 (53.4%) |
| Nationality | |
| Saudi | 469 (99.8%) |
| Non-Saudi | 1 (0.2%) |
| Characteristic | N (%) |
| Ever heard about cellulitis | 231 (49.1%) |
| What is cellulitis? | |
| Cellulitis is a medical condition that affects the skin and the soft tissues underneath it, usually caused by infection or injury* | 278 (59.1%) |
| Cellulitis is a disorder that affects the nervous tissue in the body and can lead to loss of sensation or movement | 112 (23.8%) |
| Cellulitis is a condition that affects blood vessels in the body, causing swelling and pain | 66 (14.0%) |
| Cellulitis is a digestive problem that affects the stomach and intestines, causing inflammation and ulcers | 14 (3.0%) |
| Effects of cellulitis on health | |
| Cellulitis can cause localized increases in temperature and redness | 144 (30.6%) |
| Cellulitis can cause pain, swelling, and redness in the affected area* | 240 (51.1%) |
| Cellulitis can lead to loss of movement or the ability to use the affected limb | 60 (12.8%) |
| Cellulitis can cause digestive disturbances and changes in sleep patterns | 26 (5.5%) |
| How can a doctor diagnose cellulitis? | |
| Visual examination of the skin and surrounding tissues for signs of swelling and redness | 91 (19.4%) |
| Blood tests to check for signs of inflammation and infection | 77 (16.4%) |
| Imaging tests such as X-rays or CT scans to evaluate internal tissues | 50 (10.6%) |
| Taking a sample of fluid from the affected area for analysis and identification of the infection | 27 (5.7%) |
| A doctor may use all of the above options* | 225 (47.9%) |
| What are the available treatments for cellulitis? | |
| Treatment with antibiotics to address potential bacterial infection | 108 (23.0%) |
| Use of anti-inflammatory medications to reduce pain and swelling | 68 (14.5%) |
| Rest and continuous elevation of the affected limb | 32 (6.8%) |
| In cases of severe skin breakdown, surgery may be necessary | 22 (4.7%) |
| All of the above options are possible* | 240 (51.1%) |
| Can cellulitis appear anywhere on the skin? | 384 (81.7%) |
| If left untreated, can the infection spread to other parts of the body? | 390 (83.0%) |
| If cellulitis is left untreated, can it quickly become a life-threatening condition? | 368 (78.3%) |
| Do you think cellulitis is a contagious disease? | 203 (43.2%) |
| Is cellulitis commonly caused by a common bacterial skin infection affecting the deeper layers of the skin and underlying tissues? | 399 (84.9%) |
| Characteristic | Aware about cellulitis | Multivariable regression | ||||
| No N=239 | Yes N=231 | p-value | OR | 95% CI | p-value | |
| Gender | 0.118 | |||||
| Male | 169 (48.7%) | 178 (51.3%) | ||||
| Female | 70 (56.9%) | 53 (43.1%) | ||||
| Age (years) | 0.031 | |||||
| 18 to 25 | 88 (50.6%) | 86 (49.4%) | Reference | Reference | ||
| 26 to 35 | 84 (57.9%) | 61 (42.1%) | 0.49 | 0.29, 0.81 | 0.006 | |
| 36 to 45 | 53 (50.5%) | 52 (49.5%) | 0.58 | 0.32, 1.04 | 0.07 | |
| 46 to 55 | 11 (31.4%) | 24 (68.6%) | 1.23 | 0.51, 3.07 | 0.65 | |
| > 55 | 3 (27.3%) | 8 (72.7%) | 3.22 | 0.71, 19.9 | 0.157 | |
| Educational levels | 0.003 | |||||
| Illiterate/primary | 7 (63.6%) | 4 (36.4%) | Reference | Reference | ||
| Middle school | 4 (36.4%) | 7 (63.6%) | 3.29 | 0.49, 27.1 | 0.236 | |
| Secondary | 61 (67.8%) | 29 (32.2%) | 1.22 | 0.28, 6.90 | 0.8 | |
| University | 152 (47.4%) | 169 (52.6%) | 2.85 | 0.69, 15.7 | 0.176 | |
| Diploma | 3 (75.0%) | 1 (25.0%) | 0.88 | 0.03, 12.2 | 0.929 | |
| Master's | 11 (42.3%) | 15 (57.7%) | 2.96 | 0.58, 19.2 | 0.213 | |
| PhD | 1 (14.3%) | 6 (85.7%) | 12.2 | 1.17, 315 | 0.061 | |
| Employment status | 0.002 | |||||
| Non-employed | 128 (58.4%) | 91 (41.6%) | Reference | Reference | ||
| Employed | 111 (44.2%) | 140 (55.8%) | 1.9 | 1.21, 3.01 | 0.006 | |
| Nationality | 0.491 | |||||
| Saudi | 239 (51.0%) | 230 (49.0%) | ||||
| Non-Saudi | 0 (0.0%) | 1 (100.0%) | ||||
| Characteristic | N (%) |
| Symptoms of cellulitis | |
| Pain in the affected area | 386 (82.1%) |
| Redness and warmth of the affected skin | 367 (78.1%) |
| Swelling of the skin | 358 (76.2%) |
| Fever and chills | 339 (72.1%) |
| Risk factors for developing cellulitis* | |
| Arterial diseases | 150 (31.9%) |
| Injury or cut | 322 (68.5%) |
| Obesity | 154 (32.8%) |
| Previous history of cellulitis | 242 (51.5%) |
| Skin conditions | 264 (56.2%) |
| Weakened immune system | 280 (59.6%) |
| Complication of cellulitis* | |
| Bloodstream infection | 312 (66.4%) |
| Bone infection | 196 (41.7%) |
| Endocarditis | 148 (31.5%) |
| Gangrene (tissue death) | 284 (60.4%) |
| Joint infection | 192 (40.9%) |
| Factors that reduce the risk of cellulitis | |
| Moisturizing the skin | 384 (82.9%) |
| Wearing properly fitting closed-toe shoes | 342 (73.4%) |
| Trimming nails carefully and correctly | 353 (75.9%) |
| Cleaning and caring for wounds | 416 (88.9%) |
| Paying attention to signs of infection in wounds | 417 (89.1%) |
| Ever diagnosed with cellulitis | Multivariable regression | |||||
| Characteristic | No N=382 | Yes N=88 | p-value | OR | 95% CI | p-value |
| Gender | 0.015 | |||||
| Male | 273 (78.7%) | 74 (21.3%) | Reference | Reference | ||
| Female | 109 (88.6%) | 14 (11.4%) | 0.73 | 0.37, 1.40 | 0.363 | |
| Age (years) | 0.017 | |||||
| 18 to 25 | 147 (84.5%) | 27 (15.5%) | Reference | Reference | ||
| 26 to 35 | 124 (85.5%) | 21 (14.5%) | 0.60 | 0.30, 1.18 | 0.139 | |
| 36 to 45 | 77 (73.3%) | 28 (26.7%) | 1.11 | 0.56, 2.19 | 0.772 | |
| 46 to 55 | 28 (80.0%) | 7 (20.0%) | 0.79 | 0.28, 2.03 | 0.632 | |
| >55 | 6 (54.5%) | 5 (45.5%) | 3.38 | 0.87, 12.5 | 0.068 | |
| Educational levels | 0.161 | |||||
| Illiterate/ primary | 7 (63.6%) | 4 (36.4%) | ||||
| Middle school | 9 (81.8%) | 2 (18.2%) | ||||
| Secondary | 74 (82.2%) | 16 (17.8%) | ||||
| University | 266 (82.9%) | 55 (17.1%) | ||||
| Diploma | 4 (100.0%) | 0 (0.0%) | ||||
| Master's | 18 (69.2%) | 8 (30.8%) | ||||
| PhD | 4 (57.1%) | 3 (42.9%) | ||||
| Employment status | <0.001 | |||||
| Non-employed | 194 (88.6%) | 25 (11.4%) | Reference | Reference | ||
| Employed | 188 (74.9%) | 63 (25.1%) | 2.54 | 1.38, 4.81 | 0.003 | |
| Nationality | 0.187 | |||||
| Saudi | 382 (81.4%) | 87 (18.6%) | ||||
| Non-Saudi | 0 (0.0%) | 1 (100.0%) | ||||
| Characteristic | N (%) |
| Healthcare provides sufficient attention to raising awareness of cellulitis | |
| Strongly disagree | 7 (1.5%) |
| Disagree | 16 (3.4%) |
| Neutral | 31 (6.6%) |
| Agree | 93 (19.8%) |
| Strongly agree | 323 (68.7%) |
| General awareness of cellulitis can contribute to better prevention | |
| Strongly disagree | 5 (1.1%) |
| Disagree | 3 (0.6%) |
| Neutral | 26 (5.5%) |
| Agree | 97 (20.6%) |
| Strongly agree | 339 (72.1%) |
| It is necessary to visit a doctor when noticing a rapid increase in skin redness, accompanied by elevated temperature, chills, swelling, and pain in the skin | |
| Strongly disagree | 3 (0.6%) |
| Disagree | 9 (1.9%) |
| Neutral | 28 (6.0%) |
| Agree | 79 (16.8%) |
| Strongly agree | 351 (74.7%) |
| More education and awareness of cellulitis should be provided | |
| Strongly disagree | 4 (0.9%) |
| Disagree | 2 (0.4%) |
| Neutral | 26 (5.5%) |
| Agree | 91 (19.4%) |
| Strongly agree | 347 (73.8%) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsStreptococcal Infections and Treatments · Antimicrobial Resistance in Staphylococcus · Antibiotic Use and Resistance
Introduction
Cellulitis is one of the most typical infections of the skin and soft tissues [1-3]. As a result of bacterial invasion through breaches in the skin barrier, cellulitis, which includes erysipelas, presents as an area of skin erythema, edema, and warmth. [4] Cellulitis is frequently misdiagnosed [5]; hence, other diagnoses ought to be considered. As a common skin infection, cellulitis affects both the epidermis and subcutaneous tissue, resulting in pain, edema, redness, and warmth in the affected area [6]. As many as 70-80% of cases involve the lower limbs, although it can occur in other body regions [7]. Gram-positive bacteria, such as Staphylococcus aureus and beta-hemolytic streptococcus, are responsible for most occurrences of cellulitis [6,8,9]. Cellulitis is a serious medical emergency that frequently necessitates hospitalization, can cause recurring illnesses, and can have long-term morbidity [10].
Cellulitis is characterized by erythema (redness), warmth to the touch, edema (swelling), and tenderness or discomfort in specific areas [11]. There may be a fever, chills, and malaise, along with lymphangitis and/or bacteremia [1,3]. Infection of burns, wounds, surgical incisions, or skin lesions is typically the cause of cellulitis [11,12]. Cellulitis can affect any part of the body in adults, but it typically affects the skin on the arms and lower legs. Children's cellulitis usually affects the lower limbs, periorbital infection, and extremities [13]. Numerous bacteria, most frequently Streptococcus pyogenes (Strep A), Staphylococcus aureus, or other beta-hemolytic streptococci, can cause cellulitis. Recurrent episodes of cellulitis affect about one-third of patients [14,15]. Low-dose antibiotics taken over an extended period of time have been demonstrated to lower the chance of recurrence, but successful preventative measures still need to be found [15].
Cellulitis can cause life-threatening and incapacitating consequences, such as necrotizing fasciitis, necrotizing hypodermitis, abscess development, septic shock, and, in severe cases, death, if diagnosis and treatment are delayed [16-18]. Determining the risk factors linked to cellulitis is essential for taking preventative action. Venous edema, lymphedema, skin disorders, traumatic injuries, leg ulcers, peripheral vascular disease, fungal infections, a history of cellulitis, and obesity are examples of risk factors [19,20]. Our research work aimed to measure awareness of the Al-Qunfudhah population of cellulitis health problems.
Materials and methods
Methodology
A descriptive cross-sectional study was conducted targeting all residents in Al-Qunfudhah, Saudi Arabia, during the period from January to March 2024. Adults aged above 18 years in Al-Qunfudhah Governorate were included, while children <18 years and who live outside Al-Qunfudhah Governorate and those who refused to participate or had missing questionnaire data, as well as participants who might have a conflict of interest, were excluded. Our study sample size of 501 was calculated with the aid of the Raosoft calculator (Raosoft, Inc., Seattle, WA) with a 5% margin of error and 95% confidence level (CI). Data were collected using a pre-structured online questionnaire that was initiated by the study authors with the help of experts and a literature review. A panel of three experts in the study field reviewed the initial questionnaire after its running in a pilot study to assess its content validity and applicability, and all suggested changes were applied. The final questionnaire included participants' demographic data, history of diagnosis with cellulitis, and associated complaints. The third section covered their awareness of cellulitis, including disease definition, causes, clinical symptoms, diagnosis methods, management methods, and associated complications, besides their source of information. The last section covered participants’ attitudes towards cellulitis and the role of health care staff. The final questionnaire was uploaded online using social media platforms by the researchers and their friends until no more new participants were included. Ethical approval was obtained from the Biomedical Research Ethics Committee of Umm Al-Qura University, Al-Qunfudhah, Saudi Arabia (approval number: HAPO-02-K-012-2024-02-1980).
Statistical analysis
The statistical analysis was conducted using RStudio software version 4.3.1 (Posit Software, PBC, Boston, MA, USA). Descriptive statistics were employed to summarize variables, including frequency distributions and percentages. Inferential statistics, including Pearson's chi-squared test and Fisher's exact test, were utilized to assess the associations between demographic variables and being aware of and diagnosed with cellulitis. Additionally, binary logistic regression analysis was performed to identify the independent predictors of being aware of and diagnosed with cellulitis in separate models. The models included variables that showed significant associations in the inferential analysis. Odds ratios (ORs) with 95% confidence intervals (CIs) were computed to quantify the strength and direction of associations. A significance level of p<0.05 was considered statistically significant.
Results
Sociodemographic characteristics
Initially, we received the responses of 501 participants. However, 31 records of participants aged <18 years were excluded. Therefore, a total of 470 records were analyzed. Among the respondents, the majority were male (n=347, 73.8%), and the highest proportion fell within the age range of 18 to 25 years (n=174, 37.0%). Regarding educational levels, the largest group consisted of individuals with a university education (n=321, 68.3%). In terms of employment status, a slight majority were employed (n=251, 53.4%). Additionally, almost all participants were Saudi nationals (n=469, 99.8%, Table 1).
Participants’ awareness of cellulitis
Less than half of the participants had ever heard about cellulitis (n=231, 49.1%). The highest proportion of respondents correctly identified cellulitis as a medical condition affecting the skin and soft tissues underneath it, typically caused by infection or injury (n=278, 59.1%). Additionally, the majority acknowledged that cellulitis can cause pain, swelling, and redness in the affected area (n=240, 51.1%). Among the participants, the most commonly recognized method for diagnosing cellulitis was all the available options (n=225, 47.9%), including visual examination of the skin and surrounding tissues for signs of swelling and redness, blood tests to detect inflammation and infection, imaging techniques such as X-rays or CT scans for internal tissue evaluation, and the collection of fluid samples from affected areas for infection analysis and identification. Regarding treatments, the highest proportion of respondents identified all the available treatments (n=240, 51.1%), including treatment with antibiotics to combat potential bacterial infections, the utilization of anti-inflammatory medications to alleviate pain and swelling, advocating rest and sustained elevation of the affected limb, and considering surgical intervention in instances of severe skin breakdown.
Moreover, the majority of participants correctly indicated that cellulitis can appear anywhere on the skin (n=384, 81.7%) and that it is commonly caused by a bacterial skin infection affecting deeper layers of the skin and underlying tissues (n=399, 84.9%). Additionally, a notable proportion of respondents correctly recognized that cellulitis is not a contagious disease (n=203, 43.2%). Furthermore, most participants recognized that if left untreated, cellulitis can spread to other parts of the body (n=390, 83.0%) and can quickly become a life-threatening condition (n=368, 78.3%, Table 2). In general, the most common sources of information regarding cellulitis were the Internet (n=312, 66.4%), followed by healthcare providers (n=186, 39.6%) and television (n=168, 35.7%, Figure 1).
Proportions of sources of information regarding cellulitis
Factors associated with awareness of cellulitis
In the analysis of factors associated with awareness of cellulitis, significant associations were found with age group (p=0.031), educational levels (p=0.003), and employment status (p=0.002). Notably, individuals aged 26 to 35 years displayed a lower proportion of awareness (n=61, 42.1%) compared to those aged 18 to 25 years. Similarly, the employed group exhibited a higher proportion of awareness (n=140, 55.8%) compared to the non-employed group. Regarding educational levels, individuals with a PhD demonstrated a significantly higher proportion of awareness (n=6, 85.7%) compared to those with an illiterate/primary education. In the multivariable analysis, individuals aged 26 to 35 years had lower odds of being aware of cellulitis compared to those aged 18 to 25 years (OR=0.49, 95% CI: 0.29 to 0.81, p=0.006). Furthermore, employed individuals had higher odds of awareness compared to non-employed individuals (OR=1.90, 95% CI: 1.21 to 3.01, p=0.006, Table 3).
Participants’ knowledge of different aspects of cellulitis
The highest level of awareness of symptoms of cellulitis was about recognizing pain in the affected area (n=386, 82.1%) and redness and warmth of the affected skin (n=367, 78.1%). Additionally, participants demonstrated strong knowledge of factors that reduce the risk of cellulitis, including cleaning and caring for wounds (n=416, 88.9%) and paying attention to signs of infection in wounds (n=417, 89.1%). Notably, a substantial proportion of respondents demonstrated awareness of potential complications, with 66.4% (n=312) recognizing bloodstream infection, 60.4% (n=284) acknowledging gangrene (tissue death), and 41.7% (n=196) identifying bone infection. Regarding risk factors for developing cellulitis, participants displayed considerable awareness, with injury or cut being the most recognized risk factor (n=322, 68.5%), followed by a weakened immune system (n=280, 59.6%) and skin conditions (n=264, 56.2%, Table 4).
Prevalence of cellulitis and the associated factors
Among the participants, 88 respondents had ever been diagnosed with cellulitis (18.7%, Figure 2). Of those who were diagnosed with cellulitis, the most common sites for cellulitis were the lower limbs (n=46, 52.4%) and the upper limbs (n=40, 45.2%), whereas only 2.4% had cellulitis around the eyes. Notably, a higher proportion of males (n=74, 21.3%) were diagnosed with cellulitis compared to females (n=14, 11.4%, p=0.015). Additionally, employed individuals exhibited a significantly higher proportion of cellulitis diagnoses (n=63, 25.1%) compared to non-employed individuals (n = 25, 11.4%). Additionally, the diagnosis of cellulitis increased significantly with advanced age, from 15.5% (n=27) among participants aged 18 to 25 years and 14.5% (n=21) for those aged 26 to 35 to 26.7% (n=28), 20.0% (n=7), and 45.5% (n=5) among 36 to 45 years, 46 to 55, and >55 years, respectively (p=0.017). Importantly, on the multivariable analysis, only employment status was a significant predictor of cellulitis diagnosis, where employed participants were more likely to experience cellulitis compared to their non-employed counterparts (OR=2.54, 95% CI: 1.38 to 4.81, p=0.003, Table 5).
Proportions of participants who had ever been diagnosed with cellulitis
Attitudes towards cellulitis
The internal consistency of items related to participants’ attitudes (n=4) was 0.788 as per the outcomes of the Cronbach’s alpha test, indicating good reliability. In Table 6, participants' attitudes towards cellulitis are outlined. The majority strongly agreed that healthcare provides sufficient attention to raising awareness of cellulitis (n=323, 68.7%) and that general awareness of cellulitis can contribute to better prevention (n=339, 72.1%). Additionally, a significant proportion strongly agreed that it is necessary to visit a doctor when noticing rapid increases in skin redness, accompanied by elevated temperature, chills, swelling, and pain in the skin (n=351, 74.7%). Moreover, the majority strongly agreed that more education and awareness of cellulitis should be provided (n=347, 73.8%, Table 6).
Discussion
The current study aimed to assess the public awareness of cellulitis in the Al-Qunfudhah region, Saudi Arabia. In cases where patients lack knowledge of cellulitis, they are unlikely to alter risk factors to avoid recurrent bouts [21]. A single, brief qualitative study with secondary care patients receiving cellulitis treatment has been conducted. Participants expressed not getting enough assistance or information, as well as not always knowing what to do to stop recurrences [22]. This can be the result of conflicting advice on cellulitis prevention. The current study also aimed to investigate the prevalence and characteristics of cellular tissue inflammation in the Al-Qunfudhah region.
With regard to the prevalence of cellulitis, the current study revealed that about one-fifth of the participants had ever been diagnosed with cellulitis, mainly in their extremities (lower limbs and upper limbs), which is in line with the literature that revealed cellulitis usually affects the lower extremities more commonly compared with other parts of the body [23,24]. Old age, male gender, and employment were significantly associated with a higher frequency of cellulitis among study participants. Literature shows that cellulitis is observed most frequently among middle-aged and older adults, which is consistent with the current study findings [9,25]. Worldwide, about 200 cases of cellulitis per 100,000 patients are registered per year, which is much lower than assessed in the current study [6]. A much lower prevalence was reported by Hailu et al. [26], where an incidence rate of 1.8% was assessed, but similar to the current study, most patients were males. Also, in the USA, 1.4% of cellulitis cases are noted in hospital admissions [27]. In Saudi Arabia, the incidence of skin and soft-tissue infections was 1.67% [28]. Another study revealed that cellulitis accounted for 23.5% of general surgical admission during Hajj Pilgrims [29]. The estimated high prevalence in the current study may be due to subjective methods used for identifying the disease frequency based on participants' judgments, who may overreport any skin condition or dermatitis as cellulitis.
With regard to public awareness of cellulitis, the current study revealed that about half of the study participants heard about cellulitis, with most participants correctly defining the condition. Also, about half of them identified the clinical presentation, diagnostic techniques, management methods, and associated complications of neglected cases. Pain, local redness, and warmth were identified by more than three-fourths of the study participants. Also, bloodstream infections were the most commonly associated complication with tissue death. The Internet, healthcare providers, and TV were the main sources of information about cellulitis. Old age, high education, and employment were the significant factors associated with high awareness levels. In contrast to the current study, Teasdale et al. [21] reported low awareness of cellulitis among their study participants. Also, the study revealed that participants were astonished that they had never heard of cellulitis and that they had not received advice or leaflets giving self-care information. Some sought information from the Internet and found this confusing. Another study by Qadir et al. [30] among students revealed that 93.5% of students knew that cellulitis was a bacterial disease, 83.1% knew that it could be treated medically, and 5.1% reported surgical treatment. In Saudi Arabia, no previous studies assessed public awareness of cellulitis, but Alshaalan et al. [31] assessed public awareness of skin diseases, and none of them reported cellulitis as one of the skin-related diseases. Regarding public attitudes towards cellulitis, it was found that most of the study participants agreed with the role of healthcare staff in providing more information to raise public awareness of the disease, which will help in disease prevention with a lower burden. This manuscript offers some strength points as it is the first work to discuss awareness of cellulitis health problems in a specific area (Al-Qunfudhah Governorate), raising their knowledge, especially in high-risk patients. Meanwhile, it is important to explore the leading role of healthcare provider teams in upgrading the culture of the Al-Qunfudhah population regarding the care of cellulitis cases.
Study limitations
This study encountered several limitations. Firstly, it used a small sample size of participants due to the limited population of Al-Qunfudhah Governorate, which may limit its generalization. Secondly, it is self-reported, which may be affected by sample bias because it depends on social media, which may be influenced by the availability of the Internet and social media accounts. Thirdly, the well-structured questionnaire limits the depth of participants' understanding of knowledge and attitudes towards cellulitis. Lastly, this study cannot differentiate between variables' causal relationships, which limits the investigation of the association between cause and effect.
Conclusions
The current study revealed that the estimated prevalence of cellulitis was higher than reported in the literature due to the subjective assessment used in the current study. Additionally, the study showed high awareness among participants regarding all aspects of cellulitis, including the nature of the disease, clinical presentation, complications, diagnosis, and management. Higher education and employment were associated with higher awareness levels. Study participants emphasized the role of healthcare staff in improving public awareness and perception of cellulitis to minimize the disease-associated burden. Periodic health education campaigns are recommended to improve public healthcare awareness of skin-related disorders and preventable diseases such as cellulitis. More effort should be made by healthcare staff, as they are a trusted source of information for the community.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Diagnosis and management of cellulitis Clin Med (Lond) Sullivan T de Barra E 1601631820182962602210.7861/clinmedicine.18-2-160PMC 6303460 · doi ↗ · pubmed ↗
- 2Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the Infectious Diseases Society of America Clin Infect Dis Stevens DL Bisno AL Chambers HF 105259201410.1093/cid/ciu 29624947530 · doi ↗ · pubmed ↗
- 3Cellulitis Infect Dis Clin North Am Bystritsky RJ 49603520213349487410.1016/j.idc.2020.10.002 · doi ↗ · pubmed ↗
- 4Bilateral lower limbs cellulitis: a narrative review of an overlooked clinical dilemma Int J Gen Med Chuang YC Liu PY Lai KL Tseng CH 556755781520223570773910.2147/IJGM.S 356852 PMC 9191579 · doi ↗ · pubmed ↗
- 5Prevalence of misdiagnosis of cellulitis: a systematic review and meta-analysis J Hosp Med Cutler TS Jannat-Khah DP Kam B Mages KC Evans AT 2542611820233618961910.1002/jhm.12977 · doi ↗ · pubmed ↗
- 6Cellulitis: a review JAMA Raff AB Kroshinsky D 32533731620162743444410.1001/jama.2016.8825 · doi ↗ · pubmed ↗
- 7Lower limb cellulitis and its mimics: part I. Lower limb cellulitis J Am Acad Dermatol Hirschmann JV Raugi GJ 16311267201210.1016/j.jaad.2012.03.02422794815 · doi ↗ · pubmed ↗
- 8Cellulitis: diagnosis and management Dermatol Ther Bailey E Kroshinsky D 2292392420112141061210.1111/j.1529-8019.2011.01398.x · doi ↗ · pubmed ↗