Esophageal Entrapment in a Thoracic Spine Fracture-Dislocation Injury After a Motor Vehicle Accident
Sarah Danehower, Emily Sieg

TL;DR
This paper describes a rare case of esophageal entrapment caused by a thoracic spine injury after a car accident.
Contribution
The novelty lies in reporting a rare complication of esophageal entrapment in a high thoracic spine injury.
Findings
Esophageal entrapment was identified in a high thoracic distraction injury.
The injury occurred following a motor vehicle accident.
This case highlights the potential for esophageal involvement in such spinal injuries.
Abstract
Thoracic spine fracture-dislocation injuries result from significant forces that cause significant morbidity and mortality. In rare instances, there have been cases of associated esophageal injury from bony laceration. Here we report a case esophageal entrapment in a high thoracic distraction injury following a motor vehicle accident.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
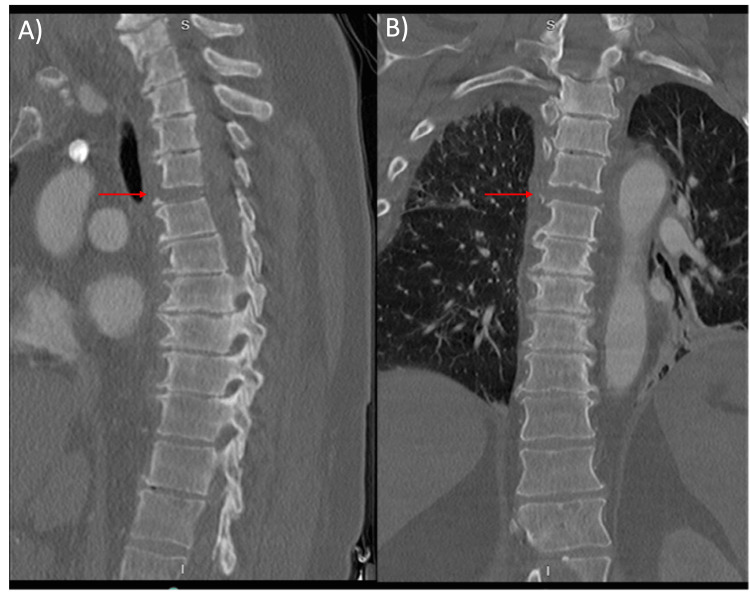 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Trauma Management and Diagnosis · Dysphagia Assessment and Management
Introduction
Thoracic spine fracture-dislocation injuries result from significant forces that disrupt the anterior, middle, and posterior columns of the spine. They are rare and associated with significant neurologic morbidity and mortality. Additionally, these injuries are often associated with concomitant chest injuries. In rare cases, there have been reports of thoracic spine flexion-dislocation injuries with associated vertebral body fractures leading to esophageal perforation due to blunt injury [1-4]. Recovery from esophageal injuries depends on early identification and repair [3]. However, these injuries are difficult to identify due to confounding factors, thereby delaying care. Here we report a case of early identified esophageal entrapment in a high thoracic distraction injury following a motor vehicle accident.
Case presentation
A 61-year-old woman presented to the emergency department (ED) as an unrestrained MVA victim. Upon presentation, she was alert and oriented, able to move all extremities but hypotensive with mean arterial pressures in the 50s. During her initial assessment in the ED, the patient was found to have active extravasation from a significant liver laceration on ultrasonography. The patient was taken emergently to the operating room by general surgery for definitive repair and remained intubated and sedated afterward. Following stabilization, the patient underwent further imaging studies. On computed tomography (CT) scan she was noted to have a thoracic 4/5 distraction injury (Figure 1).
Sagittal (A) and Coronal (B) CT of Thoracic Spine T4/5 fracture-disruption with retrolisthesis of T4 on T5 as indicated with red arrows.
The patient was intubated and sedated on the initial neurological exam but able to move both lower extremities antigravity to noxious stimuli. Magnetic resonance imaging (MRI) of the thoracic spine was obtained, which confirmed a three-column ligamentous injury and disc disruption at T4/5 without spinal cord injury (Figure 2).
T2-weighted sagittal MRIT4/5 disc disruption as well as anterior longitudinal ligamentous and ligamentum flavum disruption without spinal cord injury
MRI T2 short T1 inversion recovery (STIR) sequence further revealed esophageal herniation into disrupted disc space at the level of the injury (Figure 3).
T2-STIR sagittal MRIEsophageal herniation into T4/5 disrupted disc space as indicated by arrow.STIR: short T1 inversion recovery
General surgery performed an esophagogastroduodenoscopy (EGD) to rule out esophageal injury. EGD confirmed retropulsion of the esophagus into the spine at 23cm without perforation or injury. To reduce the esophageal herniation, the general surgery team elected to place an esophageal stent. Following stent placement, posterior thoracic instrumentation of T2 to T7 with pedicle screw fixation and fracture reduction was performed. Pedicle screws for T4 and T5 on the left side were aborted given the patient's small pedicles and inability to safely place screws. Following this procedure, an EGD was again performed which confirmed no esophageal injury after thoracic spine fixation. Postoperatively, the patient recovered from surgery. Given her extensive traumatic injuries and airway edema, the patient was unable to wean from a ventilator. She required a tracheostomy and percutaneous gastrostomy tube, and clinical assessment for esophageal injury was unable to be obtained during hospital admission.
Discussion
Esophageal injury is a rare phenomenon in the trauma setting. Roughly 10% of esophageal injuries are due to penetrating or blunt injury while the remaining 90% are due to iatrogenic causes or perforation by foreign bodies [5-8]. Esophageal injury in the setting of thoracic spine trauma is exceedingly rare but has been reported multiple times in the literature. However, the diagnosis of esophageal injury secondary to blunt injury from thoracic spine trauma is often missed or delayed, resulting in significant patient morbidity. Maroney et al. were the first to report esophageal entrapment after thoracic spine fracture-dislocation [9]. In this case report, the entrapment was only revealed after CT with oral contrast was conducted for persistent dysphagia. Imaging revealed contrast extravasation into the mediastinum. Given the delay in esophageal injury, the patient suffered an infection and ultimately required thoracotomy with diverting esophagostomy, gastrostomy tube placement, and mediastinal drain for contamination.
DeLappe et al. report a case of esophageal entrapment that was discovered after a patient re-presented to the hospital with complaints of dysphagia and nausea after being discharged four days prior [3]. Given the delay in the identification of esophageal injury, the patient suffered an esophageal hematoma and edema necessitating gastrostomy tube placement.
Conclusions
Identification of esophageal injury after thoracic spine trauma remains a difficult and costly problem. Key signs of esophageal injury include pneumomediastinum, subcutaneous emphysema, pneumothorax, or pleural effusion. However as seen in the literature, injuries may be occult on initial CT imaging. Furthermore, given the neurologic morbidity of thoracic fracture dislocations, patients may lack the ability to properly display or communicate signs and symptoms of esophageal injury. Despite the rarity of blunt esophageal injuries from thoracic fracture-dislocations, careful attention should be paid to ruling out esophageal injury prior to any neurosurgical instrumentation given the close proximity of the esophagus to the anterior spinal column. The increasing use of MRI in the setting for fracture-dislocation injuries may allow for earlier identification of these injuries, allowing for earlier EGD with stent placement and prevention of iatrogenic injury.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Esophageal perforation associated with fracture of the upper thoracic spine from blunt trauma: a case report Spinal Cord Ser Cases Inoue T Abe M 150342201610.1038/scsandc.2015.34PMC 512943228053736 · doi ↗ · pubmed ↗
- 2Extension injury of the thoracic spine with rupture of the oesophagus and successful conservative therapy of concomitant mediastinitis Eur Spine J Tjardes T Wafaizadeh A Steinhausen E Krakamp B Bouillon B 24024418 Suppl 220091930104410.1007/s 00586-009-0930-z PMC 2899550 · doi ↗ · pubmed ↗
- 3Esophageal entrapment with blunt thoracic spinal trauma Emerg Radiol Delappe RS Jr Vattoth S Sonavane SK 2432462020132307025610.1007/s 10140-012-1085-5 · doi ↗ · pubmed ↗
- 4Entrapment and obstruction of the esophagus from thoracic spine hyperextension-dislocation injury J Trauma Chiu WC Rodriguez A Greif WM Joseph-Herbert JH Gammaitoni CJ 9599614619991033842310.1097/00005373-199905000-00034 · doi ↗ · pubmed ↗
- 5Thoracic esophageal and tracheal injury following blunt trauma J Trauma Stothert JC Jr Buttorff J Kaminski DL 992995201980700103710.1097/00005373-198011000-00018 · doi ↗ · pubmed ↗
- 6Blunt traumatic rupture of the thoracic oesophagus Thorax Young CP Large SR Edmondson SJ 794795431988306105110.1136/thx.43.10.794PMC 461515 · doi ↗ · pubmed ↗
- 7Esophageal perforation following external blunt trauma J Trauma Beal SL Pottmeyer EW Spisso JM 14251432281988317230010.1097/00005373-198810000-00003 · doi ↗ · pubmed ↗
- 8Rupture of the cervical esophagus and trachea associated with cervical spine fracture J Trauma Reddin A Mirvis SE Diaconis JN 564566271987357311410.1097/00005373-198705000-00018 · doi ↗ · pubmed ↗