Usefulness of Vena Contracta for Identifying Severe Secondary Mitral Regurgitation: A Three-Dimensional Transesophageal Echocardiography Study
Hirokazu Onishi, Masaki Izumo, Toru Naganuma, Yoshihiro J. Akashi, Sunao Nakamura

TL;DR
This study shows that vena contracta measurements are more accurate than traditional methods for identifying severe secondary mitral regurgitation using 3D transesophageal echocardiography.
Contribution
The study introduces vena contracta-based parameters as a novel and more accurate method for assessing severe secondary mitral regurgitation.
Findings
VCWAverage and VCAEllipse showed stronger correlations with VCA than EROAPISA.
Over 40% of patients with moderate or less SMR by EROAPISA had severe SMR based on VCA.
VCWAverage and VCAEllipse improved reclassification of SMR severity in patients with EROAPISA <0.30 cm².
Abstract
In secondary mitral regurgitation (SMR), effective regurgitant orifice area by the proximal isovelocity surface area method (EROAPISA) evaluation might cause an underestimation of regurgitant orifice area because of its ellipticity compared with vena contracta area (VCA). We aimed to reassess the SMR severity using VCA-related parameters and EROAPISA. The three-dimensional transesophageal echocardiography data of 128 patients with SMR were retrospectively analyzed; the following parameters were evaluated: EROAPISA, anteroposterior and mediolateral vena contracta widths (VCWs) of VCA (i.e., VCWAP and VCWML), VCWAverage calculated as (VCWAP + VCWML)/2, and VCAEllipse calculated as π × (VCWAP/2) × (VCWML/2). Severe SMR was defined as ≥0.39 cm2. The mean age of the patients was 77.0 ± 8.9 years, and 78 (60.9%) were males. Compared with EROAPISA (r = 0.801), VCWAverage (r =…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
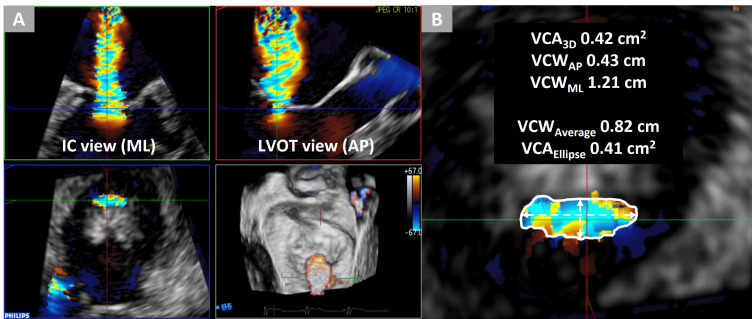 Fig. 1
Fig. 1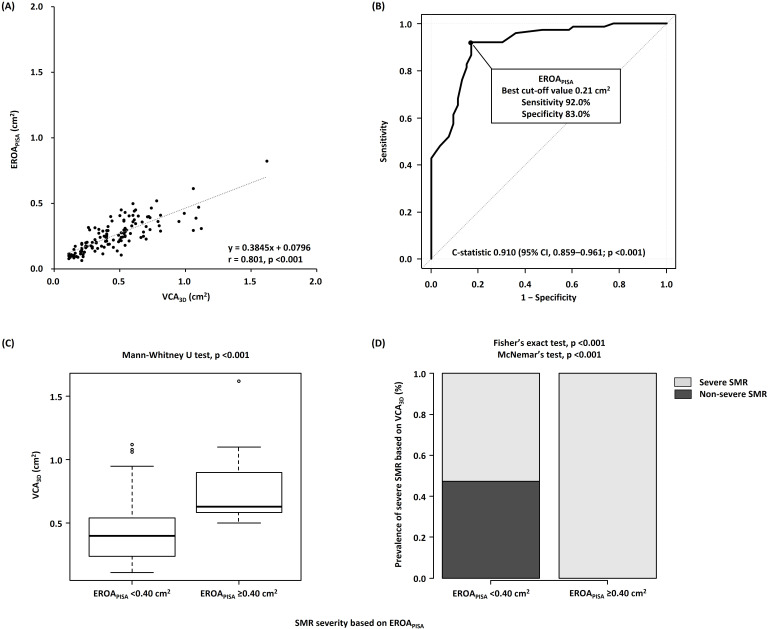 Fig. 2
Fig. 2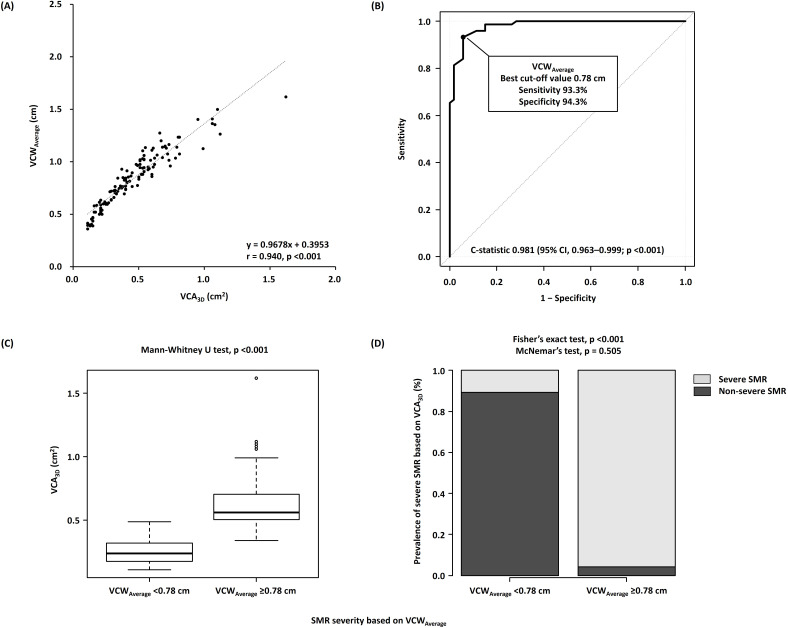 Fig. 3
Fig. 3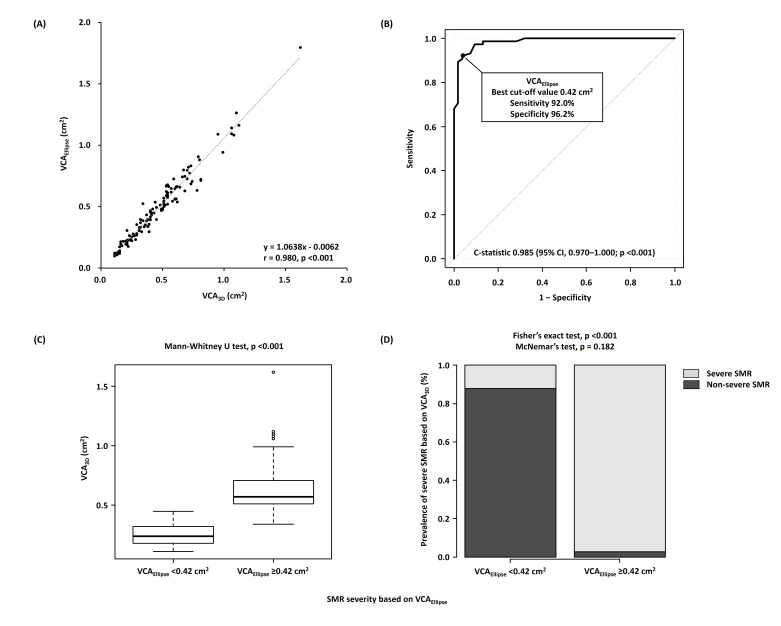 Fig. 4
Fig. 4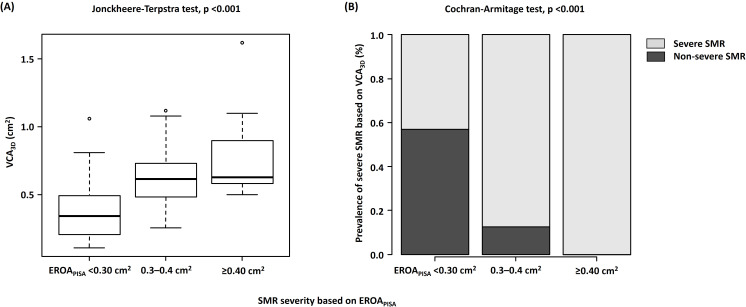 Fig. 5
Fig. 5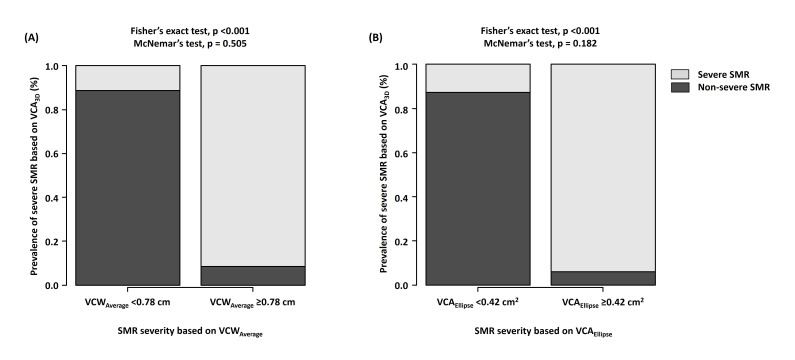 Fig. 6
Fig. 6| Variables | All patients (n = 128) | |
| Age, years | 77.0 | |
| Men, n | 78 (60.9) | |
| Body surface area, | 1.57 | |
| Hypertension, n | 66 (51.6) | |
| Diabetes mellitus, n | 42 (32.8) | |
| Dyslipidemia, n | 59 (46.1) | |
| Smoking, n | 71 (55.5) | |
| Chronic kidney disease (eGFR | 108 (84.4) | |
| Paroxysmal atrial fibrillation/flutter, n | 32 (25.0) | |
| Persistent atrial fibrillation/flutter, n | 64 (50.0) | |
| Irregular rhythm, n | 54 (42.2) | |
| Previous myocardial infarction, n | 35 (27.3) | |
| Pacemaker, n | 16 (12.5) | |
| Implantable cardioverter defibrillator, n | 16 (12.5) | |
| Cardiac resynchronization therapy, n | 7 (5.5) | |
| NYHA functional class | 2.1 | |
| I, n | 19 (14.8) | |
| II, n | 85 (66.4) | |
| III, n | 23 (18.0) | |
| IV, n | 1 (0.8) | |
| Variables | All patients (n = 128) | |
| Measurements on two-dimensional transthoracic echocardiography | ||
| LVEDV index, mL/ | 120.6 | |
| LVESV index, mL/ | 83.9 | |
| LVEF, % | 37.5 | |
| LVEF | 95 (74.2) | |
| Interventricular septum thickness, mm | 9.3 | |
| Posterior wall thickness, mm | 9.2 | |
| Left atrial volume index, mL/ | 119.8 | |
| PASP, mmHg | 41.6 | |
| Severe aortic stenosis, n | 0 (0.0) | |
| Severe aortic regurgitation, n | 3 (2.3) | |
| Severe mitral stenosis, n | 0 (0.0) | |
| Severe tricuspid regurgitation, n | 32 (25.0) | |
| Severe pulmonary regurgitation, n | 0 (0.0) | |
| Atrial septal defect, n | 5 (3.9) | |
| Measurements in mitral valve on three-dimensional transesophageal echocardiography | ||
| Heart rate, bpm | 70.0 | |
| Heart rate in 54 patients with irregular rhythm, bpm | 71.9 | |
| Anterior mitral leaflet pseudoprolapse, n | 42 (33.0) | |
| Tenting height, cm | 0.88 | |
| Anteroposterior annulus diameter, cm | 3.28 | |
| Mediolateral annulus diameter, cm | 3.49 | |
| 0.26 | ||
| 40.6 | ||
| Severe SMR based on | 16 (12.5) | |
| 0.49 | ||
| 1.19 | ||
| 0.46 | ||
| Severe SMR based on | 75 (58.6) | |
| 0.84 | ||
| Severe SMR based on | 72 (56.3) | |
| 0.49 | ||
| Severe SMR based on | 70 (54.7) | |
| 2.47 | ||
| Frame rate in | 18.4 | |
| Frame rate in | 18.8 | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Cardiovascular Function and Risk Factors · Atrial Fibrillation Management and Outcomes
1. Introduction
Secondary mitral regurgitation (SMR) is a common valvular heart disease that affects heart failure symptoms and clinical outcomes [1, 2, 3]. According to the current guidelines, two-dimensional (2D) echocardiographic parameters, including vena contracta width (VCW) and effective regurgitant orifice area by the proximal isovelocity surface area method ( ), are recommended to determine SMR severity; however, the severity may be underestimated using VCW and if regurgitant orifice area is elliptical [4, 5, 6].
Vena contracta area (VCA) hydrodynamically corresponds to the regurgitant
orifice area [7]. Kahlert et al. [8] primarily reported direct planimetry
of VCA ( ) based on three-dimensional transesophageal echocardiography
(3D-TEE), and was subsequently validated using an in vitro
model and cardiac magnetic resonance imaging [9, 10]. Furthermore, Goebel
et al. [11] reported that compared with , is a
robust parameter for discriminating severe SMR. Moreover, previous studies have
suggested that is elliptical in cases of SMR based on several vena contracta (VC)
parameters, including anteroposterior VCW ( ), mediolateral VCW
( ), average of and ( ), and VCA
calculated as an ellipse ( ). These studies have also reported that
the ellipticity consequently limited the ability of and
to accurately classify SMR severity [8, 12]. However, these were relatively
small-scale studies, and there is little information available regarding the best
cutoff values of VC parameters for severe SMR.
Thus, we hypothesized that parameters that considered the elliptical shape of the mitral regurgitant orifice, including and , are better surrogate markers for severe SMR based on than . This study also investigated the best cutoff values of these VC parameters for severe SMR. Furthermore, we reassessed the true SMR severity using the cutoff values of VC parameters to avoid underestimating SMR based on .
2. Methods
2.1 Patient Population
Patient characteristics and echocardiographic data were collected from the medical records and echocardiography reports. The study protocol was approved by the Institutional Review Board of New Tokyo Hospital and was in accordance with the guidelines of the Declaration of Helsinki. The requirement for informed consent was waived because of the retrospective nature of this study. Based on integrative methods using qualitative, semiquantitative, and quantitative approaches, 154 patients with at least mild SMR were identified via a review of echocardiography databases at New Tokyo Hospital between January 2018 and March 2021. These patients underwent 3D-TEE based on clinical indications and transthoracic echocardiography (TTE) within 1 month of 3D-TEE at our center [4]. SMR was defined as incomplete mitral leaflet closure because of regional myocardial dysfunction, global left ventricular remodeling, apical tethering of the mitral valve (MV), or annular dilation in the presence of an anatomically normal valve apparatus [4, 13]. Of 172 patients, those with multiple or nonholosystolic SMR jet (6 patients), previous MV intervention (7 patients), concomitant mitral stenosis (2 patients) [14], and mitral annular calcification (3 patients) were excluded from this study.
Overall, 19 of 154 patients were excluded because the quality of 3D imaging was inadequate for analysis, and 7 patients were excluded because of incomplete data for the quantitative assessment of SMR; hence, 128 patients were included in the final analysis.
2.2 Echocardiographic Parameters
Echocardiographic examinations were performed using iE33 system (Philips Healthcare, Andover, MA, USA) and EPIQ7 system (Philips Healthcare, Andover, MA, USA) equipped with a matrix-array transducer for transthoracic (X5-1) and transesophageal echocardiography (X7-2t and X8-2t), according to the guidelines for the clinical application of echocardiography [4, 14, 15, 16, 17, 18]. For offline analysis, echocardiographic data were stored in a computer at a dedicated workstation.
Regarding two-dimensional TTE (2D-TTE) parameters, left ventricular end-diastolic and -systolic volumes, left ventricular ejection fraction (LVEF), and left atrial volume were estimated using the biplane Simpson disk method via transthoracic echocardiography.
Regarding TEE parameters, and regurgitant volume ( )
were estimated using the proximal isovelocity surface area method [4]. A
continuous wave Doppler cursor was aligned parallel to the SMR jet for obtaining
peak velocity and velocity–time integral at a Nyquist limit of 50–70 cm/s, with
the gain set to a level immediately below the threshold for noise.
was derived using a color Doppler in a four-chamber view at an aliasing velocity
of 30–40 cm/s. Moreover, during systole, proximal isovelocity surface area (PISA) radius and flow velocity
parameters were obtained at similar time points for calculating . To
determine VC parameters, 3D color Doppler datasets were acquired from an
intercommissural view using full volume for each patient. The quantification of
was performed via multiplanar reconstruction using dedicated software
(Philips QLAB Versions 9.0, Philips Healthcare, Andover, MA, USA) (Fig. 1) [4].
The cropping plane was moved along the direction of the jet until the smallest
jet cross-sectional area became visible at the level of VC. Subsequently,
was measured using manual planimetry of the color Doppler flow signal.
and were also measured as anteroposterior and mediolateral
VCWs, respectively, in reconstructed 2D planes from the 3D-TEE dataset;
and were obtained in the left ventricular outflow tract and
intercommissural views (or views that were close to intercommissural views),
respectively [8]. was calculated as ( + )/2,
was calculated as
( /2)
( /2) [8], and shape index was calculated as
/ . In patients with irregular rhythm (i.e., atrial
fibrillation or flutter not requiring constant ventricular pacing for
bradycardia), these parameters were calculated as the mean of 3–5 parameters
performed by avoiding remarkable irregular RR intervals. and VC
parameters were performed by one observer (H.O.).
Assessment of vena contracta using 3D-TEE. A case of an 84-year-old woman with dilated cardiomyopathy and secondary mitral regurgitation. (A) Vena contracta described by multiplanar reconstruction of 3D color Doppler datasets. (B) VCA3D measured using manual planimetry of the vena contracta was 0.42 cm2. VCWAP and VCAML measured as the narrow and wide VCWs in the anteroposterior and mediolateral directions were 0.43 and 1.21 cm, respectively. VCWAverage, calculated as (VCWAP + VCWML)/2, was 0.82 cm. VCAEllipse, calculated as π × (VCWAP/2) × (VCWML/2), was 0.41 cm2. IC, intercommissural; LVOT, left ventricular outflow tract; 3D-TEE, three-dimensional transesophageal echocardiography; VCA3D, three-dimensional vena contracta area; VCWAP, anteroposterior vena contracta width; VCWML, mediolateral vena contracta width; VCWAverage, average of anteroposterior and mediolateral vena contracta widths; VCAEllipse, vena contracta area as an ellipse.
of 0.39 was used as a reference standard of severe SMR in the current study, considering that the severity of SMR may be underestimated using and that is a more robust parameter for distinguishing severe SMR than [4, 11].
2.3 Statistical Analysis
Categorical variables were presented as frequencies and analyzed using chi-square, Fisher’s exact, or Cochran–Armitage test, as appropriate. Continuous variables were presented as mean standard deviation or median with interquartile range and were compared using Mann–Whitney U or Jonckheere–Terpstra test, as appropriate. The overall rates of correct SMR severity classifications based on were statistically compared using McNemar’s test in 2 2 tables. Correlations between different parameters were determined using Pearson’s test and linear regression analysis. Receiver operating characteristic (ROC) curve analyses were performed to assess the ability of each parameter to identify severe SMR based on . The Youden index was used to determine the best cutoff value for severe SMR based on considering optimal sensitivity and specificity. Discrimination of severe SMR based on was assessed using the C-statistic. All statistical tests were two-tailed, and a two-sided p-value of 0.05 was considered to indicate statistical significance. Data analysis was performed using EZR software version 1.50 (Saitama Medical Center, Jichi Medical University, Saitama, Japan) [19].
3. Results
3.1 Patient Characteristics
The mean age of the patients was 77.0 8.9 years, and 78 (60.9%) patients were men (Table 1). Regarding echocardiographic data, the mean LVEF was 37.5% 13.4%, with an LVEF of 50% in 95 (74.2%) patients (Table 2). The mean tenting height of MV was 0.88 0.34 cm. Regarding SMR quantification, and were 0.26 0.12 and 40.6 17.3 mL, respectively, with severe SMR based on of 0.40 (according to the current guidelines) in 16 (12.5%) patients [4]. was 0.46 0.26 , with severe SMR based on in 75 (58.6%) patients. and were 0.84 0.26 cm and 0.49 0.28 , respectively.
3.2 Associations of EROAPISA with VCA3D
showed a strong correlation with (r = 0.801, *p *
0.001) (Fig. 2A). ROC curve analysis revealed that showed good
discrimination of severe SMR based on (C-statistic, 0.910; 95%
confidence interval [CI], 0.859–0.961; *p *
0.001), with the best
cutoff value of 0.21 (Fig. 2B). The sensitivity and specificity of
for severe SMR based on were as follows:
of 0.20 , 92.0% and 73.6%; of 0.30 , 49.3% and
94.3%; and of 0.40 , 22.6% and 100.0%; respectively. In
addition, and SMR incidence were significantly lower (*p *
0.001) in patients with nonsevere SMR based on of 0.40
(according to the current guidelines) than in those with severe SMR based on
of 0.40 (Fig. 2C,D) [4]. Notably, among 112
patients with nonsevere SMR based on of 0.40 , 59
(52.7%) had discordantly severe SMR based on . SMR severity based on
was not correctly reclassified as severe SMR by
(McNemar’s test; *p *
0.001).
Associations of VCA𝟑𝐃 with EROA𝐏𝐈𝐒𝐀. (A) Correlations between VCA3D and EROAPISA. (B) Receiver operating characteristic curve analyses of EROAPISA to identify severe SMR. (C) Comparison of VCA3D between the nonsevere (EROAPISA of <0.40 cm2) and severe (EROAPISA of ≥0.40 cm2) SMR groups. (D) Incidence of severe SMR based on VCA3D of ≥0.39 cm2 in the nonsevere (EROAPISA of <0.40 cm2) and severe (EROAPISA of ≥0.40 cm2) SMR groups. VCA3D, three-dimensional vena contracta area; EROAPISA, effective regurgitant orifice area by proximal isovelocity surface area method; SMR, secondary mitral regurgitation.
3.3 Associations of VCWAP with VCA3D
showed a strong correlation with (r = 0.786, *p * 0.001). ROC curve analysis indicated that showed relatively good discrimination of severe SMR based on (C-statistic, 0.874; 95% CI, 0.812–0.936; *p * 0.001), with the best cutoff value of 0.43 cm.
3.4 Associations of VCWAverage and VCAEllipse with
VCA3D
and had a strong correlation with (r
= 0.940, *p *
0.001 and r = 0.980, *p *
0.001, respectively)
(Figs. 3A,4A). According to ROC curve analysis, and
showed fairly good discrimination of severe SMR based on
(C-statistic, 0.981; 95% CI, 0.963–1.000; *p *
0.001 and
C-statistic, 0.985; 95% CI, 0.970–1.000; *p *
0.001, respectively),
with the best cutoff values of 0.78 cm and 0.42 , respectively (Figs. 3B,4B). Moreover, regarding the comparison of C-statistics, and
showed significantly better discrimination than
(p = 0.007 and p = 0.003, respectively).
Associations of VCA𝟑𝐃 with VCWVCW𝐀𝐯𝐞𝐫𝐚𝐠𝐞. (A) Correlations between VCA3D and VCWAverage. (B) Receiver operating characteristic curve analyses of VCWAverage to identify severe SMR. (C) Comparison of VCA3D between the nonsevere (VCWAverage of <0.78 cm) and severe (VCWAverage of ≥0.78 cm) SMR groups. (D) Incidence of severe SMR based on VCA3D of ≥0.39 cm2 in the nonsevere (VCWAverage of <0.78 cm) and severe (VCWAverage of ≥0.78 cm) SMR groups. VCA3D, three-dimensional vena contracta area; VCWAverage, average of anteroposterior and mediolateral vena contracta widths; SMR, secondary mitral regurgitation.
Associations of VCA𝟑𝐃 with VCA𝐄𝐥𝐥𝐢𝐩𝐬𝐞. (A) Correlations between VCA3D and VCAEllipse. (B) Receiver operating characteristic curve analyses of VCAEllipse to identify severe SMR. (C) Comparison of VCA3D between the nonsevere (VCAEllipse of <0.42 cm2) and severe (VCAEllipse of ≥0.42 cm2) SMR groups. (D) Incidence of severe SMR based on VCA3D of ≥0.39 cm2 in the nonsevere (VCAEllipse of <0.42 cm2) and severe (VCAEllipse of ≥0.42 cm2) SMR groups. VCA3D, three-dimensional vena contracta area; VCAEllipse, vena contracta area as an ellipse; SMR, secondary mitral regurgitation.
In addition, patients with nonsevere SMR, according to of
0.78 cm and of 0.42 , showed significantly lower
(*p *
0.001 for both) and SMR incidence based on
(*p *
0.001 for both) than those with severe SMR based on
and (Fig. 3C,D and Fig. 4C,D). Notably, SMR
severity based on was correctly reclassified as severe SMR based on
(p = 0.505) and (p = 0.182).
3.5 SMR Severity Based on EROAPISA Considering VCWAverage
and VCAEllipse
Our patients were classified into the following three subgroups based on according to the current guidelines [4]: 88 patients with of 0.30 , 24 patients with of 0.30–0.40 , and 16 patients with of 0.40 . According to the incremental , (*p * 0.001) and SMR incidence based on (*p * 0.001) significantly increased (Fig. 5A,B). Notably, in patients with of 0.30 , which is suggestive of moderate SMR according to the current guidelines, 38 of 88 (43.2%) patients had severe MR based on . However, SMR severity based on in patients with of 0.30 was correctly reclassified as severe MR based on (p = 0.505) and (p = 0.182) (Fig. 6A,B).
Associations between VCA𝟑𝐃 and EROA𝐏𝐈𝐒𝐀 among the three subgroups (EROA𝐏𝐈𝐒𝐀 of <0.30 cm2, EROA𝐏𝐈𝐒𝐀 of 0.30–0.40 cm2, and EROA𝐏𝐈𝐒𝐀 of ≥0.40 cm2). (A) Increase in VCA3D according to the increase in SMR severity. (B) Incidence of severe SMR based on VCA3D of ≥0.39 cm2 according to the increase in SMR severity. VCA3D, three-dimensional vena contracta area; EROAPISA, effective regurgitant orifice area by proximal isovelocity surface area method; SMR, secondary mitral regurgitation.
Associations of VCA𝟑𝐃 with VCW𝐀𝐯𝐞𝐫𝐚𝐠𝐞 and VCA𝐄𝐥𝐥𝐢𝐩𝐬𝐞 in the EROA𝐏𝐈𝐒𝐀 <0.30 cm2 group. (A) Incidence of severe SMR based on VCA3D of ≥0.39 cm2 between the nonsevere (VCWAverage of <0.78 cm) and severe (VCWAverage of ≥0.78 cm) SMR groups. (B) Incidence of severe SMR based on VCA3D of ≥0.39 cm2 between the nonsevere (VCAEllipse of <0.42 cm2) and severe (VCAEllipse of ≥0.42 cm2) SMR groups. VCA3D, three-dimensional vena contracta area; VCWAverage, average of anteroposterior and mediolateral vena contracta widths; VCAEllipse, vena contracta area as an ellipse; EROAPISA, effective regurgitant orifice area determined by the proximal isovelocity surface area method; SMR, secondary mitral regurgitation.
4. Discussion
The current study revealed the following findings: (1) and
had a fairly strong correlation with , with the best
cutoff values of 0.78 cm and 0.42 , respectively, and (2)
of 0.78 cm and of 0.42 might be useful
in identifying severe SMR based on , particularly in patients with
of 0.30 , corresponding to moderate SMR according to the
current guidelines, who are at potential risk of underestimation of SMR severity
because of the ellipticity of regurgitant orifice area [4].
4.1 Usefulness of VCWAverage and VCAEllipse in Identifying
Severe SMR
Although was shown to be a reliable semiquantitative parameter for
evaluating SMR severity according to the current guidelines,
evaluation is not routinely used as a stand-alone parameter [4]. However,
according to a previous study by Kahlert et al. [8], was more
strongly correlated with than with . Furthermore,
is strongly correlated with [8]. To accurately
identify severe SMR, the current guidelines recommend calculating
with a cutoff value of 0.80 cm for severe SMR if the regurgitant orifice area is
elliptical [4]. However, there is little information on the discrimination and
best cutoff value of for severe SMR. Our study indicated that
had a fairly strong correlation with and showed
adequately good discrimination of severe SMR. Notably, the best cutoff value of
was 0.78 cm—which is close to the value of 0.80 cm according to
the current guidelines—with adequately high sensitivity and specificity for
severe SMR based on [4]. Further, had a strong
correlation with and showed good discrimination of severe SMR.
Moreover, the best cutoff value of was 0.42 , with high
sensitivity and specificity for severe SMR based on .
The current study and previous studies have demonstrated that the regurgitant orifice area in SMR may be elliptical [8, 12], indicating that SMR severity based on and is underestimated [4, 5, 6]. Furthermore, there was a weak correlation between the shape index and difference between and ; this finding conforms to that reported by Goebel et al. [11], suggesting that the ellipticity of the regurgitant orifice area rather than the extent of ellipticity is related to the underestimation of SMR severity based on .
4.2 Assessment of SMR Severity to Avoid its Underestimation
Patients with SMR having of 0.30 , corresponding to moderate SMR according to the current guidelines, have a potential risk of underestimation of SMR severity because of the elliptical regurgitant orifice area [4]. Of the 88 patients with of 0.30 in the current study, 38 (43.2%) had severe MR based on . In such cases, of 0.78 cm and/or of 0.42 might be useful in identifying discordantly severe SMR based on . If is 0.30 , SMR severity is expected to be truly severe based on ; however, of 0.30 does not necessarily indicate nonsevere SMR based on . If of 0.78 cm and/or of 0.42 are calculated using and , SMR severity might be considered discordantly severe despite the of 0.30 . After the exclusion of severe SMR according to the abovementioned assessment, symptomatic patients may be evaluated using exercise-stress echocardiography to confirm significantly worsening SMR, if applicable.
4.3 Clinical Implications
Although severe SMR is associated with adverse clinical outcomes [1, 2, 3], it may be underestimated using conventional echocardiographic parameters, including and . Moreover, an inaccurate assessment of SMR severity can lead to misleading indications for optimal MV interventions, including MV transcatheter edge-to-edge repair, which is known to be effective and is recommended in patients with SMR with reduced LVEF [5, 20, 21]. Karam et al. [22] reported that MV transcatheter edge-to-edge repair for SMR is equally effective in patients with of 0.30 and those with of 0.30 in terms of clinical outcomes, suggesting that patients with of 0.30 may have a higher severity of SMR than expected based on . To obtain an accurate evaluation of SMR severity, is useful as a substantially reliable echocardiographic parameter [11]. However, the assessment of is relatively time-consuming and requires good quality of 3D-echocardiographic data [4]. and , which were calculated via simple equations using and , showed fairly strong correlations with and good discrimination of severe SMR based on . Therefore, instead of , and , with best cutoff values of 0.78 cm and 0.42 , respectively, might be helpful in identifying true severe SMR.
5. Study Limitations
This study has several important limitations. First, this was a small-scale
retrospective analysis of patients with SMR who underwent TEE, with a
considerable bias in data accumulation (i.e., selection bias). Second, our study
defined severe SMR as of 0.39 based on the findings
of a previous study [11]. However, our results may not be accurate when using
other definitions of severe SMR based on modalities other than echocardiography,
including cardiac magnetic resonance imaging. Third, TEE and TTE were not
performed on the same day. Hence, there might have been differences in the
hemodynamic status at the time of TEE and TTE. Finally, we measured
and using 3D-TEE data, which may not be similar to and
determined using 2D-TEE. However, there were no significant
differences between and measured using 3D-TEE and
2D-echocardiography according to a previous study [8].
6. Conclusions
and based on 3D-TEE were strongly associated with . Therefore, in general, the regurgitant orifice area of SMR may be elliptical, and SMR severity might be underestimated if determined using only and . Hence, and , with best cutoff values of 0.78 cm and 0.42 , respectively, were useful in identifying severe SMR.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sannino A Smith RL 2nd Schiattarella GG Trimarco B Esposito G Grayburn PA Survival and Cardiovascular Outcomes of Patients With Secondary Mitral Regurgitation: A Systematic Review and Meta-analysis JAMA Cardiology 20172113011392887729110.1001/jamacardio.2017.2976 PMC 5710448 · doi ↗ · pubmed ↗
- 2Goliasch G Bartko PE Pavo N Neuhold S Wurm R Mascherbauer J et al Refining the prognostic impact of functional mitral regurgitation in chronic heart failure European Heart Journal 20183939462902033710.1093/eurheartj/ehx 402 · doi ↗ · pubmed ↗
- 3Barakat AF Raza MQ Banerjee K Tsutsui RS Mentias A Abdur Rehman K et al Long-term mortality in patients with severe secondary mitral regurgitation and normal left ventricular ejection fraction: interventional perspective Euro Intervention 201813188118882931381810.4244/EIJ-D-17-00561 · doi ↗ · pubmed ↗
- 4Zoghbi WA Adams D Bonow RO Enriquez-Sarano M Foster E Grayburn PA et al Recommendations for Noninvasive Evaluation of Native Valvular Regurgitation: A Report from the American Society of Echocardiography Developed in Collaboration with the Society for Cardiovascular Magnetic Resonance Journal of the American Society of Echocardiography 2017303033712831462310.1016/j.echo.2017.01.007 · doi ↗ · pubmed ↗
- 5Otto CM Nishimura RA Bonow RO Carabello BA Erwin JP 3rd Gentile F et al 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines Journal of the American College of Cardiology 202177 e 25e 1973334258610.1016/j.jacc.2020.11.018 · doi ↗ · pubmed ↗
- 6Ashikhmina E Shook D Cobey F Bollen B Fox J Liu X et al Three-dimensional versus two-dimensional echocardiographic assessment of functional mitral regurgitation proximal isovelocity surface area Anesthesia and Analgesia 20151205345422516646510.1213/ANE.0000000000000409 · doi ↗ · pubmed ↗
- 7Yoganathan AP Cape EG Sung HW Williams FP Jimoh A Review of hydrodynamic principles for the cardiologist: applications to the study of blood flow and jets by imaging techniques Journal of the American College of Cardiology 19881213441353317097710.1016/0735-1097(88)92620-4 · doi ↗ · pubmed ↗
- 8Kahlert P Plicht B Schenk IM Janosi RA Erbel R Buck T Direct assessment of size and shape of noncircular vena contracta area in functional versus organic mitral regurgitation using real-time three-dimensional echocardiography Journal of the American Society of Echocardiography 2008219129211838501310.1016/j.echo.2008.02.003 · doi ↗ · pubmed ↗