Moderate Ischemic Mitral Regurgitation with Ejection Fraction <40% Undergoing Concomitant Mitral Valve Repair during Revascularization: A Single-Center Observational Study
Ye Yang, Fangyu Liu, Yulin Wang, Limin Xia, Chunsheng Wang, Qiang Ji

TL;DR
This study found that patients with moderate ischemic mitral regurgitation and low heart function had similar surgical and midterm outcomes to those with better heart function, though they required more prolonged ventilation.
Contribution
The study provides new insights into the surgical outcomes of patients with moderate ischemic mitral regurgitation and depressed left ventricular function.
Findings
Patients with EF <40% had similar surgical mortality to those with EF ≥40%.
EF <40% was independently associated with prolonged ventilation.
Midterm survival was not significantly different between the two groups.
Abstract
Numerous studies have examined the therapeutic effects of mitral valve repair during revascularization on moderate ischemic mitral regurgitation (IMR), as well as the incremental benefit of subvalvular repair alongside an annuloplasty ring. However, the impact of depressed left ventricular (LV) function on the surgical outcome of patients with moderate IMR has been rarely investigated. The aims of this single-center, retrospective, observational study were firstly to evaluate short- and medium-term outcomes in this patient group after undergoing mitral valve repair during revascularization, and secondly to assess the impact of depressed LV function on surgical outcomes. A total of 272 eligible patients who had moderate IMR and underwent concomitant mitral valve repair and revascularization from January 2010 to December 2017 were included in the study. These patients were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
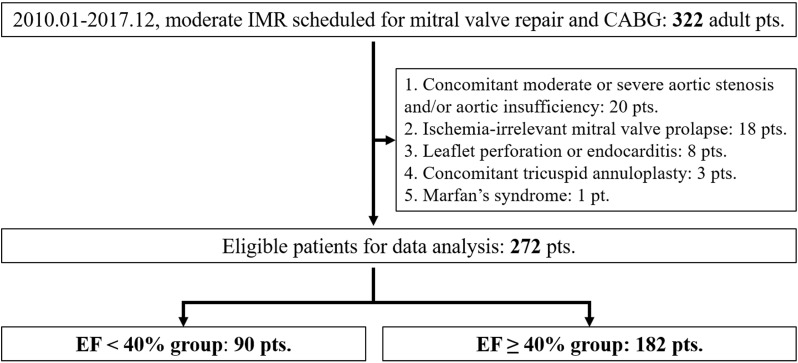 Fig. 1
Fig. 1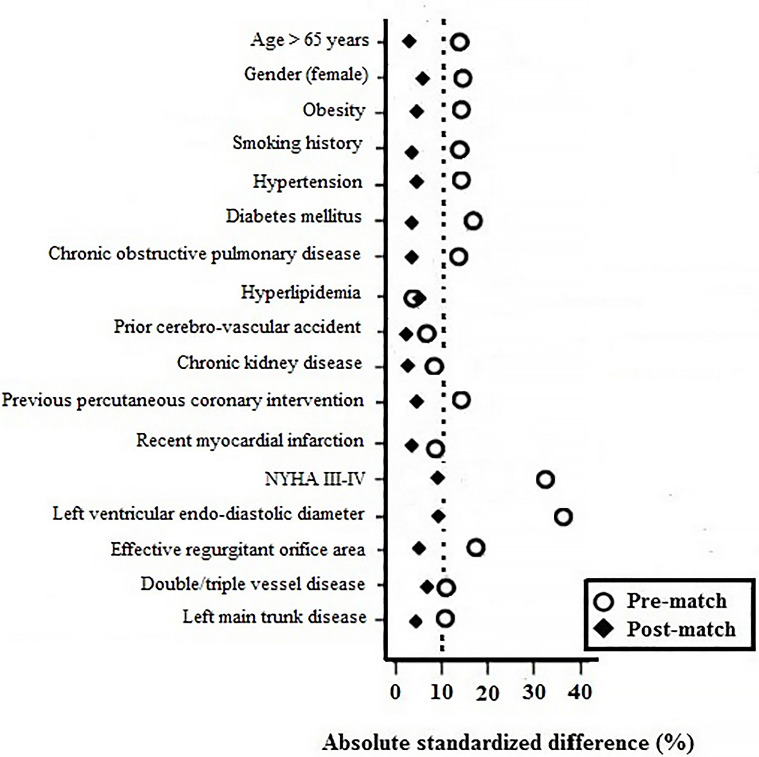 Fig. 2
Fig. 2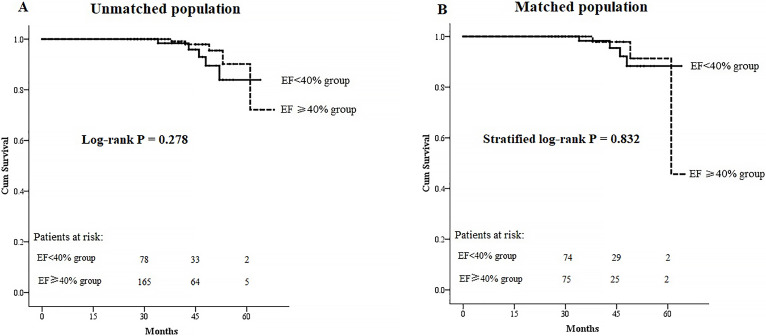 Fig. 3
Fig. 3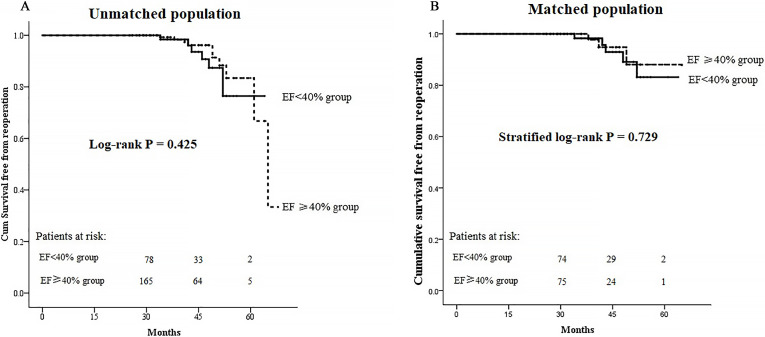 Fig. 4
Fig. 4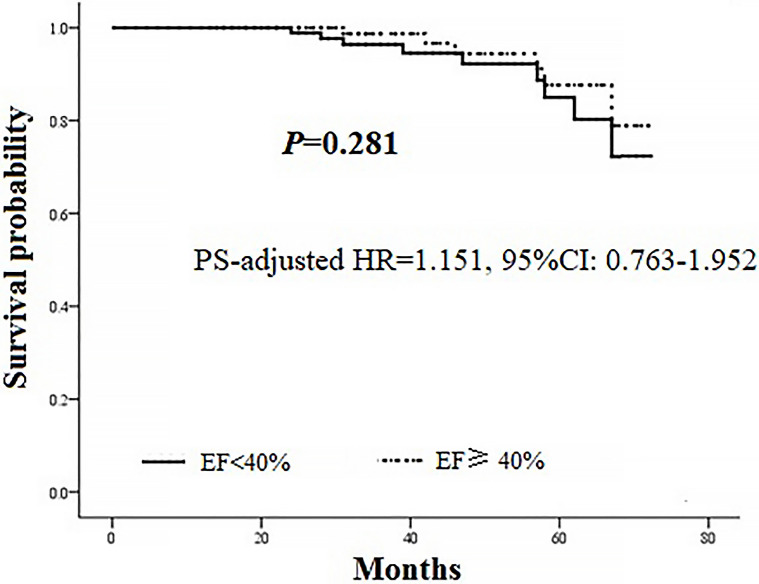 Fig. 5
Fig. 5| Variables | Unmatched population | Matched population | |||||
| EF | EF |
| EF | EF |
| ||
| Demographics | |||||||
| Age (years) | 64.1 | 65.3 | 0.254 | 64.4 | 65.0 | 0.630 | |
| Gender (female) | 15, 16.7% | 35, 19.2% | 0.607 | 14, 17.1% | 15, 18.3% | 0.838 | |
| Obesity | 14, 15.6% | 26, 14.3% | 0.781 | 12, 14.6% | 13, 15.9% | 0.828 | |
| Smoking history | 42, 46.7% | 78, 42.9% | 0.552 | 38, 46.3% | 36, 43.9% | 0.754 | |
| Concomitant diseases | |||||||
| Hypertension | 47, 52.2% | 94, 51.6% | 0.929 | 43, 52.4% | 42, 51.2% | 0.876 | |
| Diabetes | 40, 44.4% | 75, 41.2% | 0.611 | 37, 45.1% | 35, 42.7% | 0.753 | |
| Hyperlipidemia | 20, 22.2% | 41, 22.5% | 0.955 | 18, 22.0% | 17, 20.7% | 0.849 | |
| CKD | 8, 8.9% | 17, 9.3% | 0.903 | 7, 8.5% | 9, 11.0% | 0.599 | |
| Prior CVA | 7, 7.8% | 15, 8.2% | 0.895 | 6, 7.3% | 7, 8.5% | 0.773 | |
| COPD | 7, 7.8% | 21, 11.5% | 0.337 | 6, 7.3% | 9, 11.0% | 0.416 | |
| Preoperative cardiac status | |||||||
| Recent MI | 38, 43.3% | 75, 41.2% | 0.873 | 36, 43.9% | 34, 41.5% | 0.752 | |
| Previous PCI | 15, 16.7% | 29, 15.9% | 0.877 | 13, 15.9% | 12, 14.6% | 0.828 | |
| NYHA III–IV | 32, 35.6% | 41, 22.5% | 0.023 | 30, 36.6% | 22, 26.8% | 0.179 | |
| EF | 0.38 | 0.49 | 0.38 | 0.48 | |||
| LVEDD (mm) | 64.5 | 59.2 | 64.1 | 62.0 | 0.055 | ||
| EROA ( | 16 (12, 18) | 16 (12, 17) | 0.452 | 16 (12, 18) | 16 (12, 17) | 0.408 | |
| Extent of CAD | |||||||
| 2-vessel | 12, 13.3% | 28, 15.4% | 0.653 | 11, 13.4% | 12, 14.6% | 0.822 | |
| 3-vessel | 78, 86.7% | 154, 84.6% | 71, 86.6% | 70, 85.4% | |||
| LM | 26, 28.9% | 54, 29.7% | 0.894 | 24, 29.3% | 25, 30.5% | 0.865 | |
| EuroSCORE | 7 (5, 8) | 7 (5, 7) | 0.012 | 7 (5, 8) | 7 (5, 8) | 0.201 | |
| Variables | Unmatched population | Matched population | |||||
| EF | EF |
| EF | EF |
| ||
| CPB time (min) | 97.8 | 91.7 | 0.071 | 97.5 | 93.4 | 0.194 | |
| ACC time (min) | 77.5 | 76.8 | 0.721 | 77.3 | 76.5 | 0.663 | |
| Number of grafts | 3 (3, 3) | 3 (3, 3) | 0.653 | 3 (3, 3) | 3 (3, 3) | 0.712 | |
| Use of left IMA | 89, 98.9% | 180, 98.9% | 0.993 | 82, 100% | 81, 98.8% | 0.316 | |
| Use of vein graft | 88, 97.8% | 177, 97.3% | 0.797 | 81, 98.8% | 81, 98.8% | ||
| Use of RA | 5, 5.6% | 6, 3.3% | 0.514 | 5, 6.1% | 3, 3.7% | 0.720 | |
| Type of ring | |||||||
| Band | 14, 15.6% | 26, 14.3% | 0.781 | 11, 13.4% | 12, 14.6% | 0.822 | |
| Complete-ring | 76, 84.4% | 156, 85.7% | 71, 86.6% | 70, 85.4% | |||
| Size of complete-ring | 28 (28, 30) | 28 (26, 30) | 0.572 | 28 (28, 30) | 28 (28, 30) | 0.718 | |
| Repair techniques | |||||||
| Annuloplasty alone | 64, 71.1% | 142, 78.1% | 0.667 | 61, 74.4% | 63, 76.8% | 0.972 | |
| Plus sub-valvular | 11, 12.3% | 17, 9.3% | 9, 11.0% | 9, 11.0% | |||
| Plus leaflet | 13, 14.4% | 20, 11.0% | 11, 13.4% | 9, 11.0% | |||
| All | 2, 2.2% | 3, 1.6% | 1, 1.2% | 1, 1.2% | |||
| TEE data | |||||||
| No or trace MR | 81, 90.0% | 162, 89.0% | 0.804 | 76, 92.7% | 75, 91.5% | 0.773 | |
| Mild MR | 9, 10.0% | 20, 11.0% | 6, 7.3% | 7, 8.5% | |||
| Variables | Unmatched population | Matched population | |||||
| EF | EF |
| EF | EF |
| ||
| In-hospital | |||||||
| Number of patients | 90 | 182 | 82 | 82 | |||
| Surgical mortality | 8, 8.9% | 6, 3.3% | 0.076 | 7, 8.5% | 2, 2.4% | 0.167 | |
| CABG-associated MI | 3, 3.3% | 5, 2.7% | 0.722 | 2, 2.4% | 1, 1.2% | ||
| Low cardiac output | 8, 8.9% | 5, 2.7% | 0.034 | 7, 8.5% | 2, 2.4% | 0.167 | |
| IABP support | 9, 10.0% | 7, 3.8% | 0.042 | 8, 9.8% | 3, 3.7% | 0.119 | |
| Redo for bleeding | 3, 3.3% | 6, 3.3% | 0.999 | 2, 2.4% | 2, 2.4% | ||
| New-onset stroke | 4, 4.4% | 5, 2.7% | 0.484 | 3, 3.7% | 2, 2.4% | ||
| Prolonged ventilation | 12, 13.3% | 10, 5.5% | 0.026 | 11, 13.4% | 3, 3.7% | 0.025 | |
| DSWI | 2, 2.2% | 3, 1.6% | 0.667 | 1, 1.2% | 1, 1.2% | ||
| AKI requiring hemodialysis | 6, 6.7% | 5, 2.7% | 0.187 | 5, 6.1% | 2, 2.4% | 0.443 | |
| ICU stay (d) | 4 (2, 5) | 2 (1, 3) | 3 (2, 4) | 2 (2, 3) | 0.012 | ||
| Postoperative hospital stay (d) | 8 (7, 10) | 7 (6, 8) | 8 (7, 10) | 7 (6, 9) | 0.009 | ||
| Follow-up | |||||||
| Number of patients | 78 | 165 | 74 | 75 | |||
| Follow-up time (months) | 42 (36, 48) | 42 (34, 50) | 0.318 | 42 (37, 48) | 43 (36, 50) | 0.101 | |
| At 30-month | |||||||
| Moderate or more MR | 19, 24.4% | 35, 21.2% | 0.582 | 18, 24.3% | 16, 21.3% | 0.664 | |
| NYHA III–IV | 11, 14.1% | 19, 11.5% | 0.567 | 9, 12.2% | 8, 10.7% | 0.774 | |
| Outcomes | Univariate analysis | Multivariate analysis* | ||
| OR (95% CI) |
| OR (95% CI) |
| |
| Surgical mortality | 3.733 (0.752–9.542) | 0.086 | 2.967 (0.712–7.245) | 0.138 |
| CABG-associated MI | 2.025 (0.580–7.780) | 0.560 | / | |
| Low cardiac output | 3.562 (0.724–8.939) | 0.105 | 3.134 (0.658–8.623) | 0.214 |
| Redo for bleeding | 1.001 (0.407–6.274) | 0.987 | / | |
| New-onset stroke | 1.519 (0.547–6.338) | 0.650 | / | |
| Prolonged ventilation | 3.538 (1.116–7.215) | 0.027 | 2.814 (1.321–6.151) | 0.031 |
| IABP support | 2.847 (0.728–7.141) | 0.183 | 2.634 (0.564–6.571) | 0.310 |
| DSWI | 1.001 (0.123–7.263) | 0.991 | / | |
| AKI requiring hemodialysis | 2.529 (0.589–7.790) | 0.196 | 2.428 (0.634–5.578) | 0.283 |
| Moderate or more MR at 30 months | 1.196 (0.558–2.623) | 0.700 | / | |
| NYHA III-IV at 30 months | 1.162 (0.469–3.189) | 0.801 | / | |
- —Zhongshan Hospital Fudan University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Cardiac, Anesthesia and Surgical Outcomes · Cardiac Structural Anomalies and Repair
1. Introduction
Ischemic mitral regurgitation (IMR) affects over two million individuals in the United States and is the most frequent etiology of functional mitral regurgitation (MR) [1]. IMR is provoked by acute or chronic coronary artery disease. The tethering mitral leaflets appear with unsatisfactory coaptation, predominantly as a result of disadvantageous left ventricular (LV) remodeling with annular dilatation [2]. The risks of death and heart failure increase with the development of IMR and increase further with the severity of regurgitation [3]. Because the shaping of adverse LV remodeling may vary, IMR also shows diversity according to distinct LV injuries. Even when small ischemic or infarcted areas appear, especially in the posterolateral region, obvious IMR occurs despite the ventricle showing good performance overall [4]. Dynamic, paroxysmal MR patterns often exist in such patients, who are thought to benefit from surgery. Some patients also have severely dilated ventricles, usually accompanied by low ejection fraction (EF). The outcomes for these patients are often disappointing and unpredictable [5]. EF is an evaluation index for LV systolic performance and has decision-making value in the treatment of IMR [6, 7]. Ellis et al. [8] conducted an observational study of 3-year survival following percutaneous coronary intervention in IMR patients. These authors found that depressed LV function (EF 40%) may be related to increased 3-year mortality.
According to the guidelines from the American Association for Thoracic Surgery, mitral valve repair using an undersized ring annuloplasty is recommended as “may be considered” for moderate IMR during surgical revascularization [9]. An increasing number of studies have reported that coronary artery bypass grafting (CABG) plus simultaneous mitral valve repair could be an effective surgical plan for moderate IMR, although recurrent MR may occur. Surgery eliminates MR immediately following the operation, reverses LV remodeling, ameliorates LV performance, and allows a more reliable repair of moderate IMR [10, 11, 12]. The results of our previous study showed that concomitant mitral valve repair may improve New York Heart Association (NYHA) functional class and reduce residual MR, with no increase in surgical mortality, morbidity, or follow-up deaths [13].
Previous studies assessed mainly the therapeutic effects of revascularization along with mitral valve repair in moderate IMR patients, and the incremental benefits of subvalvular repair plus an annuloplasty ring. However, the impact of depressed LV function on surgical outcomes of patients with moderate IMR has not been determined. Based on our experience, we hypothesize that concomitant mitral valve repair during revascularization is safe, feasible, and effective in patients with moderate IMR and EF 40%. The aims of this present study included the evaluation of short- and medium-term outcomes for patients with moderate IMR and EF 40% who received mitral valve repair during CABG, and the assessment of the impact of depressed LV function on surgical outcomes.
2. Materials and Methods
2.1 Patient Characteristics
Consecutive patients with moderate IMR and scheduled for mitral valve repair and simultaneous CABG between January 2010 to December 2017 were identified from medical records. The inclusion criteria were: (1) previous myocardial infarction (MI) indicated by regional wall motion abnormalities revealed by echocardiography, or as detected by electrocardiogram; (2) sinus rhythm; and (3) no structural mitral valve abnormalities. The exclusion criteria were: (1) echocardiographic evidence and/or clinical manifestations of other structural heart diseases; (2) organic mitral apparatus abnormalities; (3) unstable global clinical status; (4) atrial fibrillation that was not appropriate for this study because it was reported to cause atrioventricular valve regurgitation [14]; (5) concomitant tricuspid annuloplasty; and (6) emergency surgery.
Within 3 days before surgery, routine transthoracic echocardiography was performed to assess the severity and mechanism of MR. The IMR level was classified as mild (narrow central jet area less than 20% of left atrium (LA) and vena contracta less than 3.0 mm under Doppler), moderate (regurgitant volume less than 30 mL, effective regurgitant orifice area (EROA) less than 20 , and regurgitant fraction less than 50%), or severe (regurgitant volume over 30 mL, EROA over 20 , and regurgitant fraction over 50%). MR suggested by echocardiography was evaluated by two independent professional readers, with a third reader used when discrepancies arose. Examinations were performed according to current guidelines [15].
All procedures began with a midline sternotomy. The detailed protocol for on-pump CABG was described in a previous study [16]. After grafting, the quality of anastomosis was evaluated during the operation using a transit-time flow probe. Technical details regarding our institutional approach to mitral valve repair were described previously [17]. After weaning off the bypass, intraoperative transesophageal echocardiography was performed immediately to determine the quality of mitral valve repair. If moderate or more residual MR was observed, a repeat procedure was executed immediately.
2.2 Study Protocol
This single-center, retrospective, observational study received approval from the medical ethics committee of Zhongshan Hospital, Fudan University (No. B2022-024R), and followed the principles of the Declaration of Helsinki. Similar to a previous report [8] in which an EF of 40% was used as the cut-off point to discriminate depressed LV function, EF 40% was used in the present study to define depressed LV function. All patients included in this study were assigned to either the EF 40% group or the EF 40% group. Baseline characteristics and surgical data were extracted for all patients, and in-hospital and follow-up outcomes were compared between groups. An electronic in-hospital database was used to access baseline characteristics, as well as in-hospital outcomes. A standard case report form was used to record the data. Enrolled patients were routinely followed up postoperatively at three and six months, and afterward at 6-month intervals. Telephone interviews and clinical visits were used to obtain follow-up data. A clinical visit was scheduled if recrudescent symptoms of coronary artery disease or questionable symptoms of MR appeared during the follow-up.
In-hospital outcomes consisted of surgical mortality and major postoperative morbidity. Death during the same hospitalization or within 30 days after surgery would be recognized as surgical mortality [18]. Major postoperative morbidities were CABG-associated MI, prolonged ventilation, low cardiac output, new-onset stroke, acute kidney injury requiring hemodialysis, redo for bleeding, and deep sternal wound infection (DSWI). CABG-associated MI was diagnosed as elevation of cardiac troponin T (cTnT) values to 10 times the 99th percentile of the upper reference range using one or more of the following methods: (1) new onset pathological Q wave or left bundle branch block recorded with electrocardiography; (2) new occlusion of graft or native coronary artery documented by angiography; (3) new viable myocardium loss or abnormal regional wall motion manifested by imaging [19]. Low cardiac output was recorded when an intra-aortic balloon pump (IABP) and/or positive inotropic agent support became necessary for difficulty in weaning off the cardiopulmonary bypass, or when longer than 30 mins was required to maintain the cardiac index 2.2 L/min/ with systolic blood pressure 90 mmHg after the patient returned to intensive care unit (ICU) [20]. Postoperative prolonged ventilation was identified as when the mechanical ventilation exceeded 48 hours, or when re-intubation was required after surgery. New-onset stroke was considered to be a new onset of global or focal brain dysfunction occurring over 24 hours, or permanent neurological damage persisting until either discharge or death [21]. The definition of DSWI was the same as in our previous study [22]. The duration of the postoperative hospital stay and of the ICU stay were counted.
Follow-up outcomes included all-cause death, reoperation (including repeat mitral valve procedure and repeat revascularization), moderate or severe MR, and NYHA functional class. All-cause mortality is the most unbiased and robust index and was therefore selected rather than cardiac mortality. This helped to avoid misinterpretation of the cause of death due to unreliable medical records. The minimum follow-up time in this study was 30 months. Follow-up information obtained at 30 months after surgery was used for the analysis of NYHA classification and residual MR.
2.3 Statistical Analysis
The normal distribution of variables was determined using the Shapiro-Wilks test. An independent-samples t-test was used while comparing normally distributed continuous variables between groups, which were exhibited as the mean standard deviation (SD). The Wilcoxon rank sum test was performed on non-normally distributed continuous variables, which were exhibited as the median and interquartile range (IQR). Categorical variables were exhibited as frequencies and percentages, which were compared using the Chi-square test between groups, or using the Fisher’s exact test when the expected frequency was 5.
The propensity score (PS) was generated for each patient using a multivariable
logistic regression model to control potential confounders in the dataset. The PS
was performed according to 17 independent variables, with LV function-based
grouping (EF 40% vs. EF 40%) used as a binary dependent
variable. Demographics, complications, cardiac status (except for EF and
EuroSCORE), and EROA were included in the 17 variables. The model was verified
with the Hosmer-Lemeshow goodness-of-fit method. The greedy-matching
algorithm was used with a caliper width of 0.2 of the SD of the logit of the PS,
thus implementing a 1:1 nearest-neighbor. Other details of the PS matching could
refer to our former study [16]. After matching, paired t-test was used
for normally distributed continuous variates. The Wilcoxon signed-rank
test was used for non-normally distributed continuous variates.
McNemar’s test was used for categorical variates. Conditional
mixed-effects logistic regression analysis was applied to evaluate the effect of
grouping as independent risk factors. The Kaplan-Meier method was
applied to estimate the overall survival and survival free from reoperation with
the stratified log-rank test used to compare survival curves in the PS-matched
population. Between the two matched groups, the Cox regression model was
utilized to estimate the PS-adjusted hazard ratio (HR) and 95% confidence
interval (CI) of midterm mortality. Statistical analysis was performed using SPSS
version 22.0 (SPSS Inc., Chicago, IL, USA), with a two-sided p-value
0.05 considered to represent statistical significance.
3. Results
3.1 Study Population
A total of 5336 consecutive patients in our department received surgical revascularization with or without other concomitant cardiac surgery between January 2010 to December 2017. Amongst these, 322 patients were eligible according to the inclusion criteria. During patient enrollment, as shown in Fig. 1, 50 patients were ruled out, leaving 272 patients for data analysis. Of these, 90 patients were enrolled in the EF 40% group, and 182 patients in the EF 40% group.
Flow chart for the patient enrollment. IMR, ischemic mitral regurgitation; CABG, coronary artery bypass grafting; pts, patients; EF, ejection fraction.
Baseline characteristics of the patients are shown in Table 1. Patients in the EF 40% group had a larger LV endo-diastolic diameter (64.5 7.8 mm vs. 59.2 7.1 mm, *p * 0.001), a higher proportion of patients in NYHA class III–IV (p = 0.023), and a higher additive EuroSCORE (p = 0.012) compared with patients in the EF 40% group. Baseline characteristics were otherwise similar between groups.
Surgical data are shown in Table 2. No significant difference was discovered between groups in terms of cardiopulmonary bypass time or aortic cross-clamping time. The number of grafts was also similar between the two groups (p = 0.653). Annuloplasty was performed on 232 patients using a downsized complete rigid ring for 84.4% of the EF 40% group and 85.7% of the EF 40% group (p = 0.781). No significant difference was apparent for the type of repair techniques used in the two groups (p = 0.667). Transesophageal echocardiography examination revealed that moderate or severe MR was not found in either group immediately after weaning off the bypass.
3.2 Propensity Score Matching Cohorts
To compare baseline characteristics between the two groups, we performed bivariate analyses. The propensity score was calculated based on 17 predefined variables. The model’s Hosmer-Lemeshow goodness of fit was 4.65 (p = 0.793). Furthermore, good discrimination power was achieved with an area under the curve of 0.78 (95% CI, 0.65–0.84, p = 0.019) of the receiver operating curve. Ultimately, 82 patient pairs were matched at a 1:1 ratio. After matching, Fig. 2 shows that the absolute standardized differences were all 10%, which indicates adequate balance. Except for EF, the matched cohorts were comparable for baseline characteristics (Table 1). In addition, no significant difference was found with regard to surgical characteristics between the two matched groups.
Pre-match and post-match absolute standardized differences for baseline characteristics. NYHA, New York heart assessment functional classification.
3.3 In-Hospital Outcomes
The in-hospital outcomes are shown in Table 3. Patients in the EF 40% group had slightly higher surgical mortality, but this reached no statistical significance (p = 0.076). More patients in the EF 40% group developed low cardiac output (8.9% vs. 2.7%, p = 0.034) and received intra-aortic balloon pump support (10.0% vs. 3.8%, *p *= 0.042) compared to patients in the EF 40% group. More patients in the EF 40% group also developed prolonged ventilation (13.3% vs. 5.5%, p = 0.026). Major postoperative morbidity was otherwise similar between the two groups, including CABG-associated MI, redo for bleeding, new-onset stroke, DSWI, and acute kidney injury requiring hemodialysis. The matched groups of patients showed similar major postoperative morbidity, with the exception of prolonged ventilation. Patients in the EF 40% group had longer ICU stays and longer postoperative hospital stays compared with those in the EF 40% group, both before and after PS matching.
The effects of grouping (matched EF 40% group vs. matched EF 40% group) on major postoperative morbidity and surgical mortality are shown in Table 4. Conditional mixed-effects logistic regression analysis revealed that EF 40% had an independent impact on postoperative prolonged ventilation (OR = 2.814, 95% CI 1.321–6.151, p = 0.031). However, EF 40% was not an independent risk factor for surgical mortality (OR = 2.967, 95% CI 0.712–7.245, p = 0.138), nor was it an independent risk factor for other major postoperative morbidities.
Table 4.: Impacts of EF <40% on outcomes in the matched population.
3.4 Follow-up Outcomes
Follow-up visits were completed with 243 patients in total. The median follow-up time was 42 months (IQR, 34–50), with the shortest follow-up time being 30 months. At the 30-month follow-up, the incidence of moderate or more MR and the proportion of NYHA class III and IV did not differ either before or after matching (Table 3). As shown in Fig. 3, similar cumulative survival was shown both before and after PS matching (log-rank p = 0.278, stratified log-rank p = 0.832, respectively). No significant difference in cumulative survival free from reoperation was found between the two groups, either before or after matching (log-rank p = 0.425, stratified log-rank p = 0.729, respectively) (Fig. 4). Finally, Cox regression analysis was utilized to estimate the follow-up death in the matched cohorts. As shown in Fig. 5, grouping based on EF (EF 40%* vs. *EF 40%) was not related to midterm mortality (PS-adjusted HR 1.151, 95% CI 0.763–1.952, p = 0.281).
Kaplan-Meier curves for overall survival. (A) Kaplan-Meier curves in the unmatched cohorts. (B) Kaplan-Meier curves in the matched cohorts. EF, ejection fraction.
Kaplan-Meier curves for survival free from reoperation. (A) Kaplan-Meier curves in the unmatched cohorts. (B) Kaplan-Meier curves in the matched cohorts. EF, ejection fraction.
PS-adjusted Cox regression analysis in the matched population. PS, propensity score; HR, hazard ratio; CI, confidence interval; EF, ejection fraction.
4. Discussion
Valvular functional insufficiency in IMR is mainly attributed to disadvantageous LV remodeling and annular dilatation following myocardial injury, thereby resulting in poor coaptation of tethering mitral leaflets. Because the degree of LV remodeling can vary, IMR occurs within a broad range of LV injuries. An increasing number of studies have reported that mitral valve repair (ring annuloplasty, leaflet augmentation, subvalvular manipulation, or a combination of these) during surgical revascularization is adequate therapy for patients with moderate IMR [10, 12, 23, 24, 25, 26, 27]. However, few studies have evaluated the effect of depressed LV function on surgical outcomes in this patient group. We cannot be certain whether depressed LV function secondary to LV injury has negative impacts on the surgical outcome of this patient group. Several previous studies have hypothesized that EF may not reflect the true function of the left ventricle under several pathophysiological conditions, which could mask further weakened LV performance in patients with severe MR [28, 29, 30]. However, in the present study, we focused only on patients with moderate IMR, which is unlikely to have a significant effect on the EF. In patients with IMR, a lower EF could mostly be secondary to reduced LV contractility [31]. As per a previous report [8], in the current study we defined depressed LV function as EF 40%. Our goal was to evaluate the in-hospital and midterm outcomes of moderate IMR patients with EF 40% who received mitral valve repair during surgical revascularization, and secondly to evaluate the impacts of depressed LV function on surgical outcomes.
The key findings of our study were that, compared to moderate IMR patients with EF 40%, patients with EF 40% had similar midterm outcomes, a similar incidence of moderate or more MR, a similar proportion of NYHA class III-IV, and similar cumulative survival and cumulative survival free from reoperation. Furthermore, Cox regression analysis showed that EF grouping (EF 40% vs. EF 40%) was not associated with midterm mortality. The present results suggested that depressed LV function prior to surgery was not associated with any significant disadvantage in terms of midterm survival or NYHA functional status. Previously, Ellis et al. [8] found that depressed EF might be associated with increased 3-year mortality in IMR patients who received percutaneous coronary intervention. In contrast to the findings of our study, these authors speculated that depressed LV function could decrease the survival of patients with IMR who received percutaneous coronary intervention. This discrepancy may be due to differences in the study populations. The study by Ellis et al. [8] was on IMR patients who underwent percutaneous coronary intervention, whereas the present study was conducted on moderate IMR patients who received mitral valve repair during surgical revascularization. Using quantitative methods for functional MR grading, Rossi et al. [32] recently found that quantitatively defined functional MR was associated with the prognosis of patients with heart failure. This result concurred with the findings of the present study.
With regard to in-hospital outcomes, the current study found that patients with EF 40% had similar surgical mortality and other major postoperative morbidities to moderate IMR patients with EF 40%, but were more inclined to require prolonged ventilation after surgery. This result was validated using multivariable regression analysis and implied that depressed LVEF could contribute to poor postoperative respiratory function, consistent with the findings of earlier studies [33, 34]. Importantly, our study indicated that there was no association between depressed LV function prior to surgery and surgical mortality, consistent with results from other trials [35, 36, 37, 38]. Within patients with reduced LVEF and moderate to severe IMR, the additional mitral valve repair beyond CABG could also improve survival [39]. This could be due to the introduction over the past few years of advanced surgical techniques, perioperative management with new medicines, and assisted devices [40, 41, 42]. In addition, our study suggested that depressed LV function prior to surgery was not invariably linked to other major postoperative morbidities such as low cardiac output and acute kidney injury requiring hemodialysis. This implied that depressed LV function before surgery was not related to the deterioration of cardiac and renal function.
In general, EF 40% does not appear to be a contraindication for mitral valve repair during revascularization. The benefits of performing mitral interventions beyond CABG have been demonstrated in several studies. A randomized clinical trial of additional mitral valve repair for moderate IMR patients found greater improvements in oxygen consumption, MR severity, and LV remodeling [37]. In another trial, concomitant mitral valve repair resulted in better NYHA functional class, LV dimensions, LV function, and pulmonary artery pressure [38]. In the present study of patients with moderate IMR and depressed LV function, we observed favorable midterm outcomes and no increase in surgical mortality or major adverse cardiac events, although a higher incidence of prolonged ventilation after surgery was observed. These findings supported mitral valve repair during the revascularization of such patients.
Patients in the EF 40% group had larger LV diameters than patients in the EF 40% group, although this difference was reduced in the matched population. LV diameter was also an evaluation criterion for heart function. Enlarged LV suggested cardiac overload and can result from many types of heart disease. With lower EF, IMR patients may also experience more advanced LV diastolic dysfunction and heavier LV preload. Low EF and enlarged LV were both indicators of unfavorable clinical status. However, these patients could also benefit from surgery and still had satisfactory survival.
There were some limitations with the current study. First, the investigation was conducted in a single-center observational setting with a relatively small number of participants and relatively short follow-up, which could therefore affect the generalizability of the findings. Although no significant difference in surgical mortality was found between groups, the sample size may have limited the statistical power. Larger multicenter trials with longer follow-up times were required to further assess long-term outcomes in moderate IMR patients with depressed LV function who receive mitral valve repair during CABG, as well as the impacts of depressed LV function on the surgical outcomes of this patient group. Second, participants in the study were not randomly enrolled, which may have led to some selection bias. PS matching was applied to adjust for differences in baseline characteristics to control potential confounders in the dataset. Although PS matching was used, confounders and selection biases between groups cannot be eliminated. Third, due to the retrospective and observational nature of the study, the dynamic monitoring of changes in left ventricular geometry over time was not feasible. Lastly, the assessments of the patient’s quality of life and major adverse cardiovascular events were not conducted during the follow-up period.
5. Conclusions
Compared to moderate IMR patients with EF 40%, the current study demonstrated that patients with EF 40% had similar midterm outcomes and surgical mortality, but experienced a higher incidence of prolonged ventilation. Depressed LV function may be not associated with surgical or midterm mortality.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Noly PE Pagani FD Obadia JF Bouchard D Bolling SF Ailawadi G et al The role of surgery for secondary mitral regurgitation and heart failure in the era of transcatheter mitral valve therapies Reviews in Cardiovascular Medicine 202223873534525410.31083/j.rcm 2303087 PMC 11178038 · doi ↗ · pubmed ↗
- 2Kumar M Thompson PD Chen K New Perspective on Pathophysiology and Management of Functional Mitral Regurgitation Trends in Cardiovascular Medicine 2022(online ahead of print)10.1016/j.tcm.2022.03.00135259483 · doi ↗ · pubmed ↗
- 3Sannino A Smith RL 2nd Schiattarella GG Trimarco B Esposito G Grayburn PA Survival and Cardiovascular Outcomes of Patients With Secondary Mitral Regurgitation: A Systematic Review and Meta-analysis JAMA Cardiology 20172113011392887729110.1001/jamacardio.2017.2976 PMC 5710448 · doi ↗ · pubmed ↗
- 4Hadjadj S Marsit O Paradis JM Beaudoin J Pathophysiology, Diagnosis, and New Therapeutic Approaches for Ischemic Mitral Regurgitation Canadian Journal of Cardiology 2021379689793334797710.1016/j.cjca.2020.12.011 · doi ↗ · pubmed ↗
- 5Nappi F Avtaar Singh SS Padala M Attias D Nejjari M Mihos CG et al The Choice of Treatment in Ischemic Mitral Regurgitation With Reduced Left Ventricular Function Annals of Thoracic Surgery 2019108190119123144591610.1016/j.athoracsur.2019.06.039PMC 7424599 · doi ↗ · pubmed ↗
- 6Vahanian A Beyersdorf F Praz F Milojevic M Baldus S Bauersachs J et al 2021 ESC/EACTS Guidelines for the management of valvular heart disease European Heart Journal 2022435616323445316510.1093/eurheartj/ehab 395 · doi ↗ · pubmed ↗
- 7Otto CM Nishimura RA Bonow RO Carabello BA Erwin JP 3rd Gentile F et al 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines Circulation 2021143 e 72e 2273333215010.1161/CIR.0000000000000923 · doi ↗ · pubmed ↗
- 8Ellis SG Whitlow PL Raymond RE Schneider JP Impact of mitral regurgitation on long-term survival after percutaneous coronary intervention American Journal of Cardiology 2002893153181180943310.1016/s 0002-9149(01)02231-7 · doi ↗ · pubmed ↗