Obesity-related pubis lymphedema enclosing genitalia: An atypical case of genital reconstruction
Daniel-Adrien Wurlod, Joachim Meuli, Anne Favre-Bulle, Nuno Grilo, Pietro G. di Summa

TL;DR
A rare case of severe lymphedema in the genital area of an obese patient is described, with successful surgical removal of a 7.5 kg mass.
Contribution
This paper presents a novel clinical case of massive scrotal lymphedema in a patient with morbid obesity and hypogonadism-obesity syndrome.
Findings
A 37-year-old patient with a BMI of 68.8 kg/m2 had a 7.5 kg scrotal lymphedema mass removed.
The surgery was performed with minor complications and no additional procedures were needed.
Malignancy was ruled out prior to the surgical intervention.
Abstract
Massive localized lymphoedema (MLL) is a rare complication of morbid obesity and has been scarcely reported in the literature, especially in the pubic area and genitalia. It is associated to BMI more than 40 kg/m2. We report the case of a 37-year-old patient known for morbid obesity with 68.8 kg/m2 BMI and hypogonadism-obesity syndrome presenting an unusually voluminous scrotal MLL mass. Malignancy was ruled out before surgery. In total a 7.5 kg scrotal mass was resected. Surgery was performed with minor complications without requiring additional surgery.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
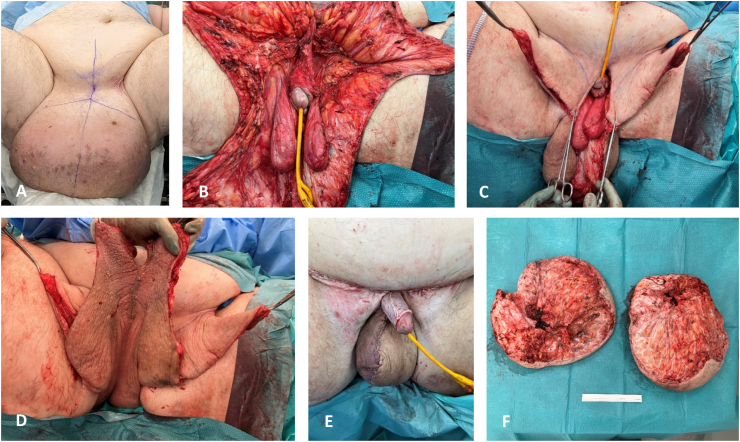 Figure 1
Figure 1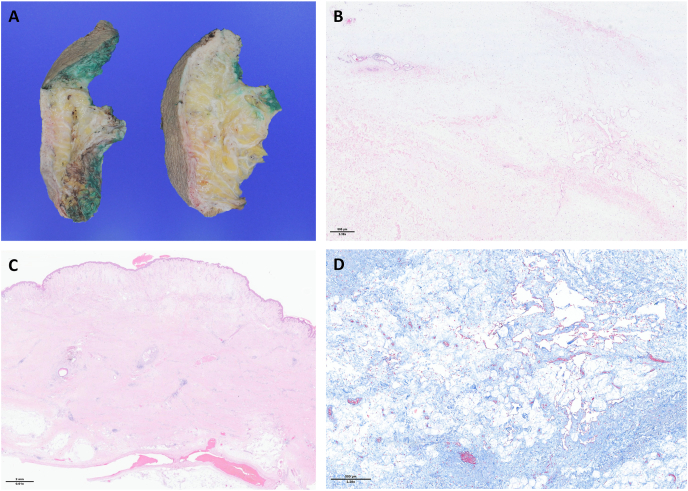 Figure 2
Figure 2 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Tumors and Angiosarcomas · Cardiovascular Effects of Exercise · Muscle and Compartmental Disorders
Introduction
1
Massive localized lymphedema (MLL) has been scarcely reported in the literature, especially in the pubic area and genitalia, and is associated with morbid obesity and BMI >40 kg/m^2^. Reconstruction in the genital area is challenging as failure can lead to infertility. We report the case of a 37 years old patient known for morbid obesity with 68.8 kg/m^2^ BMI and hypogonadism-obesity syndrome presenting an unusually voluminous scrotal MLL mass.
Case Presentation
2
Patient is a 37-year-old male with morbid obesity and BMI of 68.8 kg/m^2^, pre-diabetes, severe obstructive sleep apnea syndrome and hypertension, presenting a growing voluminous scrotal mass over 4 years. Patient's quality of life was severely impacted by his obesity and the scrotal mass, impairing his mobility and spending most of his time in bed. Patient suffered from social withdrawal, explaining the absence of prior investigation.
Initial work-up was made through an abdominopelvic angio-CT scanner showing a voluminous pubic mass enclosing the scrotum of 27 × 35 × 26 cm with adipose density, infiltration of tissue and cutaneous enlargement, along with bilateral inguinal adenomegalies of reactional aspect. Hydrocele or inguinal hernia were ruled out. Needle-biopsies were conducted and showed a fibroadipous and vascular tissue in small abundance with no signs of malignity.
Surgery was decided, planning for a penile and testicles’ excavation with in toto excision of the pubic and scrotal mass. Important lymphatic oozing was observed during dissection. After resection, residual scrotal skin had insufficient vascularization for total scrotal reconstruction. Right half of scrotum was reconstructed with well vascularized scrotal adipocutaneous flap, left half was reconstructed with random freestyle local skin flap of left thigh. Care was taken to keep the available cutaneous perforators included in the flap. Penis shaft was reconstructed with split-thickness skin graft. Mini abdominoplasty was also performed for pubic excess skin and fat resection. In total a 7.5 kg scrotal mass was resected (see Fig. 1).Fig. 1. Peroperative surgical sequence:A. Preoperative appeareance. B. Resection of massive localized lymphedema masses with liberation of gonades and penis. C. Proximal excess cutaneous flaps. D. Distal excess scrotal cutaneous flap. E. Closure using the flaps, a left thigh cutaneous advancement flap for left scrotal reconstruction, and residual cutaneous scrotal flap for right scrotal reconstruction. F. Resected masses, 7.5 kg in total.Fig. 1
Histopathology showed massive and diffuse lymphedema with discrete acute focal inflammation and rare focal liponecrosis, without signs of malignity and without Mdm2 expression, excluding liposarcoma (see Fig. 2).Fig. 2. Anatomopathology study:A. Macroscopy sampling after formaldehyde fixation. B. Cutaneous nodule (hematoxylin and eosin stains): The cutaneous nodules show a thickened collagenous dermis with dermal chronic inflammatory cell infiltrate and loss of skin appendages. C. Lymphedema (hematoxylin and eosin stains): Lymphatic proliferation with numerous ectatic lymphatic and plexiform vessels within an edematous paucicellular stroma, without atypia. D. Transition area (Masson's Trichrome stains): Masson's Trichrome underlignes the lossely textured collagen within the lymphedema, in contrast to the adjacent thickened dermis, which shows a high collagen density.Fig. 2
Surgery was followed by minor suture dehiscence in 3 areas (scrotal and inguinal), mainly caused by maceration and lymphatic edema, treated with local wound caring without need for additional surgery. No sign of recurrence is noted 1-year post operatively (see Fig. 3).Fig. 31-year post-operative.Keywords Massive Localized Lymphoedema – Obesity – Lymphoedema – Genital reconstruction.Fig. 3
Discussion
3
Massive localized lymphedema is a pseudotumor characterized by lymphedema chronical aspect and features, such as peau d’ orange aspect and skin induration. It is associated to BMI more than 40 kg/m^2^ with average of 60 kg/m2. Legs are predominantly involved but pubic area and genitalia are concerned in 10 % of cases. 1 Histologically it shares similarities to well differentiated liposarcoma, thus the importance of excluding malignity especially liposarcoma before planning excision of such lesion. 2 Exact pathogenesis remains unknown but main hypothesis is local ischemia due to overweight related compression, stimulating production of growth factor-leading to lobular structure hypertrophy and fibrosis. 1^,^3^,^4 Surgery is the sole treatment but is known for frequent post-operative complications and recurrence rate (up to 50 %). 5 Genital reconstruction is challenging, and judging the skin quality and deciding the skin excess usage requires creativity and is of great importance for such cases.
Conclusion
4
Massive localized pubic lymphedema enclosing genitalia has been scarcely reported in the literature, with frequent complications and recurrence rate. We report a successful resection and genital reconstruction of such pathology.
Consent
Patient gave his written consent for usage of picture and clinical data gathered for the present case report.
CRediT authorship contribution statement
Daniel-Adrien Wurlod: Writing – review & editing, Writing – original draft, Validation, Methodology, Formal analysis, Data curation, Conceptualization. Joachim Meuli: Validation, Methodology, Investigation, Data curation. Anne Favre-Bulle: Validation, Data curation. Nuno Grilo: Investigation, Data curation. Pietro G. di Summa: Validation, Supervision, Methodology, Investigation, Data curation, Conceptualization.
Declaration of competing interest
The authors report no conflicts of interest and no conflicts regarding ethics.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chopra K.Tadisina K.K.Brewer M.Holton L.H.Banda A.K.Singh D.P.Massive localized lymphedema revisited: a quickly rising complication of the obesity epidemic Ann Plast Surg 7412015 Jan 12613210.1097/SAP.0b 013e 31828 bb 332PMID: 2372258223722582 · doi ↗ · pubmed ↗
- 2Manduch M.Oliveira A.M.Nascimento A.G.Folpe A.L.Massive localised lymphoedema: a clinicopathological study of 22 cases and review of the literature J Clin Pathol 6292009 Sep 80881110.1136/jcp.2009.066555 PMID: 1973447719734477 · doi ↗ · pubmed ↗
- 3Evans R.J.Scilley C.Massive localized lymphedema: a case series and literature review Fall Can J Plast Surg 1932011 e 30e 31PMID: 22942667; PMCID: PMC 326933822942667 PMC 3269338 · pubmed ↗
- 4Lee S.Han J.S.Ross H.M.Epstein J.I.Massive localized lymphedema of the male external genitalia: a clinicopathologic study of 6 cases Hum Pathol 4422013 Feb 27728110.1016/j.humpath.2012.05.023Epub 2012 Sep 17. PMID: 2299533122995331 · doi ↗ · pubmed ↗
- 5Machol JA 4th Langenstroer P.Sanger J.R.Surgical reduction of scrotal massive localized lymphedema (MLL) in obesity J Plast Reconstr Aesthetic Surg 67122014 Dec 1719172510.1016/j.bjps.2014.07.031Epub 2014 Aug 5. PMID: 2515342525153425 · doi ↗ · pubmed ↗