Long-Term Outcomes of Endovascular Treatment for Type B Aortic Dissection with Simple Renal Cysts: A Multicenter Retrospective Study
Hongqiao Zhu, Kaiwen Zhao, Guangkuo Wang, Junjun Liu, Yifei Pei, Jian Zhou, Zaiping Jing

TL;DR
This study finds that type B aortic dissection patients with simple renal cysts face higher long-term risks after aortic repair surgery.
Contribution
The study identifies simple renal cysts as an independent predictor of adverse aortic events after TEVAR in type B aortic dissection patients.
Findings
BAD patients with SRC had higher long-term aortic-related adverse events after TEVAR.
SRC was an independent predictor of adverse events (hazard ratio: 1.84).
SRC combined with hypertension significantly increased rupture risk after TEVAR.
Abstract
Few studies have investigated the characteristics and long-term outcomes of type B aortic dissection (BAD) patients with simple renal cysts (SRC) after thoracic endovascular aortic repair (TEVAR). A multi-center retrospective cohort study was performed, including 718 BAD patients undergoing TEVAR from 2003 to 2016. The prevalence of SRC was 34.5% (n = 248). After propensity score matching, 214 matched pairs were selected for further analysis. Primary outcomes were long-term aortic-related adverse events (ARAEs). The effects of SRC in each subgroup of interest and their interactions were analyzed. BAD patients with SRC were older and had a greater prevalence of comorbidities, including hypertension, coronary artery disease and chronic occlusive pulmonary disease. In addition, the SRC group presented a greater proportion of pleural effusion and aortic calcification. Compared…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
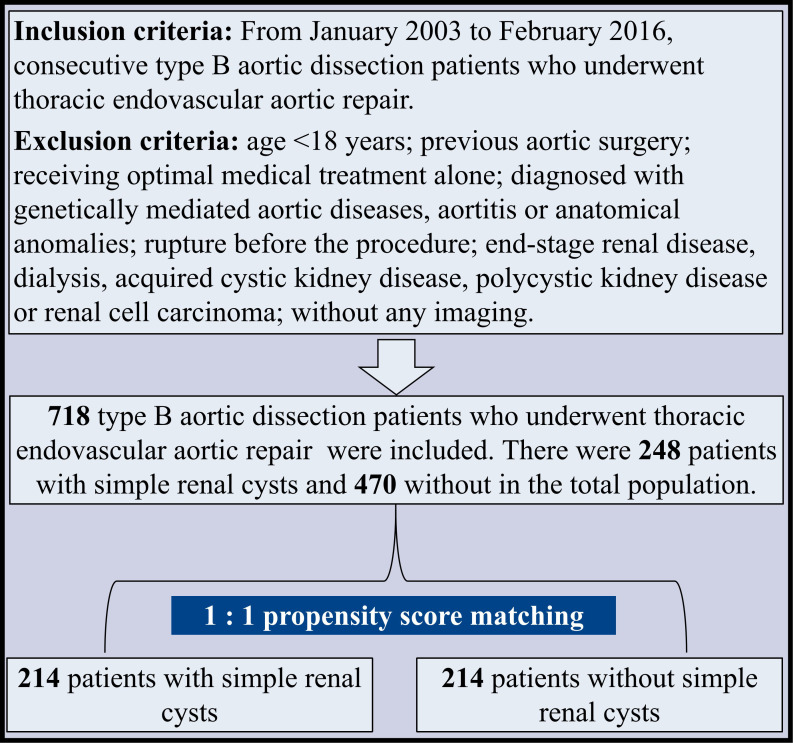 Fig. 1
Fig. 1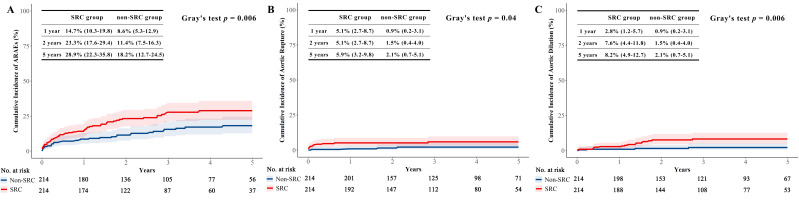 Fig. 2
Fig. 2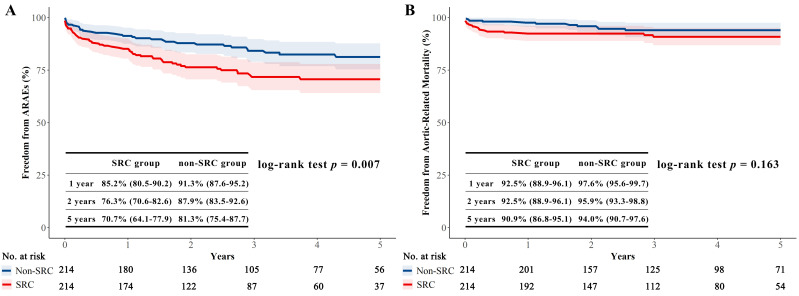 Fig. 3
Fig. 3| Variables | Overall | Matched population | |||||||
| SRC group | Non-SRC group | SMD | SRC group | Non-SRC group | SMD | ||||
| n = 248 | n = 470 | n = 214 | n = 214 | ||||||
| Baseline characteristics | |||||||||
| Age (y) | 61.1 | 56.3 | 0.38 | 59.5 | 60.3 | 0.06 | 0.494 | ||
| Male | 199 (80.2%) | 396 (84.3%) | 0.11 | 0.175 | 172 (80.4%) | 176 (82.2%) | 0.05 | 0.62 | |
| BMI | 24.4 | 24.7 | 0.1 | 0.254 | 24.6 | 24.6 | 0.01 | 0.893 | |
| Smoking | 135 (54.4%) | 245 (52.1%) | 0.05 | 0.556 | 116 (54.2%) | 120 (56.1%) | 0.04 | 0.697 | |
| Drinking | 47 (19.0%) | 99 (21.1%) | 0.05 | 0.504 | 44 (20.6%) | 45 (21.0%) | 0.01 | 0.905 | |
| Hypertension | 205 (82.7%) | 349 (74.3%) | 0.21 | 0.011 | 174 (81.31%) | 169 (78.97%) | 0.06 | 0.545 | |
| CAD | 22 (8.9%) | 18 (3.8%) | 0.21 | 0.005 | 12 (5.6%) | 14 (6.5%) | 0.04 | 0.686 | |
| Arrhythmia | 32 (12.9%) | 52 (11.1%) | 0.06 | 0.466 | 25 (11.7%) | 34 (15.9%) | 0.12 | 0.207 | |
| Stroke | 10 (4.03%) | 17 (3.62%) | 0.02 | 0.781 | 8 (3.7%) | 11 (5.1%) | 0.07 | 0.481 | |
| COPD | 46 (18.6%) | 27 (5.7%) | 0.40 | 23 (10.8%) | 26 (12.2%) | 0.04 | 0.649 | ||
| Diabetes mellitus | 21 (8.5%) | 37 (7.9%) | 0.02 | 0.781 | 16 (7.5%) | 24 (11.2%) | 0.13 | 0.184 | |
| CKD | 16 (6.5%) | 19 (4.0%) | 0.11 | 0.154 | 14 (6.5%) | 8 (3.7%) | 0.13 | 0.189 | |
| SBP at admission (mmHg) | 138.7 | 138.0 | 0.03 | 0.669 | 137.9 | 137.6 | 0.01 | 0.956 | |
| DBP at admission (mmHg) | 82.9 | 82.3 | 0.05 | 0.509 | 83.0 | 81.2 | 0.15 | 0.115 | |
| Pleural effusion | 104 (41.9%) | 127 (27.0%) | 0.32 | 84 (39.3%) | 76 (35.5%) | 0.08 | 0.424 | ||
| Malperfusion | 18 (7.26%) | 23 (4.89%) | 0.1 | 0.194 | 16 (7.5%) | 9 (4.2%) | 0.14 | 0.149 | |
| Echocardiography parameters | |||||||||
| Diameters of ascending aorta (cm) | 3.4 | 3.4 | 0.06 | 0.643 | 3.4 | 3.4 | 0.06 | 0.677 | |
| LVEF (%) | 61.8 | 62.2 | 0.08 | 0.434 | 61.9 | 62.5 | 0.12 | 0.482 | |
| Medication in hospital | |||||||||
| ACEI/ARB | 140 (56.5%) | 239 (50.9%) | 0.11 | 0.153 | 111 (51.87%) | 112 (52.34%) | 0.01 | 0.923 | |
| 96 (38.7%) | 187 (39.8%) | 0.02 | 0.779 | 81 (37.9%) | 86 (40.2%) | 0.05 | 0.62 | ||
| 167 (67.3%) | 339 (72.1%) | 0.1 | 0.181 | 143 (66.8%) | 146 (68.2%) | 0.03 | 0.757 | ||
| CCB | 187 (75.4%) | 352 (74.9%) | 0.01 | 0.881 | 160 (74.8%) | 147 (68.7%) | 0.14 | 0.163 | |
| Diuretic | 33 (13.3%) | 60 (12.8%) | 0.02 | 0.838 | 27 (12.6%) | 35 (16.4%) | 0.11 | 0.272 | |
| Anatomical characteristics | |||||||||
| Arch type | 0.07 | 0.641 | 0.12 | 0.459 | |||||
| I | 83 (33.5%) | 157 (33.4%) | 68 (31.8%) | 71 (33.2%) | |||||
| II | 32 (12.9%) | 50 (10.6%) | 27 (12.6%) | 19 (8.9%) | |||||
| III | 133 (53.6%) | 263 (56.0%) | 119 (55.6%) | 124 (57.9%) | |||||
| Diameters of maximum ascending aorta (mm) | 40.2 | 38.3 | 0.35 | 0.012 | 38.9 | 38.2 | 0.12 | 0.413 | |
| Diameters of maximum descending aorta (mm) | 44.1 | 44.1 | 0.01 | 0.97 | 44.3 | 44.2 | 0.01 | 0.772 | |
| Calcification | 0.66 | 0.13 | 0.595 | ||||||
| None | 93 (37.5%) | 319 (67.9%) | 87 (40.65%) | 95 (44.39%) | |||||
| Mild | 105 (42.3%) | 117 (24.9%) | 89 (41.59%) | 91 (42.52%) | |||||
| Moderate | 40 (16.1%) | 26 (5.5%) | 31 (14.49%) | 23 (10.75%) | |||||
| Severe | 10 (4.0%) | 8 (1.7%) | 7 (3.27%) | 5 (2.34%) | |||||
| Thrombosis | 0.15 | 0.331 | 0.08 | 0.879 | |||||
| Patent | 113 (45.6%) | 182 (38.7%) | 95 (44.4%) | 90 (42.1%) | |||||
| Partial | 83 (33.5%) | 174 (37.0%) | 74 (34.6%) | 72 (33.6%) | |||||
| Complete | 34 (13.7%) | 79 (16.8%) | 29 (13.6%) | 34 (15.9%) | |||||
| ULP | 18 (7.3%) | 35 (7.5%) | 16 (7.5%) | 18 (8.4%) | |||||
| Variables | Overall | Matched population | |||||||
| SRC group | Non-SRC group | SMD | SRC group | Non-SRC group | SMD | ||||
| n = 248 | n = 470 | n = 214 | n = 214 | ||||||
| Operation time (min) | 120.0 (79.0–156.3) | 115.0 (80.0–160.0) | 0.07 | 0.448 | 120.0 (80.0–160.0) | 115.0 (80.0–150.0) | 0.07 | 0.629 | |
| Oversize (%) | 15.8 (7.4–23.5) | 16.1 (7.4–33.5) | 0.45 | 0.074 | 16.1 (8.0–27.1) | 12.5 (6.6–28.7) | 0.05 | 0.792 | |
| Length of proximal landing zone (mm) | 24.0 (17.3–32.8) | 20.6 (14.1–30.3) | 0.22 | 0.239 | 22.4 (15.0–32.3) | 22.0 (15.8–34.8) | 0.02 | 0.802 | |
| Timing of operation | 0.22 | 0.02 | 0.05 | 0.856 | |||||
| Acute phase | 153 (61.7%) | 239 (50.9%) | 128 (59.8%) | 127 (59.4%) | |||||
| Subacute phase | 64 (25.8%) | 160 (34.0%) | 59 (27.6%) | 63 (29.4%) | |||||
| Chronic phase | 31 (12.5%) | 71 (15.1%) | 27 (12.6%) | 24 (11.2%) | |||||
| Hybrid approach | 1 (0.4%) | 10 (2.1%) | 0.15 | 0.074 | 1 (0.5%) | 4 (1.9%) | 0.13 | 0.372 | |
| Chimney technique | 51 (20.6%) | 77 (16.4%) | 0.11 | 0.164 | 45 (21.0%) | 36 (16.8%) | 0.11 | 0.267 | |
| Adjunctive procedure | 44 (17.7%) | 97 (20.6%) | 0.07 | 0.353 | 40 (18.7%) | 45 (21.0%) | 0.06 | 0.545 | |
| Era | 0.03 | 0.697 | 0.03 | 0.771 | |||||
| 2003–2010 | 106 (42.7%) | 208 (44.3%) | 98 (45.8%) | 95 (44.4%) | |||||
| 2011–2016 | 142 (57.3%) | 262 (55.7%) | 116 (54.2%) | 119 (55.6%) | |||||
| Variables | Hazard ratio (95% CI) | ||
| SRC | 1.84 (1.13, 3.00) | 0.014 | |
| Stroke | 2.62 (1.31, 5.24) | 0.006 | |
| Timing of operation | |||
| Acute phase | Reference | ||
| Subacute phase | 1.56 (0.92, 2.64) | 0.098 | |
| Chronic phase | 2.16 (1.16, 4.02) | 0.015 | |
| Outcomes | Hazard ratio (95% CI) | |||
| ARAEs | 0.917 | |||
| Overall | 1.84 (1.13–3.00) | 0.014 | ||
| Normotension | 1.64 (0.55–4.89) | 0.372 | ||
| Hypertension | 1.77 (1.09–2.85) | 0.02 | ||
| Aortic-related mortality | 0.472 | |||
| Overall | 1.74 (0.82–3.69) | 0.147 | ||
| Normotension | 0.7 (0.06–7.75) | 0.773 | ||
| Hypertension | 1.78 (0.79–4.00) | 0.161 | ||
| Rupture | 0.023 | |||
| Overall | 3.13 (1.01–9.72) | 0.048 | ||
| Normotension | 0.92 (0.15–5.51) | 0.926 | ||
| Hypertension | 5.58 (1.25–24.95) | 0.024 | ||
| Endoleak | 0.398 | |||
| Overall | 1.19 (0.43–3.28) | 0.739 | ||
| Normotension | 2.81 (0.26–31.0) | 0.399 | ||
| Hypertension | 0.96 (0.31–2.98) | 0.946 | ||
| Aortic dilation | 0.918 | |||
| Overall | 4.17 (1.39–12.48) | 0.011 | ||
| Normotension | 4.05 (0.42–38.98) | 0.226 | ||
| Hypertension | 4.27 (1.21–15.00) | 0.023 | ||
| New dissection | NA | |||
| Overall | 1.11 (0.07–17.8) | 0.942 | ||
| Normotension | NA | NA | ||
| Hypertension | 1.07 (0.07–17.21) | 0.961 | ||
| Retrograde AD | 0.602 | |||
| Overall | 1.29 (0.53–3.12) | 0.573 | ||
| Normotension | 0.73 (0.07–8.01) | 0.794 | ||
| Hypertension | 1.39 (0.53–3.64) | 0.509 | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAortic Disease and Treatment Approaches · Aortic aneurysm repair treatments · Renal and Vascular Pathologies
1. Introduction
Aortic dissection (AD) is a devastating aortic disease caused by an entry tear in the aortic intima or hemorrhage in the aortic media, leading to the separation of the aortic layers [1]. According to the Stanford classification, type B aortic dissection (BAD) originates distal to the ostium of the left subclavian artery [1]. With the development of thoracic endovascular aortic repair (TEVAR), the mortality rate of BAD patients has significantly reduced [2]. Nonetheless, patients can still suffer from diverse stent-graft-related complications, including endoleak, aortic dilation, retrograde type A aortic dissection (AAD) and new dissection [2]. Therefore, it is imperative to identify potential risk factors associated with aortic-related adverse events (ARAEs) in BAD patients undergoing TEVAR.
Recently published studies have found an association between simple renal cysts (SRC) and aortic dissection/aneurysm [3, 4]. However, the perioperative characteristics and long-term outcomes of BAD patients with SRC that undergo TEVAR remain unclear. In this context, a multi-center retrospective study was conducted. First of all, differences in perioperative characteristics and intraoperative details between SRC and non-SRC groups were compared. Moreover, a propensity score matching was performed to minimize selection bias. The differences in long-term outcomes between the two groups were compared in the overall and matched study populations. Finally, subgroup analysis was performed to identify which subpopulations of SRC patients sustained the highest risk of ARAEs after TEVAR.
2. Methods
2.1 Study Population
A multi-center retrospective analysis was performed, including three Chinese tertiary referral centers (Supplementary Table 1). Consecutive BAD patients who underwent TEVAR from January 2003 to February 2016 were included in this study. A flowchart of the study population is shown in Fig. 1.
Flowchart of the study population. A multi-center retrospective cohort study was performed, including 718 BAD patients undergoing TEVAR from 2003 to 2016, consisting of 248 and 470 patients with and without SRC. After propensity score matching, 214 matched pairs were taken into further analysis.
2.2 TEVAR Procedure
The indications of TEVAR for complicated and uncomplicated BAD were reported in our previous studies [5]. All procedures were performed as previously described [5, 6].
2.3 Study Definitions and Follow-Up
The duration of BAD was divided into acute ( 15 days after onset), subacute (15–90 days) and chronic phases ( 90 days) [7]. CTA data on the admission of the eligible patients were retrospectively reviewed to assess the anatomical characteristics, including arch type, aortic calcification, thrombosis status of the false lumen, maximal diameter of the ascending and descending aorta according to the guidelines of the Society for Vascular Surgery [8].
The presence of SRC was confirmed by the CT or magnetic resonance imaging on admission. The same definition was used to diagnose SRC in all participating centers: a lesion characterized with round shape, thin wall, size 4 mm, with low attenuation and no distinct enhancement or septations radiographically [9]. BAD patients were then divided into SRC and non-SRC groups.
Primary outcomes were defined as any ARAEs, including endoleak (type I, II and III), new dissection, retrograde AAD, aortic dilation, rupture (of the false lumen) and aortic-related mortality at 5-year follow-up [2]. The in-hospital aortic-related mortality was evaluated by reviewing the inpatient record, death and autopsy reports, while the out-of-hospital mortality was determined by phone calls. Secondary outcomes included all-cause mortality and cardiovascular events at the five-year follow-up. A short-term outcome was defined as any clinical adverse event described at 30-day follow-up, while a long-term outcome was defined as any events occurring at the 5-year follow-up. The follow-up was performed until February 2021. The completeness of follow-up of our study was estimated using the Clark C index [10].
2.4 Statistical Analysis
Data were presented as n (%) for categorical variables and mean standard deviations or median (interquartile range, IQR) for continuous variables. The Chi-square test or Fisher exact test was used to compare categorical variables, while the student t-test was used to compare continuous variables.
To minimize selection bias and improve confounding variable balance, adverse clinical outcomes were compared using propensity-matched data for the 214 pairs of SRC and non-SRC patients. The propensity score matching was conducted using a caliper width of 0.1. Maximal SMD was usually considered acceptable with a value 0.2 [11, 12]. All variables in Tables 1,2 were included in the matching process.
Table 1.: Preoperative characteristics of patients with and without SRC and propensity-matched population.
Table 2.: Intra-operative details of patients with and without SRC and propensity-matched population.
To identify potential risk factors for ARAEs, Cox hazard analysis was used in the matched population. Variables that had a significant correlation (*p * 0.1) in the univariate analysis were selected for multivariable analysis using the backward selection method. All tests were two-sided, and a p-value 0.05 was statistically significant. Statistical package R version 3.4.3 (R Foundation for Statistical Computing, Vienna, Austria) was used to analyze the data.
3. Results
3.1 Clinical Characteristics
From January 2003 to February 2016, 718 patients were enrolled in the study, of whom 595 were males (82.9%), and 248 presented with at least one SRC (34.5%) (Table 1). Patients with SRC were older (61.1 12.6 years versus 56.3 12.7 years; *p * 0.001) and had a greater prevalence of comorbidities, including hypertension (p = 0.011), coronary artery disease (CAD) (p = 0.005) as well as chronic occlusive pulmonary disease (COPD) (*p * 0.001). Compared with the non-SRC group, BAD patients with SRC presented a greater pleural effusion prevalence (*p * 0.001). Anatomically, a greater proportion of patients with SRC presented with aortic calcification (*p * 0.001) and the maximal diameter of the ascending aorta was significantly larger in patients with SRC (p = 0.012).
3.2 Intra-Operative Details
Table 2 shows the differences in intra-operative details between the SRC and non-SRC groups.
3.3 Outcomes
Short-term outcomes in the overall and matched population were shown in the Supplementary Table 2.
The median length of follow-up in the matched population was 3.6 (IQR: 1.7–5.9) years and 3.1 (IQR: 1.2–5.7) years for patients with and without SRC, respectively. The completeness of follow-up for the primary outcomes was 67.3% for the SRC group and 68.1% for the non-SRC group. In the matched population, ARAEs were significantly lower in the non-SRC group than in the SRC group (Gray’s test p = 0.006 and log-rank p = 0.007) (Fig. 2A and Fig. 3A). In terms of 5-year aortic rupture, the cumulative incidence was 5.9% in the SRC group and 2.1% in the non-SRC group (p = 0.04) (Fig. 2B). Cumulative incidence of 5-year aortic dilation was also higher in patients with SRC (8.2% vs. 2.1%, p = 0.006) (Fig. 2C). No difference was observed in the aortic-related mortality between the two groups (log-rank p = 0.163) (Fig. 3B). Supplementary Figs. 1–4 show the cumulative incidences of aortic-related mortality, endoleak, retrograde AAD and new dissection in the matched population. Long-term outcomes in the total population are presented in the Supplementary Table 3.
The cumulative incidences of the ARAEs, rupture and aortic dilation, with all-cause death as the competing risk in the matched population. (A)The cumulative incidence of ARAEs in the SRC group was significantly greater than in the non-SRC group (p = 0.006). (B) The cumulative incidence of rupture in the SRC group was significantly greater than in the non-SRC group (p = 0.04). (C) The cumulative incidence of aortic dilation in the SRC group was significantly greater than in the non-SRC group (p = 0.006). The differences were assessed with Gray’s test.
Kaplan-Meier survival analysis of ARAEs and aortic-related mortality in the matched population. (A) Freedom from ARAEs between the SRC and non-SRC groups. Freedom from ARAEs in the SRC group was significantly lower than that of the non-SRC group (p = 0.007). (B) Freedom from aortic-related mortality between the two groups. Freedom from aortic-related mortality in the SRC group was similar with that of the non-SRC group (p = 0.163). The differences between the SRC and non-SRC groups were assessed with log-rank test.
3.4 Outcomes Analysis
Univariate Cox hazard analysis indicated that SRC, hypertension, chronic occlusive pulmonary disease, operation time, stroke, malperfusion, chronic aortic dissection, maximum diameters of descending aorta were potential risk factors for ARAEs (*p * 0.1) (Supplementary Table 4). Multivariable Cox hazard analysis revealed that SRC (HR: 1.84, 95% CI: 1.13–3.00), stroke (HR: 2.62, 95% CI: 1.31–5.24), chronic aortic dissection (HR: 2.16, 95% CI: 1.16–4.02) were independent risk factors of ARAEs (Table 3).
Table 3.: Multivariable Cox hazard analysis of ARAEs in the matched population.
As seen in Table 4, a statistically significant interaction between SRC and hypertension on the risk of rupture after TEVAR was found (p = 0.023).
Table 4.: Multivariable Cox analyses in the matched population for ARAEs, aortic-related mortality, rupture, endoleak, aortic dilation, new dissection and retrograde AAD.
When patients were stratified according to potential impact factors for ARAEs, no significant interactions with SRC were found for age, hypertension, stroke, operation timing, chimney technique, adjunctive procedure and hybrid approach (Supplementary Table 5).
4. Comment
Although previous studies indicated that SRC is a significant risk factor for BAD patients undergoing TEVAR [4], the relatively short follow-up periods and small sample size in these studies could be a source of selection and observational bias. To our best knowledge, this is the largest and most contemporary report providing comprehensive analyses of SRC-related disparities in baseline characteristics, anatomical patterns, intra-operative details and long-term outcomes of BAD patients after TEVAR.
In our study, BAD patients with SRC were significantly older than those without, consistent with the literature [13]. In comparison with the general population, patients with BAD were found to be older [14]. Clinical evidence from the international registry of acute aortic dissection (IRAD) showed that the mean age of BAD patients was 63.5 years (the mean age in our study is 57.9 years) [15]. Moreover, we found that the SRC group was significantly older than the non-SRC group (mean age, 61.1 years vs. 56.3 years; *p * 0.001). However, no significant interaction between age and SRC on ARAEs was found (p for interaction = 0.429, Supplementary Table 5). Our results indicated that age, although related to SRC, is not the major factor influencing aortic-related outcomes in BAD patients after TEVAR.
A significant gender imbalance was found in SRC patients in our study, with a male-to-female ratio of 4.8:1. Moreover, female patients were significantly older than male patients (62.1 12.9 years vs. 57.1 12.7 years, *p * 0.001), while the prevalence of SRC between the two groups was similar (39.8% vs. 33.4%, p = 0.175). In a study by Chung et al. [16], female patients that underwent cardiac surgery were older with larger indexed aortic sizes, with a lower prevalence of coronary disease and reduced left ventricular ejection fraction than their male counterparts. In our study, the prevalence of CAD (p = 0.174), stroke (p = 0.781), COPD (p = 0.07) and CKD (p = 0.357) was similar between the males and females, while hypertension was predominantly found in male patients (*p * 0.001).
In our study, a difference was found in the prevalence of hypertension between the two groups in the total population (Table 1). Consistently, previous clinical studies have shown that SRC is associated with a greater prevalence of hypertension [17]. Although we found that hypertension is not an independent predictor of ARAEs, the subgroup analysis showed that patients with SRC and hypertension led to the highest risk of rupture after TEVAR (Table 4). The attenuation of the power to detect a direct association between hypertension and ARAEs may also result from relatively small sample (n = 214) after matching. Recently, Lu et al. [4] found that lower diastolic blood pressure at admission could predict ARAEs in BAD patients after TEVAR, which emphasized the important role of hemodynamic stability in aortic remodeling. Whether hypertensive patients with SRC suffer from severer blood pressure fluctuation than that without after onset of BAD warrants further study.
Contrary to the previous belief that SRC is a benign disease, an increasing body of evidence suggests that patients with SRC experience a higher risk of long-term ARAEs after TEVAR [3, 4]. What’s more, no difference in 5-year all-cause mortality or cardiovascular events (shown in Supplementary Figs. 5,6) was found between the two groups, implying that SRC might play an exclusive role in the adverse aortic remodeling after TEVAR.
We noticed that the difference of ARAEs between the two groups was mostly accumulated in the first 2 years (Fig. 2). Therefore, a landmark analysis was performed by dividing the 5-year follow-up into the first two years and the remaining three years. Results indicated that during the first two years, patients with SRC were at a higher risk of ARAEs (HR: 1.93, 95% CI: 1.17–3.19, p = 0.009). However, for the remaining three years, the cumulative hazard ratios in the two groups were similar (HR: 1.02, 95% CI: 0.37–2.82, p = 0.97). One explanation for this trend is that the patients initially without SRC could have developed new cysts, increasing the probability of ARAEs at follow-up. Another explanation is that all patients receiving TEVAR could benefit from positive aortic remodeling in the long term, irrespective of the presence of SRC [18]. In any case, further studies should be conducted to identify the role of SRC on long-term patient outcomes.
According to current clinical and laboratory evidence, there are several possible underlying correlations between SRC and BAD.
First, both SRC and BAD are related to increased matrix metalloproteinases (MMPs). It has been established that the structural integrity of the aorta depends on the expression of extracellular matrix (ECM) proteins, which are regulated by proteolytic enzymes. Zhang et al. [19] found that MMP-1, MMP-9, and active MMP-9 levels were higher in aortic dissection tissue than control tissue. Interestingly, MMP overexpression and an elevated ratio of MMPs to tissue inhibitors of metalloproteinases (TIMPs) in aortic tissue could induce the degradation of multiple components in the ECM, making the blood vessel more vulnerable to adverse clinical events [20]. Similarly, Harada et al. [21] found massive accumulation of MMP-2 and MMP-9 in human benign cystic fluids. Obermuller et al. [22] found the upregulation of MMP-14 in a rat model of autosomal-dominant polycystic kidney disease and advocated that TIMPs are promising biomarkers for treating polycystic kidney. In summary, the imbalance of MMPs and TIMPs may persist in patients with SRC and BAD, making them susceptible to ARAEs after TEVAR.
Moreover, our study indicated that the patients with SRC had a greater aortic calcification prevalence than the non-SRC group in the total population. It has been established that multiple factors can affect arterial calcification, including calcium and phosphorus imbalances [23]. Calcium ions are key mediators that regulate inflammation, apoptosis and calcification in vascular smooth muscle cells (VSMC) [24]. Consistently, decreased calcium concentration has been documented in AD patients [25], which could be attributed to calcium loss resulting from the administration of diuretics for blood pressure control [26]. Interestingly, clinical studies demonstrated that -antagonists were related to the enlargement of simple renal cysts [27]. Clinically, calcification-induced degradation presents a reduction in stiffness of the aortic wall [23]. This degradation, coupled with the significant tension caused by calcification, results in a remarkable increase in stress around the non-calcified aortic tissue, ultimately putting the aorta at high risk of rupture. Disorders of calcium metabolism and aortic calcification may lead to chronic inflammation of the arterial wall and the formation of residual thrombosis [28], consistent with our findings.
Overall, the results of our study suggested that SRC may be an independent high-risk predictor of long-term ARAEs in BAD patients after TEVAR. According to our findings, BAD patients with SRC should be followed-up by CTA at 1-month, 1-year and 2-year follow-ups and blood pressure should be closely monitored within two years after TEVAR. Annual CTA follow-up and routine blood pressure monitor should be recommended in patients with SRC, two years after TEVAR.
5. Limitation
Due to the retrospective design of our study, it was impossible to randomly allocate the patients.
6. Conclusions
Compared with the non-SRC group, BAD patients with SRC experienced a higher risk of long-term ARAEs after TEVAR. Subgroup analysis showed that the presence of SRC and hypertension led to the highest risk of rupture after TEVAR.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Erbel R Aboyans V Boileau C Boileau C Bossone E Di Bartolomeo R et al 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: Document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC) European Heart Journal 201435287329262517334010.1093/eurheartj/ehu 281 · doi ↗ · pubmed ↗
- 2Zhang L Zhao Z Chen Y Sun Y Bao J Jing Z et al Reintervention after endovascular repair for aortic dissection: a systematic review and meta-analysis The Journal of Thoracic and Cardiovascular Surgery 201615212791288 e 32745355610.1016/j.jtcvs.2016.06.027 · doi ↗ · pubmed ↗
- 3Nishibe T Dardik A Koizumi J Kano M Akiyama S Iwahashi T et al Simple renal cyst and its association with sac shrinkage after endovascular aneurysm repair for abdominal aortic aneurysms Journal of Vascular Surgery 20197118901898 e 13178428110.1016/j.jvs.2019.05.073 · doi ↗ · pubmed ↗
- 4Lu N Hu P Wang J Yan W He Z Xu T et al Simple Renal Cysts are Associated with 24-Month Prognosis of Patients with Type B Aortic Dissection and Hypertension Canadian Journal of Cardiology 201935149915043160467210.1016/j.cjca.2019.07.631 · doi ↗ · pubmed ↗
- 5Zhang L Lu Q Zhu H Jing Z Branch stent-grafting for endovascular repair of chronic aortic arch dissection The Journal of Thoracic and Cardiovascular Surgery 20211621222 e 13192669710.1016/j.jtcvs.2019.10.184 · doi ↗ · pubmed ↗
- 6Zhang R Zhou J Feng J Zhao Z Liu J Li Z et al Inducing false lumen thrombosis for retrograde type a aortic dissection The Journal of Thoracic and Cardiovascular Surgery 201715357652775157910.1016/j.jtcvs.2016.09.022 · doi ↗ · pubmed ↗
- 7Xiang D Wu F Chen L Liang H Xiong B Liang B et al Timing of endovascular repair impacts long-term outcomes of uncomplicated acute type B aortic dissection European Journal of Vascular and Endovascular Surgery 202163 e 54e 5510.1016/j.jvs.2021.09.01734592378 · doi ↗ · pubmed ↗
- 8Lombardi JV Hughes GC Appoo JJ Bavaria JE Beck AW Cambria RP et al Society for Vascular Surgery (SVS) and Society of Thoracic Surgeons (STS) reporting standards for type B aortic dissections Journal of Vascular Surgery 2020717237473200105810.1016/j.jvs.2019.11.013 · doi ↗ · pubmed ↗