Influence of the Single Coronary Vessel on Acute Outcomes of In-Stent CTO Recanalization
Jan-Erik Guelker, Christian Blockhaus, Edward Kemala, Klaus Ingerfurth, Julian Kuervers, Alexander Bufe

TL;DR
This study examines how the location of a coronary vessel affects outcomes when reopening blocked coronary stents.
Contribution
The study shows that vessel location does not impact success or complication rates in in-stent CTO recanalization.
Findings
Technical success was independent of the involved coronary vessel.
No significant difference in safety endpoints was found between the LAD, LCX, and RCA groups.
Retrograde techniques were more common in RCA cases but did not affect outcomes.
Abstract
Recanalization of in-stent chronic total occlusion (IS-CTO) is challenging and has resulted in inconsistent results. The aim of our study was to analyze the influence of the individual coronary vessels on the acute outcomes following IS-CTO PCI. This was an observational retrospective study, including 66 patients undergoing recanalization of a CTO. The CTO interventions were performed bi-femoral using 7-French guiding catheters. A composite endpoint summarizing severe complications was evaluated, including emergency coronary artery bypass grafting surgery (CABG) and cardiac death. We subdivided our cohort into three groups (LAD group, LCX group, RCA group). The retrograde technique and the utilization of an extension catheter were used more frequently in patients with a RCA IS-CTO. There was no significant difference between the composite safety endpoints amongst the three…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
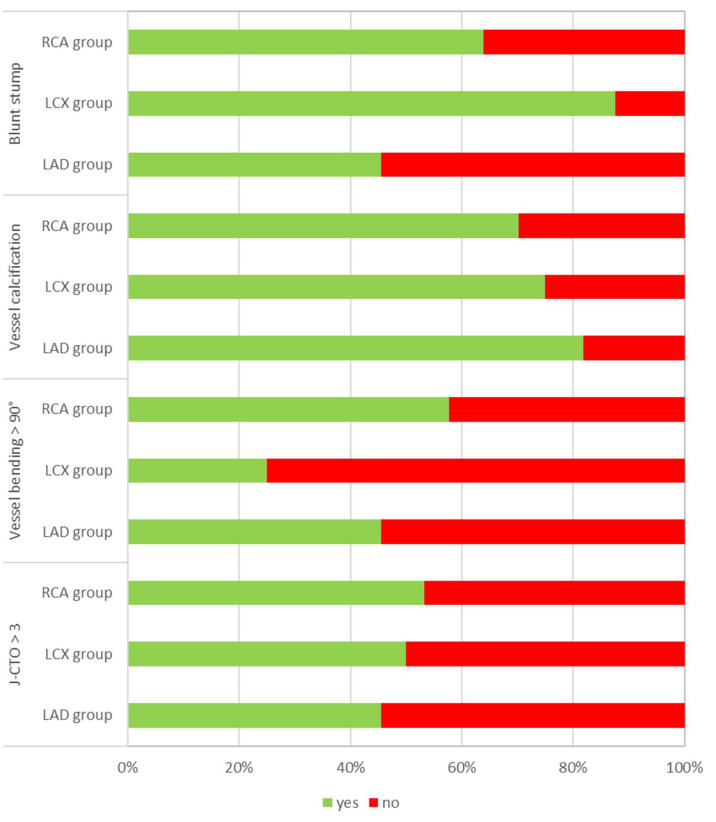 Fig. 1
Fig. 1| LAD | LCX | RCA | ||
| (n = 11) | (n = 8) | (n = 47) | ||
| Age | 2 (18.2%) | 3 (37.5%) | 18 (38.3%) | 0.503 |
| Male sex | 10 (90.9%) | 7 (87.5%) | 41 (87.2%) | 1.000 |
| Diabetes | 5 (45.5%) | 2 (25.0%) | 8 (17.0%) | 0.147 |
| COPD | 0 (0.0%) | 1 (12.5%) | 2 (4.3%) | 0.386 |
| Smoking | 3 (27.3%) | 5 (62.5%) | 21 (44.7%) | 0.304 |
| PAD | 1 (9.1%) | 1 (12.5%) | 8 (17.0%) | 1.000 |
| Hypertension | 10 (90.9%) | 5 (62.5%) | 32 (68.1%) | 0.292 |
| Family history for CAD | 1 (9.1%) | 1 (12.5%) | 13 (27.7%) | 0.375 |
| Prior MI | 7 (63.6%) | 2 (25.0%) | 16 (34.0%) | 0.142 |
| Prior CABG | 2 (18.2%) | 3 (37.5%) | 5 (10.6%) | 0.115 |
| Prior CTO PCI attempt | 4 (36.4%) | 6 (75.0%) | 34 (72.3%) | 0.079 |
| Prior PCI | 9 (81.8%) | 6 (75.0%) | 32 (68.1%) | 0.759 |
| EF | 11 (100.0%) | 8 (100.0%) | 46 (97.9%) | 1.000 |
| Cholesterol | 0 (0.0%) | 2 (28.6%) | 9 (24.3%) | 0.538 |
| HDL Cholesterol | 5 (71.4%) | 8 (100.0%) | 25 (67.6%) | 0.306 |
| LDL Cholesterol | 3 (42.9%) | 4 (57.1%) | 16 (43.2%) | 0.901 |
| LAD | LCX | RCA | |||
| (n = 11) | (n = 8) | (n = 47) | |||
| Coronary artery disease | 0.392 | ||||
| 1 vessel | 2 (18.2%) | 2 (25.0%) | 9 (19.1%) | ||
| 2 vessel | 4 (36.4%) | 3 (37.5%) | 24 (51.1%) | ||
| 3 vessel | 5 (45.5%) | 3 (37.5%) | 14 (29.8%) | ||
| Blunt Stump | 5 (45.5%) | 7 (87.5%) | 30 (63.8%) | 0.180 | |
| Calcification | 9 (81.8%) | 6 (75.0%) | 33 (70.2%) | 0.905 | |
| Bending | 5 (45.5%) | 2 (25.0%) | 30 (63.8%) | 0.089 | |
| J-CTO Score | 5 (45.5%) | 4 (50.0%) | 25 (53.2%) | 0.926 | |
| Retrograde technique | 2 (18.2%) | 0 (0.0%) | 16 (34.0%) | 0.101 | |
| Use of an extension catheter | 1 (9.1%) | 0 (0.0%) | 29 (61.7%) | 0.041 | |
| Use of IVUS | 9 (81.8%) | 6 (75.0%) | 35 (74.5%) | 0.926 | |
| Length of lesion** | 40 mm (10–60) | 25 mm (15–70) | 40 mm (15–80) | 0.182 | |
| Fluoroscopy time** | 43 min (12–48) | 31 min (12–65) | 42 min (11–97) | 0.407 | |
| Examination time** | 110 min (50–150) | 85 min (45–115) | 120 min (35–240) | 0.141 | |
| Amount of contrast medium** | 300 mL (100–500) | 210 mL (100–450) | 250 mL (120–630) | 0.555 | |
| Number of stents** | 3 (1–5) | 2 (1–3) | 2 (1–4) | 0.364 | |
| Diameter of stents** | 3.0 mm (2.5–3.5) | 3.0 mm (2.75–3.5) | 3.5 mm (2.5–4.0) | 0.037 | |
| Length of stent** | 66 mm (30–120) | 46 mm (23–69) | 66 mm (18–132) | 0.212 | |
| Complication rate | 0 (0.0%) | 1 (12.5%) | 1 (2.1%) | 0.255 | |
| Technical success rate | 11 (100.0%) | 7 (87.5%) | 40 (85.1%) | 0.495 | |
| LAD | LCX | RCA | ||
| (n = 11) | (n = 8) | (n = 47) | ||
| In-hospital death | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 1.000 |
| Hamatoma | 0 (0.0%) | 1 (12.5%) | 1 (2.1%) | 0.255 |
| Stroke | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 1.000 |
| Perforation | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 1.000 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCoronary Interventions and Diagnostics · Peripheral Artery Disease Management · Cardiac Valve Diseases and Treatments
1. Introduction
In interventional cardiology recanalization of chronic total occlusion (CTO) remains a complex procedure. A CTO of a coronary artery can be identified in up to 18% of patients undergoing coronary angiography [1]. Due to novel recanalization strategies and emerging devices, percutaneous coronary intervention (PCI) has become a promising treatment option [2, 3, 4, 5, 6, 7]. CTO revascularization has been shown to be a predictor for the prevention of cardiac death [8].
Particularly PCI of in-stent occlusions (IS-CTO) is extremely demanding, and studies have shown inconsistent results regarding outcomes and complications [9, 10, 11, 12, 13, 14, 15]. There is little data in the literature on outcomes amongst the three individual major coronary artery branches. IS-CTO is defined as a 50% stenosis of a previously stented segment.
In this study we want to analyze the influence of the individual coronary vessels on the acute outcomes following IS-CTO PCI.
2. Methods
Our study is an observational study. 66 patients who underwent IS-CTO PCI between 2012 and 2021 were retrospectively included. The indication for CTO-PCI was based on the presence of clinically symptoms including typical angina pectoris or dyspnea [16, 17, 18].
The complex interventions were performed bi-femoral using 7-French guiding catheters. After initial contralateral contrast injections, the length of the CTO lesion and the existence and extent of collateral vessels was carefully analyzed. Antegrade and retrograde recanalization techniques were used. Heparin was administered during CTO-PCI guided by measurements of the activated clotting time ( 300 sec).
After a successful recanalization a dual antiplatelet therapy consisting of aspirin and clopidogrel for at least 6 months was instituted. The primary endpoint was technical success, defined as a successful recanalization of the CTO with a residual stenosis less than 30% and restoration of thrombolysis in myocardial infarction (TIMI)-flow grade 3.
A composite endpoint was evaluated including acute cardiac death, vascular and bleeding complications, coronary perforation, which necessitated treatment by pericardial puncture, peri-interventional myocardial infarction (MI) which was defined as an increase in cardiac troponin blood levels in a patient who also exhibits signs or symptoms of MI, stroke and emergency coronary artery bypass grafting surgery (CABG) [19, 20].
3. Statistical Analysis
The distribution of continuous variables was characterized by mean
standard deviation, or median with interquartile ranges (25th to 75th
percentiles), as well as ranges (minimum to maximum), and the distribution of
categorical variables by absolute and relative frequencies. The Shapiro-Wilk test
was used to test for normality of the data. The Kruskal-Wallis test was used
without testing normality because of the small sample size. Fisher’s exact test
was used to test the differences in the distributions of categorical variables.
According to the exploratory character of the analysis all p values were
interpreted as descriptive measures rather than as definitive inferential
measures. A p value of less than 0.05 was considered statistically
significant, *p * 0.10 was considered as a statistical trend.
4. Results
66 patients were included and subdivided into three groups (LAD group, LCX group, RCA group). 47 (72.2%) patients suffered from a RCA IS-CTO, 11 (16.7%) from a LAD IS-CTO and 8 (12.1%) from a LCX IS-CTO.
Table 1 shows the baseline clinical characteristics. The majority of the patients were male (87.9%) and 34.8% were older than 65 years of age. Patients in the LAD group had a higher incidence of diabetes mellitus (LAD group: 45.5%, LCX group: 25.0%, RCA group: 17.0%, p value: 0.147). Other cardiovascular risk factors such as smoking habits, increased cholesterol values, and a family history of coronary artery disease (CAD), were distributed equally amongst the groups. Hypertension was present in 90.9% of the LAD group, 62.5% in the LCX group and 68.1% in the RCA group (p value: 0.292). Patients in the LCX group had a higher incidence of prior coronary artery bypass graft (CABG) surgery (LAD group: 18.2%, LCX group: 37.5%, RCA group: 10.6%, p value: 0.115). Fewer patients in the LAD group had a prior CTO PCI attempt (LAD group: 36.4%, LCX group: 75.0%, RCA group: 72.3%, p value: 0.079). Almost all patients in each group had an ejection fraction (EF) greater than 40% (LAD group: 100%, LCX group: 100%, RCA group: 97.9%, p value: 1).
Table 2 summarizes the angiographic parameters and peri-procedural characteristics.
The J-CTO score, including the degree of calcification of the occlusion, bending over 90° in the occluded segment, a blunt stump morphology, the length of the occluded segment longer than 20 mm and a previously failed recanalization attempt, was comparable in all groups; however, the bending of the vessel was more frequent in the RCA group (Fig. 1). The retrograde technique was used more frequently in patients with a RCA IS-CTO (LAD group: 18.2%, LCX group: 0.0%, RCA group: 34.0%, p value: 0.10). The use of a GuideLiner (Vascular Solutions Inc., Minneapolis, MN, USA) was used more frequently in the RCA group and the diameter of the implanted stents were larger in these patients (LAD group: 3.0 mm, LCX: 3.0 mm, RCA: 3.5 mm, p value: 0.037).
Distribution of the J-CTO, blunt stump morphology, vessel calcification and vessel bending.
The number of stents (LAD group: 3, LCX group: 2, RCA group: 2, p value: 0.364) and the length of stents (LAD group: 66 mm, LCX group: 46 mm, RCA group: 66 mm, p value: 0.212) were similar amongst the groups.
Technical success was independent of the involved vessel (LAD group: 100%, LCX group: 87.5%, RCA: 85.1%).
Acute procedural complications derived from the composite endpoint were rare and showed no significant difference between the groups (LAD group: 0.0%, LCX group: 12.5%, RCA group: 2.1%, p value: 0.255). They included mostly vascular complications such as a local hematoma at the puncture site and could be treated without further consequences. No severe complications such as peri-procedural death, stroke or MI occurred (Table 3).
5. Discussion
Several studies have reported the challenges involved in IS-CTO recanalization. A large registry could demonstrate the incidence of a IS-CTO PCI was 11% [21]. Mir et al. [10] emphasized that PCI for IS-CTO was associated with higher odds of MACE and MI compared to PCI for de-novo CTO. Data by Guan et al. [22] stressed that effectiveness and safety of this complex procedure are reasonable, but the risk of cardiac death and MI is higher among patients with IS-CTO. In another study including 81 patients, Gao et al. [23] added that patients with IS-CTO had worse Seattle Angina Questionnaire scores concerning anginal stabilities than the patients with de novo CTO.
Karmpaliotis et al. [24] provided some reasons for the difficulties to recanalize IS-CTO which may explain the on-going challenges involved with this complex procedure. It was particularly emphasized that the previous use of under-expanded stents is one key problem. This leads to the problem that the wire may enter the subintimal space. Furthermore, a possible stent fracture may complicate the wiring even with stiff wires. This is even more complex in tortuous vessels which are often associated with hard fibrous tissue and high calcium content [24]. In contrast to data from Azzalini et al. [13], we experienced many In-Stent CTO in the RCA.
This present study emphasizes three important findings:
First, the retrograde technique was used more frequently in patients with a RCA IS-CTO. We know that the retrograde approach, when used by experienced operators who have been well trained, can produce higher retrograde success in complex CTO lesions [25]. Surmely et al. [26] proposed that septal collaterals of the LAD can be used as an optimal access for the retrograde approach in RCA-CTO revascularization.
Second, the bending of the vessel was more frequent in the RCA group. That is consistent with the fact that the use of an extension catheter, such as the GuideLiner, was more frequently required. Several studies have proposed that a mother-and-child catheter is a simple, safe and efficacious adjunctive device for complex CTO recanalization when despite standard measures, it is not possible to deliver an initial balloon or microcatheter across the occluded segment [27, 28, 29, 30]. It helps to avoid implantation of under-expanded stents which contributes to in-stent occlusion. Furthermore, information about the amount of neointimal or peri-stent calcium, and multiple old stent strut layers are important determinants of new stent under expansion which is associated with adverse long-term outcomes [31].
Third, we demonstrated that the technical success and complication rate in IS-CTO PCI is independent of the target vessel. To the best of our knowledge, this is the first study to document that there is no influence of the target vessel on the success of this complex and challenging intervention.
6. Study Limitations
Our study has some limitations. First, the study is an observational retrospective analysis and all the data was collected from one single center. Second, our study only reported in-hospital outcomes without a follow-up. Third, no data was available on the type of stent used in this cohort. Fourth, there was no clinical event adjudication by a clinical events committee. Fifth, all procedures were performed at one experienced PCI center, thus limiting the generalizability of our findings to centers with limited experience. Sixth, our cohort included only 66 patients.
7. Conclusions
Recanalization of in-stent CTO lesions is a challenging procedure in interventional cardiology. Success and complication rates are independent of the occluded vessel. Recanalization is safe and feasible when performed safely in experienced hands.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Azzalini L Jolicoeur EM Pighi M Millán X Picard F Tadros V et al Epidemiology, Management Strategies, and Outcomes of Patients with Chronic Total Coronary Occlusion The American Journal of Cardiology 2016118112811352756119010.1016/j.amjcard.2016.07.023 · doi ↗ · pubmed ↗
- 2Fefer P Knudtson ML Cheema AN Galbraith PD Osherov AB Yalonetsky S et al Current Perspectives on Coronary Chronic Total Occlusions. The Canadian Multicenter Chronic Total Occlusions Registry Journal of the American College of Cardiology 2012599919972240207010.1016/j.jacc.2011.12.007 · doi ↗ · pubmed ↗
- 3Tomasello SD Boukhris M Giubilato S MarzàF Garbo R Contegiacomo G et al Management strategies in patients affected by chronic total occlusions: results from the Italian Registry of Chronic Total Occlusions European Heart Journal 201536318931982633336710.1093/eurheartj/ehv 450 · doi ↗ · pubmed ↗
- 4Bufe A Haltern G Dinh W Wolfertz J Schleiting H Guelker H Recanalisation of coronary chronic total occlusions with new techniques including the retrograde approach via collaterals Netherlands Heart Journal 2011191621672202099610.1007/s 12471-011-0091-7PMC 3077875 · doi ↗ · pubmed ↗
- 5Galassi AR Tomasello SD Reifart N Werner GS Sianos G Bonnier H et al In-hospital outcomes of percutaneous coronary intervention in patients with chronic total occlusion: insights from the ERCTO (European Registry of Chronic Total Occlusion) registry Euro Intervention 201174724772176466610.4244/EIJV 7I 4A 77 · doi ↗ · pubmed ↗
- 6Christopoulos G Menon RV Karmpaliotis D Alaswad K Lombardi W Grantham A et al The efficacy and safety of the “hybrid” approach to coronary chronic total occlusions: insights from a contemporary multicenter US registry and comparison with prior studies The Journal of Invasive Cardiology 20142642743225198485 PMC 4747420 · pubmed ↗
- 7Galassi AR Sianos G Werner GS Escaned J Tomasello SD Boukhris M et al Retrograde recanalization of chronic total occlusions in Europe: procedural, in-hospital, and long-term outcomes from the multicenter ERCTO registry Journal of the American College of Cardiology 201565238824002604673210.1016/j.jacc.2015.03.566 · doi ↗ · pubmed ↗
- 8Gong X Zhou L Ding X Chen H Li H The impact of successful chronic total occlusion percutaneous coronary intervention on long-term clinical outcomes in real world BMC Cardiovascular Disorders 2021211823385834910.1186/s 12872-021-01976-w PMC 8048230 · doi ↗ · pubmed ↗