When “Myeloma” is not a Myeloma: a case report of malignant bone lymphoma
José Guilherme Freitas, Teresa Ribeiro, Cláudia Moreira, Ilídia Moreira, José Mário Mariz

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
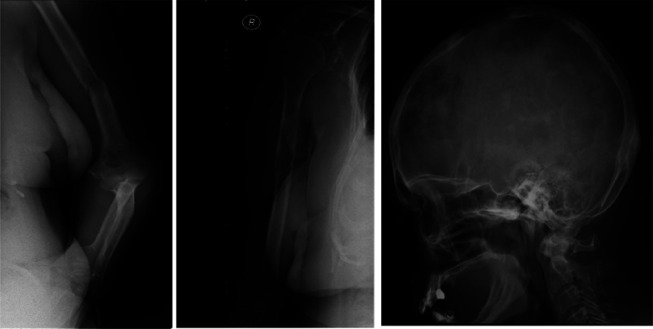 Figure 1
Figure 1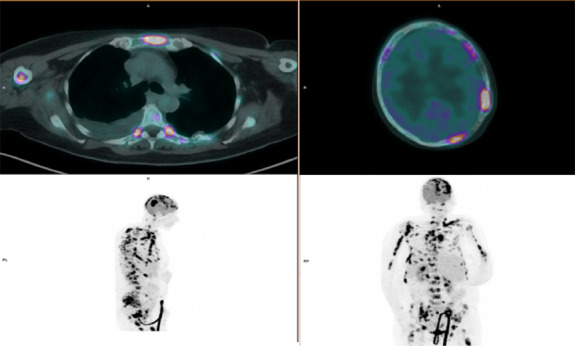 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMultiple Myeloma Research and Treatments · Lymphoma Diagnosis and Treatment · Sarcoma Diagnosis and Treatment
Malignant bone lymphoma (MBL) is a rare entity and is subdivided into primary (PBL) and secondary (SBL) subtypes.^1,2^ PBL accounts for 5% of MBL and presents as unifocal lesion (uPBL) with or without lymph node involvement or as multifocal disease (mPBL), also known as “multifocal osteolymphoma” or “polyostotic lymphoma.”^3,4^ SBL, defined by disseminated lymphoma with bone involvement, is much more common than PBL, accounting for 15% of cases.^2,5,6^ The median age at diagnosis varies between 40 and 60 years with a slight male predominance, diffuse large B-cell lymphoma (DLBCL) being the most common histological subtype (70–80% of cases).^3,7^
Patients may present with bone pain or tumor mass, the long bones, such as the femur and humerus, being the most commonly affected, whereas pathological fracture is the most frequent complication at diagnosis.^1,7–9^ Patients with PBL are staged according to the Ann Arbor system, although the International Extranodal Lymphoma Study Group (IELSG) developed an adapted staging system. PBL presenting as uPBL is classified as stage-IE in Ann Arbor and IELSG systems and mPBL as stage IV in Ann Arbor and IVE in IELSG system.^6^
Primary bone DLBCL should be treated with an anthracycline-containing chemotherapy, rituximab plus cyclophosphamide, doxorubicin, vincristine and prednisone (R-CHOP) with radiotherapy being the standard treatment approach.^10,11^ The overall response rate is over 90% and 5-year overall survival 80–90%,^7,12,13^ over 70–80% being for localized disease, less than 40% for stage IV, and even less for SBL.^6^ Older patients, pathologic bone fracture as the initial presentation, and a high International Prognostic Index (IPI) score portray poorer outcomes,^12^ although the role of IPI score as prognostic factor is controversial.^12,14^ Another issue to be considered is the role of bisphosphonates as their use on PBL is still not established.^15,16^
Most of the literature is exclusively based on small retrospective series and case reports, so biological, clinical, and therapeutic questions remain open to discussion.^3^ We describe a case of a patient presented with bone fractures and lytic lesions resembling multiple myeloma (MM).
A 63-year-old woman presented with a medical history of cirrhosis, diabetes mellitus, fibromyalgia, and acute myeloblastic leukemia (AML), French-American-British classification M2, diagnosed at 2000 and treated with a standard “7+3” regimen plus consolidation with high-dose cytarabine. Afterward, she had secondary cytopenias (neutropenia and thrombocytopenia) due to previous AML treatment, portal hypertension, and cirrhosis.
The patient presented in our emergency department with generalized pain, fatigue, anorexia, and weight loss and a pathologic bone fracture in the right clavicle and left humerus in the previous month (Fig. 1). The physical examination did not reveal any palpable hepatosplenomegaly or lymphadenopathy. Blood tests showed a hemoglobin of 10.6 g/dL, white blood cell count 1.74 × 10^9^/L (neutrophil 0.82 × 10^9^/L; lymphocyte 0.31 × 10^9^/L), and platelet count (93 × 10^9^/L). Biochemistry did not reveal any hepatic or renal dysfunction; albumin was 3.2 g/dL [VR 3.8–5.3], lactate dehydrogenase 472 U/L [RV 67–248], and no hypercalcemia, hyperuricemia, or beta-2 microglobulin elevation. Serum quantitative immunoglobulins, serum protein, and 24-hour urine immunoelectrophoresis were normal. Skeleton X-ray showed osteolytic lesions on the right humerus and skull and bone fracture of the left humerus (Fig. 1), and a spine CT showed osteolytic lesions and compressive fractures at D7-D8. A PET-CT scan showed bone lesions with high avidity for 18F-FDG and low metabolism in the left cervical lymph node and right lower lobe (Fig. 2). Bone marrow aspirate and biopsy did not reveal plasma cell or lymphoid disorder. A bone biopsy of the manubrium revealed a diffuse infiltration of medium/large-sized lymphoid cells (CD10^+^, CD20^+^, BCL2+, BCL6+, MUM1+, CD3^−^, CD5^−^, CD34^−^, CD68^−^, and MPO-), and a pleural effusion immunophenotyping (IFT) revealed involvement by large B-cell lymphoma. The diagnosis of mPBL/SBL DLBCL, germinal center phenotype, stage IV Ann Arbor and IVE IELSG, IPI score 5, was established. The patient was proposed to undergo immunochemotherapy (R-CHOP protocol) and bisphosphonates (zoledronic acid), but due to clinical and analytical worsening after the first cycle (ECOG status [PS > 2], CTCAE grade 3-4 liver, and hematological toxicities), the treatment was suspended and the patient was referred to the palliative unit for best supportive care. At present, she recovered from toxicities and remains with a good symptomatic control.
Criteria to define PBL is still in debate, and the last version of the World Health Organization (WHO) classification does not provide a clearly diagnostic definition of uPBL and mPBL.^5^ Patients with PBL are characterized generally by a localized bone pain. Our patient presented with a generalized bone pain, documented as multiple lytic lesions in PET/CT scan. In such cases, the differential diagnosis for lytic lesions is broad, such as multiple myeloma, osteoblastoma, primary/secondary bone lymphoma, eosinophilic granuloma, infection (osteomyelitis), hyperparathyroidism, metastasis (sarcoma, neuroblastoma), and Ewing sarcoma, among others.^17^ A bone lymphoma diagnosis is performed by histopathological examination, immunohistochemical staining, and molecular analyses,^18^ and PET-CT is a standard tool for staging and response assessment for FDG-avid lymphomas, although this has not been established in PBL.^19^
The clinical presentation in our case might suggest a plasma cell disorder due to the presence of one of CRAB criteria (bone lytic lesions), but the absence of monoclonal plasma cells in bone marrow aspirate ruled out MM. Bone DLBCL diagnosis was confirmed by biopsy, and a PET-CT scan revealed an extensive hypermetabolic bone malignancy involvement and lower metabolism at the left cervical lymph node and right lower lobe. Pleural effusion immunophenotyping revealed involvement by large B-cell lymphoma, raising the following question: Are we facing SBL with an extensive bone involvement or mPBL with lymph node and lung involvement? Our opinion is that, although it has been documented an extranodal (lung) by IFT and lymph node (not proven by biopsy) involvement, due to the discrepancy of extensive bone and nodal involvement, we classify this case as mPBL. The literature is scarce about this issue. Huanwen Wu et colleagues^2^ evaluated patient characteristics and survival and prognostic factors in uPBL, mPBL, and SBL and showed that patients with mPBL and SBL share similar clinical (higher frequency of B symptoms, lymph node, and bone marrow involvement) and demographic characteristics and treatment outcomes compared with those with uPBL, suggesting that patients with mPBL should be better classified and treated as SBL.^2^
This case illustrates a rare presentation of DLBCL as bone lymphoma and raises the question as mentioned before: classify this case as mPBL or SBL? In mPBL, especially in those with regional lymph node and/or adjacent soft-tissue involvement, it may be impossible clinically and radiologically to distinguish from SBL, and this issue remains controversial throughout the literature. Better clarification of the diagnostic criteria and prospective studies are necessary to distinguish these two entities.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gianelli U Patriarca C Moro A . Lymphomas of the bone: a pathological and clinical study of 54 cases. Int J Surg Pathol. 2002;10:257–66.12490975 10.1177/106689690201000403 · doi ↗ · pubmed ↗
- 2Wu H Bui MM Leston DG . Clinical characteristics and prognostic factors of bone lymphomas: focus on the clinical significance of multifocal bone involvement by primary bone large B-cell lymphomas. BMC Cancer. 2014;14:900.25465716 10.1186/1471-2407-14-900PMC 4265495 · doi ↗ · pubmed ↗
- 3Kaiafa G Didangelos T Bobos M . Primary bone diffuse large B-cell lymphoma with multifocal osteolytic lesions: a rare entity. Gen Med Open Access. 2018;6. doi: 10.4172/2327-5146.1000308. · doi ↗
- 4Heyning FH Hogendoorn PCW Kramer MHH . Primary non-Hodgkin’s lymphoma of bone: a clinicopathological investigation of 60 cases. Leukemia. 1999;13:2094–8.10602434 10.1038/sj.leu.2401582 · doi ↗ · pubmed ↗
- 5Fletcher C. World Health Organization, International Agency for Research on Cancer. WHO Classification of Tumours of Soft Tissue and Bone. Lyon, France: International Agency for Research on Cancer; 2013.
- 6Messina C Christie D Zucca E Gospodarowicz M Ferreri AJM. Primary and secondary bone lymphomas. Cancer Treat Rev. 2015;41:235–46.25698636 10.1016/j.ctrv.2015.02.001 · doi ↗ · pubmed ↗
- 7Ramadan KM Shenkier T Sehn LH Gascoyne RD Connors JM. A clinicopathological retrospective study of 131 patients with primary bone lymphoma: a population-based study of successively treated cohorts from the British Columbia Cancer Agency. Ann Oncol. 2007;18:129–35.17018705 10.1093/annonc/mdl 329 · doi ↗ · pubmed ↗
- 8Jawad MU Schneiderbauer MM Min ES Cheung MC Koniaris LG Scully SP. Primary lymphoma of bone in adult patients. Cancer. 2010;116:871–9.20043324 10.1002/cncr.24828 · doi ↗ · pubmed ↗