Tumor-Induced Osteomalacia: A Case Report
Dayanidhi Meher, Ranjana Giri, Vishal Agarwal, Binod Prusty, Bijay Das

TL;DR
A 55-year-old woman with hip pain and low phosphate levels was diagnosed with tumor-induced osteomalacia, a rare condition caused by a benign tumor, and successfully treated with surgery.
Contribution
This case report highlights the successful diagnosis and treatment of tumor-induced osteomalacia through a systematic workup and surgical intervention.
Findings
The patient had hypophosphatemia and a stress fracture, leading to further evaluation revealing a phosphate-wasting condition.
Elevated fibroblast growth factor levels and a PET-CT scan identified a mesenchymal tumor in the tibia.
Surgical removal of the tumor normalized phosphate levels without additional supplementation.
Abstract
Tumor-induced osteomalacia (TIO) is a rare paraneoplastic syndrome with a variable presentation. We present a case of a 55-year-old female who presented with pain in the bilateral hip region for the last two years. On routine biochemical evaluation, she was found to have hypophosphatemia with an X-ray of the bilateral hip region showing an acute stress fracture in the bilateral intertrochanteric region of the femur. An evaluation for the cause of hypophosphatemia revealed renal phosphate loss with low percentage tubular reabsorption of phosphate (% TRP) of 83% (reference range: 85-95%), with tubular maximum phosphate reabsorption per unit glomerular filtration rate (TmP/GFR) of 2.07 mg/dL (reference range: 2.5-4.5 mg/dL (0.67 mmol/L; range: 0.84-1.23 mmol/L)). Further evaluation revealed elevated levels of intact fibroblast growth factor, 445.7 pg/mL (reference range: 23-95 pg/mL). A…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2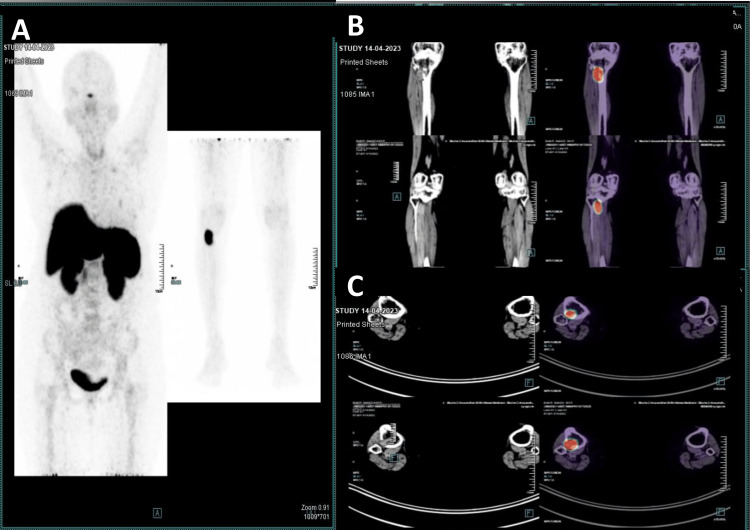 Figure 3
Figure 3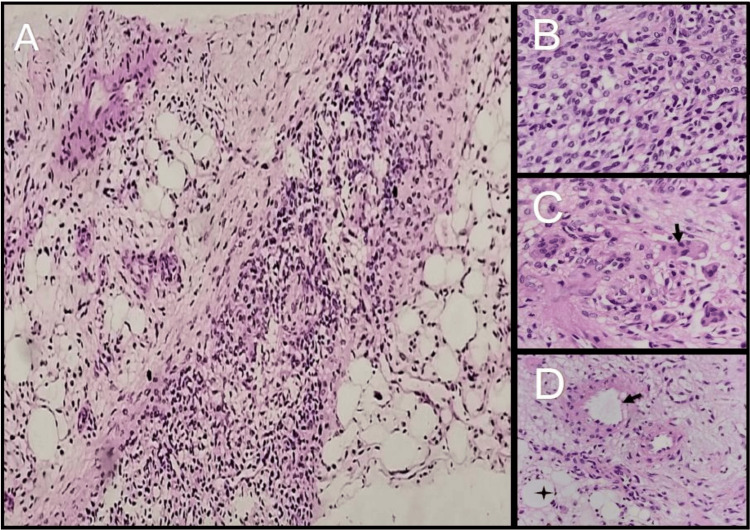 Figure 4
Figure 4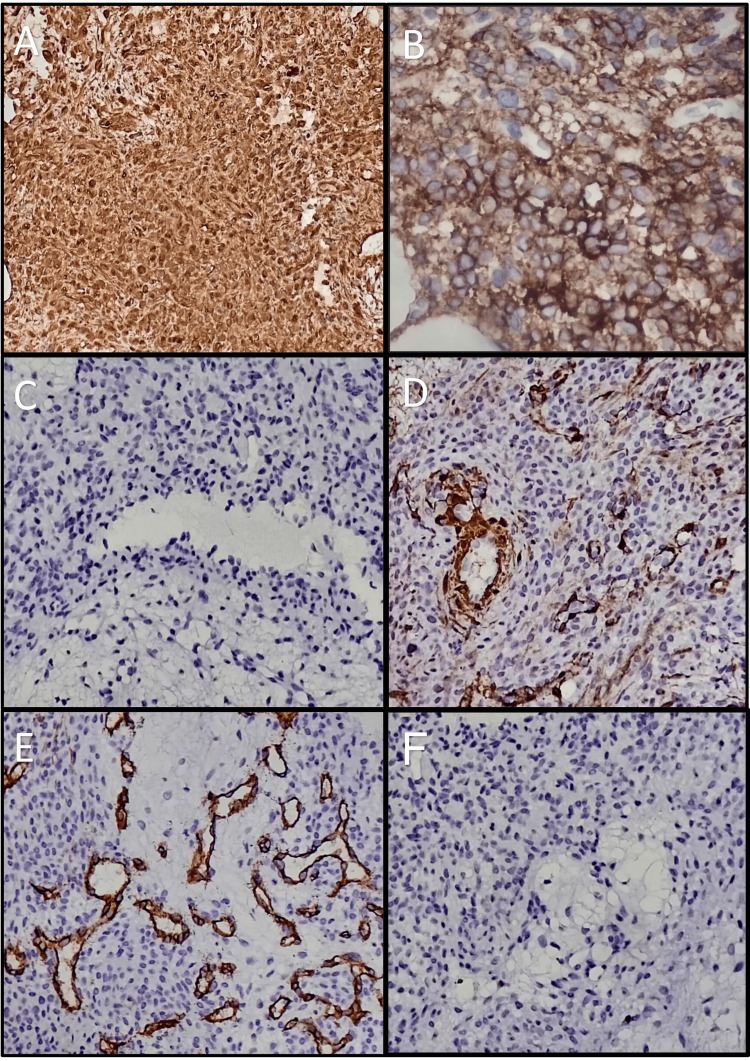 Figure 5
Figure 5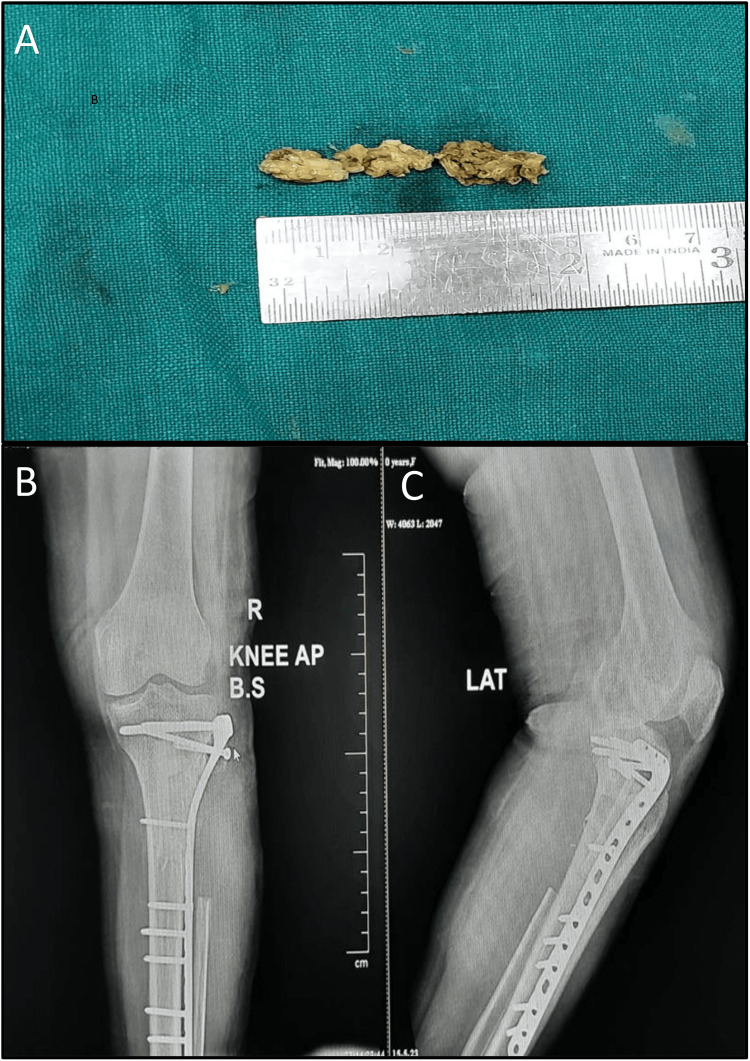 Figure 6
Figure 6| Parameter | Day 1 | Day 2 | Day 10 | Postoperative day 7 | Normal value |
| Hemoglobin | 12.1 gm/dL | - | - | - | 12-15gm/dL |
| WBC | 6,700/µL | - | - | - | 4,000-10,000/µL |
| Free T3 | 3.52 pg/mL (5.4 pmol/L) | - | - | - | 2.8-4 pg/mL (4.3-6.1 pmol/L) |
| Free T4 | 1.17 ng/dL (15 pmol/L) | - | - | - | 0.8-1.8 ng/dL (10.3-23.2 pmol/L) |
| TSH | 4.168 µIU/mL | - | - | - | 0.35-4.2 µIU/mL |
| Serum albumin | 4.4 gm/dL | - | - | 4 gm/dL | 3.9-4.9 gm/dL |
| Serum phosphorus | 1.3 mg/dL (0.41 mmol/L) | 1.4 mg/dL (0.45 mmol/L) | 2.5 mg/dL (0.80 mmol/L) | 4.1 mg/dL (1.32 mmol/L) | 2.5-4.5 mg/dL (0.8-1.45 mmol/L) |
| Serum calcium | 9.2 mg/dL (2.29 mmol/L) | - | - | 8.9 mg/dL (2.22 mmol/L) | 8.6-10.3 mg/dL (2.15-2.57 mmol/L) |
| Serum magnesium | 2.1 mg/dL (0.86 mmol/K) | - | - | - | 1.6-2.6 mg/dL (0.65-1.06 mmol/L) |
| 25-hydroxy vitamin D | 39 ng/mL (97.3 nmol/L) | - | - | - | 20-65 ng/mL (50-162 nmol/L) |
| 1,25-dihydroxy vitamin D | - | - | 18 pg/mL (43.2 pmol/L) | - | 19.9-79.3 pg/mL (47.8-190.3 pmol/L) |
| Parathyroid hormone(intact) | 43.4 pg/mL | - | - | - | 15-65 pg/mL |
| Serum creatinine | - | - | 0.78 mg/dL (68.9 µmol/L) | - | 0.5-1.1 mg/dL (44-97 µmol/L) |
| Urine creatinine | - | - | 68.92 mg/dL 6,092.6 µmol/L | - | 20-275 mg/dL (1,768-24,310 µmol/L) |
| Urine phosphorus | - | - | 38.9 mg/gm | - | 105-1,081 mg/gm |
| FePO4 | - | - | 17% | - | <15% |
| %TRP | - | - | 83% | - | 85-95% |
| TmP/GFR | - | - | 2.07 mg/dL (0.67 mmol/L) | - | 2.6-3.8 mg/dL (0.84-1.23 mmol/L) |
| FGF-23 | - | - | 445.7 pg/mL | - | 23-95 pg/mL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParathyroid Disorders and Treatments · Heterotopic Ossification and Related Conditions · Bone health and treatments
Introduction
Phosphaturic mesenchymal tumors leading to tumor-induced osteomalacia (TIO) are rare entities in clinical practice [1]. Renal phosphate loss because of elevated fibroblast growth factor-23 (FGF-23) levels is the biochemical hallmark of the disease, which leads to a clinical spectrum comprising nonspecific features such as vague musculoskeletal symptoms such as pain and aches at the pelvic girdle, gait instability, and multiple fractures [2]. These tumors are typically benign and can be found anywhere in the body. It is a rare disease entity with approximately only 1,000 cases reported until today [1]. This might represent a gross underestimation of the actual prevalence of the disease as the signs and symptoms of the disease are usually nonspecific, which may lead to a misdiagnosis by the treating physician [3,4]. Thus, here we describe a case of TIO, who presented with similar nonspecific complaints, and the systemic way we approached the diagnosis of such a case.
Case presentation
A 55-year-old Asian woman presented to our orthopedic unit with chief complaints of pain in the bilateral hip region for the last two years, along with the inability to walk for the last six months. The patient was initially able to walk without support, but, gradually, she was confined to a wheelchair for the past three months. She had a known case of primary hypothyroidism and hypertension for the past three years and was on telmisartan 40 mg once daily and levothyroxine supplementation 25 mcg once daily. There was no history of trauma and weight loss, and the patient attained menopause at the age of 50 years. A physical examination revealed tenderness on the internal rotation of bilateral hip joints. There was no evidence of any bony or soft tissue swelling. The systemic examination was unremarkable. On routine biochemical evaluation, she was found to have hypophosphatemia with a serum phosphorus level of 1.4 mg/dL (reference range: 2.5-4.5 mg/dL (0.45 mmol/L; range: 0.8-1.45 mmol/L)), with X-ray of the bilateral hip region showing acute stress fracture in the bilateral intertrochanteric region of the femur (Figure 1). A dual-energy X-ray absorptiometry (DEXA) scan of the anteroposterior spine revealed a T-score of -3.5. The patient was referred to the endocrinology unit given the evaluation of hypophosphatemia and osteoporosis.
An X-ray of the bilateral hip region showing acute stress fracture (arrows) in the bilateral intertrochanteric region of the femur.
Evaluation for the cause of hypophosphatemia revealed a renal phosphate loss with a low percentage tubular reabsorption of phosphate (%TRP) of 83% (reference range: 85-95%), with tubular maximum phosphate reabsorption per unit glomerular filtration rate (TmP/GFR) of 2.07 mg/dL (reference range: 2.5-4.5 mg/dL (0.67 mmol/L; range: 0.84-1.23 mmol/L)). A further evaluation for the cause of renal phosphate wasting revealed elevated levels of intact fibroblast growth factor-23 (445.7 pg/mL (reference range: 23-95 pg/mL)). The serum 1,25-dihydroxy vitamin D (calcitriol) level was 43.2 picomoles per liter (pmol/L) (reference range: 47.8-190.3 pmol/L (18 pg/mL; range: 19.9-79.3 pg/mL)). Her biochemical investigations are summarized in Table 1.
An X-ray of the right knee revealed an osteolytic lesion on the posterolateral aspect of the metaphyseal region of the right tibia (Figure 2). Gallium-68 DOTA-1-Nal3-octreotide (DOTANOC) PET-CT revealed a focal increased tracer uptake with lytic lesion along with a soft tissue component of lateral metaphyseal aspect of proximal right tibia (2.1 cm x 2.4 cm x 2.9 cm, standard uptake value maximum of 23.1), suspicious of somatostatin receptor avid mesenchymal tumor (Figure 3).
An X-ray of bilateral knee joints showing osteolytic lesion (arrow) in the posterolateral aspect of the right tibia: panel A (anteroposterior view) and panel B (lateral view).
A 68-Gallium DOTANOC PET-CT scan (panel A) showing a focal increased tracer uptake in the metaphyseal aspect of the proximal right tibia (approximate size: 2.1 cm x 2.4 cm x 2.9 cm, standardized uptake values (SUV) max: 23.1).No pathological focal tracer uptake or lytic/sclerotic lesion was noted in the rest of the visualized skeleton. Panels B and C are transverse and coronal views, respectively.
A CT-guided biopsy of the lesion was done, which showed a phospaturic mesenchymal tumor (Figure 4). On immunohistochemistry (Figure 5), it was positive for vimentin and negative for S-100, smooth muscle antibody (SMA), and CD34. A diagnosis of TIO was made, and the patient was planned for operative management. Preoperatively, the patient was managed with oral phosphate supplementation of 40 mg/kg/day in four divided doses, along with oral calcitriol supplementation at a dose of 0.5 μg/day.
Histological images of the CT-guided linear core biopsy.Panel A showing tumor cells arranged in sheets admixed with adipocytes and blood vessels (100x). Panel B showing bland-looking spindle cells with inconspicuous nucleoli with no nuclear atypia, mitosis, or necrosis (400x). Panel C showing multinucleated giant cells (arrow) (400x) and panel D showing blood vessels (arrow) and adipose tissue (star) (400x). Panels A through D, hematoxylin-eosin staining.
Immunostaining.Panel A and Panel B stain immune-positive for vimentin and CD56, respectively. Panels C, D, E, and F show tumor is immune-negative for S-100, smooth muscle antibody (SMA), CD34, and desmin, respectively.
Definitive treatment with excision of the tumor (Figure 6) with partial fibulectomy with stabilization with lateral tibial locking compression plate and tricortical iliac crest bone grafting under spinal and epidural anesthesia was done.
Panel A showing gross tumor specimen, post-excision. Panels B and C showing postoperative X-ray with excision of tumor mass with partial fibulectomy, with stabilization with lateral tibial locking compression plate and tricortical iliac crest bone grafting.
Postoperatively, her phosphorus level was within the normal target range, even without oral phosphate supplementation. At three months and six months after surgery, the patient was reviewed, and the patient was able to walk without support.
Discussion
TIO is a rare clinical diagnosis often associated with diagnostic delay owing to its nonspecific symptoms. As per the literature, the overall misdiagnosis rate has been reported up to 95%. This report describes a case of TIO in a 55-year-old woman, caused by a phosphaturic mesenchymal tumor in a 55-year-old woman. As per the literature, the usual age of presentation is between 40 and 45 years [3]. In adults, the most common symptom at presentation is usually bone pain, arising at the site of the localized tumor, or because of pathological fractures (80% of patients). Because of delays in diagnosis, the patient’s bone health usually worsens, and the patient usually gets confined to a wheelchair [5]. Symptoms are usually present for several months to years, and the average delay in diagnosis from the onset of symptoms is usually 2.9 ± 2.3 years. As seen in our case, the patient was symptomatic for the past two years and was undiagnosed because of nonspecific symptoms of low back ache and gait instability because of proximal myopathy and stress fractures at the bilateral femoral neck and intertrochanteric region.
The typical biochemical pattern of TIO results from increased fibroblast growth factor 23 (FGF-23), which leads to an increase in renal phosphate leak, subsequently leading to low serum phosphate levels [6]. Serum calcium, 25-hydroxyvitamin D, and parathyroid hormone levels are typically normal, with low or inappropriately normal 1,25-dihydroxy vitamin D levels, owing to the inhibition of 1-alpha hydroxylase vitamin D3 enzyme by FGF-23.
Once the diagnosis is suspected, the presence of hypophosphatemia needs to be established as the first initial step of evaluation [7]. Morning fasting blood specimen for serum phosphate is always preferred as food intake increases serum phosphate levels. Age-specific cutoffs should be taken in the case of children. Once the presence of hypophosphatemia is biochemically documented, the next step in evaluation is to look for the cause of hypophosphatemia. History of intake of antacids may point towards decreased absorption of phosphate. Phosphate loss via kidneys comprises the major cause of hypophosphatemia and is confirmed by the presence of low %TRP and low TmP/GFR [7]. In our case, there was persistent hypophosphatemia along with normal values of serum calcium, serum magnesium, serum 25-hydroxy vitamin D, and parathyroid hormone levels, along with evidence of renal phosphate loss demonstrated by low %TRP of 83% and low TmP/GFR of 2.07 mg/dL. This leads us to look for the cause of renal phosphate leak by measuring serum intact fibroblast growth factor 23 (iFGF23), a phosphaturic hormone that causes renal phosphate loss and has been implicated in having a pathogenic role in TIO [8]. Elevated levels of iFGF23 lead us to the next step of tumor localization. Tumors causing TIO can be present anywhere in the body from head to toe and are usually small and slow-growing [9].
As the physical examination was unremarkable in our case with no history of any bony or soft tissue swelling, we went for functional imaging with whole-body gallium-68 DOTANOC PET-CT to localize the tumor. As per the literature, the lower extremities (59.6%) are the most common site for tumor localization in patients with TIO. In 24% of cases, it is localized in the head and neck region, while the upper extremities and torso comprise 9.4% and 6.9% of cases, respectively [10]. In our case, it was localized to the lower extremity, involving the upper end of the right tibia. The patient later underwent anatomical imaging with contrast-enhanced magnetic resonance imaging (CEMRI) to delineate the local extension of the tumor and to plan for surgical resection.
The definitive management of TIO comprises the complete surgical resection of the tumor mass [1]. Our patient was subjected to surgical resection of the tumor and the postoperative recovery was remarkable as previously discussed.
The differential diagnosis of TIO includes other causes of hypophosphatemia, such as malabsorption syndrome, and nutritional phosphate deficiency, the possibility of which is suspected from the patient’s past medical history and dietary history. The young age of presentation, along with growth retardation and ear or dental abnormalities in the patient or their family members may hint toward genetic causes of osteomalacia associated with elevated FGF-23 and hypophosphatemia. This includes autosomal dominant, autosomal recessive, and X-linked forms of hypophosphatemic rickets. Disorders such as Fanconi syndrome and hereditary hypophosphatemic rickets with hypercalciuria constitute the differential diagnosis when renal phosphate leak is accompanied by low FGF-23 [11].
Conclusions
TIO can have varied presentations. Owing to its multifaceted presentation, it warrants a multidisciplinary approach to identify and localize the tumor. A complete resection of the tumor mass leads to a cure in such cases. This case highlights the need for proper and systematic evaluation of a case of hypophosphatemia, leading to the diagnosis of TIO.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tumor-induced osteomalacia Calcif Tissue Int Florenzano P Hartley IR Jimenez M Roszko K Gafni RI Collins MT 12814210820213250413810.1007/s 00223-020-00691-6 · doi ↗ · pubmed ↗
- 2Phosphaturic mesenchymal tumors: a review and update Semin Diagn Pathol Folpe AL 2602683620193130187610.1053/j.semdp.2019.07.002 · doi ↗ · pubmed ↗
- 3The diagnostic dilemma of tumor induced osteomalacia: a retrospective analysis of 144 cases Endocr J Feng J Jiang Y Wang O 6756836420172845068410.1507/endocrj.EJ 16-0587 · doi ↗ · pubmed ↗
- 4Tumor-induced osteomalacia JAMA Jan de Beur SM 1260126729420051616013510.1001/jama.294.10.1260 · doi ↗ · pubmed ↗
- 5A 9-month-old phosphaturic mesenchymal tumor mimicking the intractable rickets J Pediatr Orthop B Jung GH Kim JD Cho Y Chung SH Lee JH Sohn KR 1271321920101980195310.1097/BPB.0b 013e 32832 f 59cb · doi ↗ · pubmed ↗
- 6Tumor-induced osteomalacia: experience from three tertiary care centers in India Endocr Connect Pal R Bhadada SK Singhare A 266276820193072677110.1530/EC-18-0552 PMC 6410764 · doi ↗ · pubmed ↗
- 7Nomogram for derivation of renal threshold phosphate concentration Lancet Walton RJ Bijvoet OL 309310306197510.1016/s 0140-6736(75)92736-150513 · doi ↗ · pubmed ↗
- 8The foot that broke both hips: a case report and literature review of tumor-induced osteomalacia Case Rep Rheumatol Beygi S Denio A Sharma TS 2017201710.1155/2017/3191673 PMC 561874829104808 · doi ↗ · pubmed ↗