Evaluation of MMV Pandemic Response Box compounds to identify potent compounds against clinically relevant bacterial and fungal clinical isolates in vitro
Seshan Sivasankar, Appalaraju Boppe, Martin Peter Grobusch, Sankarganesh Jeyaraj

TL;DR
This study tests compounds from the MMV Pandemic Response Box against drug-resistant bacteria and fungi, identifying several effective candidates.
Contribution
The study evaluates MMV Pandemic Box compounds against clinically relevant multidrug-resistant bacterial and fungal isolates, identifying novel potent inhibitors.
Findings
MMV1634390 showed complete bactericidal effect against A. baumannii in a persister assay.
MMV1782110, eberconazole, amorolfine, and luliconazole exhibited potent antifungal activity against MDR fungal species.
Erevacycline and epetraborole inhibited both A. baumannii and P. aeruginosa at 10 μM.
Abstract
Multidrug resistant bacterial and fungal pathogens are resistant to a number of significant front-line drugs, hence, identification of new inhibitory agents to combat them is crucial. In this study, we aim to evaluate the activity of Pandemic Box compounds from Malaria Medicines Venture (MMV) against A. baumannii and P. aeruginosa bacterial, C. auris, C. albicans and A. niger fungal clinical isolates. Isolates were initially screened with 201 antibacterial and 46 antifungal compounds (10 μM) using a microbroth dilution in triplicates to determine MIC. A persister assay was performed for bacterial pathogens. Out of 201 antibacterial compounds, twenty-nine and seven compounds inhibited the growth of A. baumannii and P. aeruginosa at 10 μM, respectively. MMV1580854, MMV1579788, eravacycline and epetraborole inhibited both the bacterial test isolates. In a persister assay, MMV1634390…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
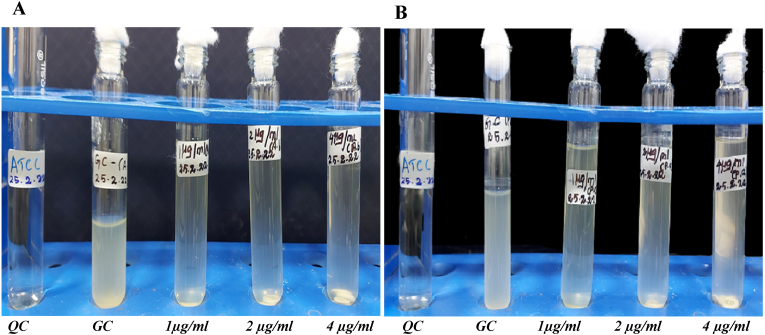 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntifungal resistance and susceptibility · Antibiotic Resistance in Bacteria · Antimicrobial Peptides and Activities
Introduction
1
The slow pace of new antibiotic discovery and the rapid emergence of drug-resistant pathogens imposts a significant burden onto human health. Apart from community-acquired infections, individuals with a compromised immune system, particularly with HIV/AIDS, those with severe burns, patients receiving chemotherapy, and neonates are at higher risk of developing co-morbidities due to bacterial and fungal infections [1,2].
Multidrug-resistant (MDR) A. baumannii and Pseudomonas aeruginosa are the most-common causative agents of infections including bacteraemia, pneumonia, meningitis, and urinary tract infections [3,4]. MDR pathogens are associated with prolonged hospital stays and higher cost alongside with high morbidity and mortality [3,4].A. baumannii and P. aeruginosa are gram-negative non-fermentative bacteria belonging to the Moraellaceae and Pseudomonadaceae families, respectively [3,4]. Both organisms are members of the ESKAPE pathogen family, which poses a serious threat to human health, acquiring antimicrobial resistance at a constant rate [4]. A. baumannii has the ability to survive on dry surfaces, and is partially resilient to disinfectants, constituting a significant cause for nosocomial transmissions [5].A. baumannii and P. aeruginosa are intrinsically resistant to most antibiotics such as fluoroquinolones, tetracyclines, β-lactams, aminoglycosides and carbapenems [4,6]. Concurrently, they emerge as multi- or pan-drug resistant strains; also against colistin, which is being considered the last resort for successful treatment [7]. A number of resistance mechanisms such as target modification, limited permeability of the cell wall, increased activity of efflux pumps and antibiotic hydrolysing enzymes that render antibiotics ineffective have been documented [3,4]. Biofilm formation leads to cross resistance due to low penetration and plays a vital role in the development of preliminary antibiotic resistance mechanisms in A. baumannii and P. aeruginosa [5,8]. The World Health Organization classified carbapenem resistant A. baumannii and carbapenem resistant P. aeruginosa as critical pathogens that require urgent research and development for new drug molecules [9].
Recently, WHO has released a fungal priority pathogen list which include Candida and Aspergillus spp. with a high mortality rate of 40 % [10] and 40–90 % [11],respectively. Candida and Aspergillus species are among the etiological agents causing invasive fungal infections (IFIs) [12]. Although Candida albicans is the major causative agent of invasive candidiasis, other Candida species are also acting as the causative agent of candidiasis, especially C. auris [13].C. auris causes major outbreaks in hospitals and clinical facilities after its first report of an ear infection in Japan 2006. Contrary to C. albicans, C. auris can reside on human skin for weeks, even after treatment and has the ability to survive on external surfaces [14]. According to CDC's 2019 report, C. auris is one among five urgent threats [15]. A. niger is not frequently reported in invasive disease, but it is seen causing otomycosis, cutaneous infections, and pulmonary infections with high fatality [16]. In everyday clinical settings, antifungal susceptibility testing has become a routine diagnostic method mainly due to increasing in vitro resistance of these pathogens [12]. There have been several reports in the recent years describing azole and echinocandin and azole resistant clinical isolates [12]. Pan drug-resistant (PDR) C. auris, resistant to all three classes of antifungals, has also been documented in a number of different countries [17]. To mitigate the emergence and treatment of these fungal pathogens, it is necessary to develop new drugs.
We set out to test the Pandemic Box compounds from Medicines for Malaria Venture (MMV) against multi drug-resistant (MDR) A. baumannii and P. aeruginosa bacterial clinical isolates and C. albicans, C. auris and A. niger MDR fungal clinical isolates. MMV and Drugs for Neglected Diseases initiative (DNDi), in collaboration with scientists in academia, provide open-source drug discovery compounds. Researchers from all over the world have studied the 400 structurally different compounds in the Pandemic Response Box in an effort to combat bacterial, fungal, parasitic and viral pathogens that cause a variety of infectious and neglected tropical diseases [18]. The purpose of this study is to evaluate the inhibitory potential of 201 antibacterial and 46 antifungal compounds from the MMV pandemic box library against the mentioned bacterial and fungal clinical isolates. Persister bacterial cells, that remain dormant during initial antibiotic exposure, were determined after the drug treatment for bacterial samples. Fungicidal concentrations of the drug molecules were assessed.
Materials and methods
2
Bacterial strains and growth conditions
2.1
Colistin-resistant clinical isolates of A. baumannii and P. aeruginosa were collected from the NABL and NABH accredited Microbiology Diagnostic Laboratory of the PSG Institute of Medical Sciences and Research, Coimbatore, India. A. baumannii was isolated from a hemodialysis catheter of the right external jugular vein of a patient with a history of chronic kidney disease. P. aeruginosa was isolated from the abdominal pus of a patient presenting with abdominal abscesses. Catheter and pus swabs were rubbed onto the blood agar and incubated at 37 °C overnight. Following incubation, colonies that emerged were streaked onto MacConkey agar (Himedia, Mumbai, India) plates supplemented with colistin (SRL, Mumbai, India) (4 μg/ml, in accordance with CLSI guidelines) [19]. The colonies were then incubated at 37 °C for 24 h and subsequently stored at 2 °C until needed. Bacteria were initially identified using Biochemical tests andVitek2®GN ID card. Antibiogram testing was performed using Kirby-Bauer method and Vitek2® AST card N280 following CLSI guidelines 2021(BioMérieux, Marcy-l'Étoile, France). The colistin disc broth elution (CDBE) assay was performed to identify resistance amongst test clinical isolates against colistin according to CLSI guidelines. This CBDE assay was performed as previously described by Simner et al., 2023 [20]. Briefly, this assay involves four tubes with colistin discs of 0,1, 2 and 4 μg/ml concentration of colistin, respectively. Fifty μl of the inoculum were added to each tube to obtain a final concentration of 5 × 10^5^ CFU/ml in accordance with CLSI guidelines. The growth of the organisms was assessed visually after incubation. Growth controls consisted of tubes inoculated with test pathogens, while the E. coli ATCC 25922 strain with colistin disc acted as negative control. The MIC of the test strains was determined using commercial MIKROLATEST MIC®-MIC colistin kits (ErbaLachemas.r.o, Brno, and Jihomoravskykraj, Czech Republic). CAMHB was used for the bacterial screening and assays.
Fungal strains and growth conditions
2.2
C. albicans, C. auris and A. niger fungal strains were isolated from patient samples. Germ tube test, lactophenol cotton blue staining methods were used for preliminary identification of the fungal species and were confirmed withVitek2® using YST ID card. Antifungal sensitivity testing was performed using Vitek2®. Candida strains were inoculated into 5 ml YPD media (1 % yeast extract; 2 % peptone; 2 % dextrose; 0.5 % ammonium sulphate) and incubated overnight at 35 °C (150 rpm) prior to use. Fresh A. niger culture on Sabouraud dextrose agar (SDA) slant (Himedia, Mumbai, India) was used for the assay. YPD was used for all fungal screening assays such as preliminary screening, MIC, and MFC determination assays.
DNA extraction, species confirmation and colistin resistant gene
2.3
Bacterial DNA was extracted using QIAamp DNA Mini kit (Qiagen, Hilden, Germany) following the manufacturer's instructions. The extracted DNA samples were subjected to 16s rRNA gene PCR amplification, and amplicons were visualized with the agarose gel electrophoresis method. Using the Genetic Analyzer 3500, amplified PCR products were sequenced using the Sanger method for species confirmation (Applied Biosystems Hitachi-High-tech, Tokyo, Japan). Chromatogram and raw reads were visualized using Finch TV and subjected to NCBI BLASTn to match the identity. Presence of mcr genes (mcr1 to mcr5) and mgrB gene alteration were detected using PCR and agarose gel electrophoresis methods. Primer sequences were used from the previously reported studies [21].PCR reaction mix consisted of 7.5 μl of Taq DNA polymerase 2x master mix RED (Ampliqon, Denmark), 200 nM of primers, 1 μl of template and nuclease free water to make up 15 μl PCR volume. PCR conditions was set as follows: 3 min of 94 °C initial denaturation, except for mcr2 with 15 min of initial denaturation, 30 cycles of 94 °C for 30 s, 90 s of annealing temperature (mcr1 – 47.9 °C; mcr2 - 56.5 °C; mcr3 - 48.4 °C;mcr4 – 46.8 °C;mcr5 - 49.5 °C; mgrB - 54 °C), and 60 s of 74 °C final elongation followed by termination at 72 °C for 10 min. The amplicons were visualized using agarose gel electrophoresis method using 1.5 % agarose.
MMV pandemic box
2.4
The compounds in the MMV Pandemic Response Box were provided in five 96-well microtiter plates, each plate containing 80 compounds. Initially, each well of the plate contained10μl of a 10 mM compound solution in DMSO. As per MMV instructions, 90 μl of DMSO was added to the 10 mM stock solution to dilute it to 1 mM. The first and last columns in each plate were left empty, reserved for negative and positive controls, respectively [18]. All plates were stored at −20 °C, until use. The structure, IUPAC name and cytotoxicity data of the compounds were provided by MMV (Table .4).
Inhibitory activity screening
2.5
Bacterial cultures and fungal cultures were inoculated into 5 ml of Cation Adjusted Muller Hinton Broth (CAMHB) and YPD media, respectively, followed by incubation at 37 °C overnight with shaking at 150 rpm. The suspension turbidity of overnight culture was adjusted to an optical density of 0.1 ± 0.02 absorbance at 600 nm or 0.5 McFarland scale, which is equivalent to 1.5 × 10^8^ CFU/ml. In case of A. niger, a loopful of conidia was suspended in saline with 1 % Tween-20 and adjusted to 0.5 McFarland. The turbidity-adjusted culture was serially diluted to obtain a 10 × 10^5^ CFU/ml inoculum in corresponding media (M_i_). The inoculum (50 μl) was dispensed into the wells of the 96-well test plate. Three microliters of 1 mM stock compounds (to possess antibacterial activity) were diluted with 147 μl of growth media (M_c_) to a concentration of 20 μM, with 150 μl of compound-broth mixture. Fifty μl of the Pandemic Response Box compounds at a concentration of 20 μM (M_c_) were then dispensed into the wells of 96-well microtiter plates containing 50 μl of 10 × 10^5^ CFU/ml culture (M_i_) (50 μl M_c_+50 μl M_i_), resulting in a final solution with 10 μM concentration of the test compound, 5 × 10^5^ CFU/ml, and 1%DMSO (in triplicates). All the compounds were screened in triplicates. The first and last columns of each plate were representing growth controls (culture without drugs) and blank (only media). The microtiter plates were sealed with optically clear micro sealers and incubated at 37 °C overnight. A. niger assay plates were incubated at 27 °C for 72–96 h, whereas C*. albicans* and C. auris plates were incubated at 35 °C for 24 h. Photometric readings were obtained by using a Varioskan Flash Multimode reader (Thermo Scientific, Waltham, Massachusetts, USA). Optical densities (OD)were recorded at 600 nm wavelength for bacteria and Candida spp. and at 530 nm for Aspergillus spp. The solutions in wells with little or no turbidity were only considered for the persister assay and fungicidal concentration determination. Fluconazole was used as an internal drug control for the preliminary screening against fungal pathogens. The percentage of growth inhibition was calculated using the formula: % of growth inhibition = 100 × [1- (OD_T_ -OD_B_)/(OD_G_-OD_B_)], where OD_T_ was the optical density of wells treated with drug; OD_G_ represented growth control where wells contain no drugs; and OD_B_ denoted the negative control. The compounds that showed inhibition in this screening method were used for further testing including persister assay and MIC determination.
Assessment of bacterial persister frequency
2.6
In order to evaluate the surviving population, liquid culture from wells with little or absence of growth were used for measuring the persister frequency (Pf). Suspensions from the wells were serially diluted up to 10^−3^, and 100 μl of suspension from the final dilution step was spread over the LB agar media and incubated overnight at 37 °C. Manual colony counting was performed to estimate the number of viable bacteria. The persister population was enumerated by calculating CFU with the colony count of each plate in relation to dilution (colony forming unit (CFU) per ml = no. of. colonies × dilution factor × inoculum volume ^−1^).
Minimum inhibitory concentration
2.7
Compounds that inhibited growth of the pathogens in the preliminary screening method were subjected to minimum inhibitory concentration (MIC) determination in sterile polystyrene flat-bottom 96-well plate. The final concentration of compounds in MIC determination ranged from 10 to 0.062 μM using microbroth dilution as mentioned before. Each well had a final cell density of 10^5^ cells/ml, and the plates were incubated at 37 °C for 18–24 h. The least concentration at which fungal growth was inhibited completely (100 %) was defined as MIC.
Fungicidal concentration
2.8
MMV indicated compounds having antifungal activity only were used to determine fungicidal activity. The fungicidal concentration was determined by transferring an aliquot of 5 μl from the wells that showed no visible fungal growth, in triplicates, from the previous MIC determination Microdilution assay plate to antibiotic free SDA plate supplemented with 2 % dextrose. The minimum fungicidal concentration (MFC) was determined as the least concentration with no fungal colonies on SDA plate after incubation. MFC:MIC ratio was determined to evaluate the compounds as fungicidal (1–2) and fungistatic (>2) [22].
Results
3
Antimicrobial susceptibility and molecular analysis
3.1
Turbidity was observed visually in all the tubes containing 0, 1, 2 and 4 μg/ml of final colistin concentration, indicating growth in all tubes (Fig. 1A and B), consistent with CLSI standards. Turbidity was observed for A. baumannii and P. aeruginosa up to 16 and 8 μg/ml, respectively, in the MIC determination assay using the Microlatest® MIC colistin kit (ErbaLachema, Brno, Czech Republic).A. baumannii was found to be resistant to colistin and ceftazidimein the antibiogram tests (Supplementary Table 1). P. aeruginosa isolate was resistant to colistin along with most of the β-lactam antibiotics, but sensitive to aztreonam (Supplementary Table 1). C. auris strain was resistant to amphotericin B and fluconazole, whereas C. albicans was resistant to ketoconazole, fluconazole, clotrimazole (Supplementary Table 2). Sanger sequencing of the 16S region and BLASTn analysis confirmed the clinical isolates as A. baumannii and P. aeruginosa, with 98.7 % and 99.8 % of identity, respectively. mcr1-5genes were found to be absent in both the isolates via PCR method. Test isolates were found to be carrying wild type mgrB gene.Fig. 1. Colistin broth Disk Elution assay with clinical isolatesFour tubes for each bacterial strain containing 10 ml of cation adjusted Muller Hinton Broth that generated a final concentration of 0, 1, 2 and 4 μg/ml colistin, respectively. Fig. 1A represents the test for A. baumannii colistin resistant strains whereas Fig. 1B displays P. aeruginosa growth until 4 μg/ml concentration with ATCC E. coli as quality control QC. GC represents growth control tubes with test isolates without colistin drugs.Fig. 1
Inhibitory activity against bacterial pathogens
3.2
In case of A. baumannii, 29 drugs inhibited 90–100 % of growth; 15 compounds inhibited 70–89 % of growth; 21 compounds showed 50–69 % of inhibition; and 136 drugs had less than 49 % inhibition effect on growth. P. aeruginosa was inhibited actively by a smaller number of drugs, where only seven drugs inhibited the growth completely (90–100 %); two drugs with 70–89 % inhibitory activity; five drugs with 50–69 % of inhibition; and 187 drugs inhibited the growth of target organism less than 49 % (Table 1). More than 75 % of compounds showed less than, or equal to, 50 % growth inhibition at the given concentration onP.aeruginosa.MMV1580854, MMV1579788, MMV1578574 and MMV1578566 compounds showed strong inhibitory activity (∼80 %) against both the strains. The compounds that showed more than 90 % inhibitory action against the pathogens were subjected to persister screening.Table 1. Initial screening of bacterial pathogens and persister cells produced after treatment.Table 1. CompoundA. baumannii**P. aeruginosa% of growth inhibitionPersistercount*% of growth inhibition*PersistercountMMV1582497100.00TNTCMMV158154899.16TNTCMMV1578568100.00TNTC96.661 × 10^−1^ CFU/mlMMV158017393.04TNTCMMV1634390100.00No coloniesMMV158155254.87TNTCMMV158085396.10TNTC60.69TNTCMMV158084150.70TNTCMMV508427100.00TNTCMMV163438376.04TNTCMMV158084856.55TNTCMMV158084070.47TNTCMMV157984697.18TNTCMMV157884297.21TNTCMMV157935479.94TNTCMMV157857196.105.5 × 10^−2^ CFU/mlMMV163396678.55TNTCMMV00245995.543.8 × 10^−2^ CFU/ml100.00TNTCMMV63794559.05TNTCMMV158085496.66TNTC55.27TNTCMMV158085191.09TNTCMMV157984997.77TNTC60.17MMV020752100.00TNTCMMV157857597.21TNTCMMV166345783.84TNTCMMV093250100.00TNTCMMV159354199.162.4 × 10^−2^ CFU/mlMMV159353797.21TNTCMMV158249290.25TNTCMMV158249196.10TNTC60.79TNTCMMV158084490.8TNTCMMV157978884.40TNTC93.95TNTCMMV157978594.43TNTCMMV157855958.22TNTCMMV157857492.20TNTC98.756.3 × 10^−1^ CFU/mlMMV157856692.48TNTC97.081.7 × 10^−2^ CFU/mlMMV178214072.14TNTCMMV163439183.57TNTCMMV163367457.38TNTCMMV159353287.19TNTCMMV63765979.11TNTCMMV157985073.10TNTCMMV37418752.24TNTCMMV68875652.37TNTCMMV157889767.13TNTCMMV00101451.25TNTCMMV157855461.00TNTCMMV163440287.47TNTC79.67TNTCMMV00005176.60TNTCMMV158249667.69TNTCMMV158249098.051.0 × 10^−3^ CFU/mlMMV158248892.48TNTCMMV00266550.42TNTCMMV158155951.81TNTCMMV158154577.16TNTCMMV158085561.56TNTCMMV1580849100.003.5 × 10^−2^ CFU/mlMMV158083965.18TNTCMMV157977853.48TNTCMMV09971448.47TNTCMMV157889153.20TNTCMMV12465650.42TNTCMMV97597255.71TNTCMMV157888497.491.9 × 10^−2^ CFU/mlMMV10846571.59TNTCMMV157857096.669.3 × 10^−2^ CFU/mlMMV157856496.38TNTCMMV178240393.316.1 × 10^−2^ CFU/mlMMV161356354.87TNTCMMV pandemic response box compounds that showed inhibition were mentioned and expressed as percentage (%) of growth inhibition. Percentage of inhibition was calculated using the OD at 600 nm.Persisterfrequencies with respect to each hit compounds against bacterial pathogens arerepresented as CFU/ml (Persister count). * TNTC – too numerous to count.
Bacterial persister frequency
3.3
Plates spread with suspension of the wells with 50 % growth inhibition showed colonies that were too numerous to count (TNTC). Liquid culture of complete inhibition wells of the test organisms when spread on LB agar plates produced countable or lesser numbers of colonies (Table 1). Interestingly, the MMV1634390 compound which showed complete inhibition of A. baumannii in microbroth dilution was found to be bactericidal with zero persisters. The remainder of the hit compounds against A. baumannii were enumerated for persister frequency; as follows, MMV1578571 (5.5 × 10^2^ CFU/ml), MMV002459 (3.8 × 10^2^ CFU/ml), MMV1593541 (2.4 × 10^2^ CFU/ml), MMV1582490 (1.0 × 10^3^ CFU/ml), MMV1580849 (3.58 × 10^2^ CFU/ml), MMV1578884 (1.9 × 10^2^ CFU/ml), MMV1578570 (9.3 × 10^2^ CFU/ml) and MMV1782403 (6.1 × 10^2^ CFU/ml) (Table 1). In case of P. aeruginosa, MMV1578568 which was inhibiting the survival of the pathogen at 100 % produced a persister frequency of 1 × 10^1^ CFU/ml. MMV1578574 and MMV1578566 resulted in 6.3 × 10^1^ CFU/ml and 1.73 × 10^2^ CFU/ml of persister frequency, respectively (Table 1).
Identification of antifungal compounds
3.4
Internal control fluconazole inhibited 99 % growth of Candida and Aspergillus fungal strains. Amongst 46 compounds tested, antifungal activity (defined as more than 90 % growth inhibition) was reached by 15 compounds against Candida auris. These compounds were eberconazole, isavuconazonium, MMV1634386, alexidine, AN-2718, terbinafine, MMV1782110, abafungin, carbendazim, amorolfine, MMV1782212, TSC-INH, MMV1782221, MMV1782218 and olorofim. Six compounds possessed antifungal activity against C. albicans, namely eberconazole (%IG = 98 %), MMV1634386 (%IG = 93 %), ketoconazole (%IG = 94 %), terbinafine (%IG = 95 %), amorolfine (%IG = 92 %) and luliconazole (%IG = 93 %). A. niger was inhibited with 99 % of growth by alexidine in preliminary screening (Table 2).Table 2. Percentage of growth inhibition of fungal pathogens by various compounds with expected antifungal activity of Pandemic Response box.Table 2MMV IDTrivial NameInhibition percentageC.aurisC. albicansA. nigerMMV1634492Eberconazole9398MMV1634494Isavuconazonium98MMV16343869893MMV637533Ketoconazole94MMV002565OxfendazoleMMV396785Alexidine9699MMV1634363AN-271890MMV1634359Terbinafine9895MMV1782110100MMV1634493Abafungin94MMV344625Carbendazim95MMV1634358Amorolfine9292MMV640014DeferasiroxMMV178221290MMV1782227TSC-INH99MMV178222196MMV1782224Luliconazole93MMV1782223MMV178221897MMV1782354Olorofim97Antifungal compounds that inhibited fungal pathogens were expressed with Inhibition percentage individually for fungal pathogens used in the study. Compounds are represented with MMV ID and trivial name.
Minimum inhibitory concentrations
3.5
Drugs like eberconazole, alexidine, AN-2718, carbendazim, amorolfine, MMV1782212, TSC-INH, MMV1782221, MMV1782218 and olorofim exhibited minimum inhibitory concentration of ≥10μMonC.auris. MICs of the compounds such as isavuconazonium (≥0.5 μM), MMV1634386 (≥0.5 μM), terbinafine (≥2 μM), MMV1782110 (≥1 μM) and abafungin (≥3 μM) that inhibited C. auris in initial screening were reasonable. C. albicans was inhibited by eberconazole, terbinafine and amorolfine at a minimum concentration of ≥ 2 μM. Lowest MIC was exhibited against C. albicans by MMV1634386 (≥0.2 μM) and ketoconazole (≥0.5 μM) where, luliconazole (≥3 μM) exhibited highest MIC value. Alexidine showed 3 μM of minimum inhibitory concentration on A. niger (Table 3).Table 3. Minimum inhibitory concentration and Minimum fungicidal concentration of antifungal compounds calculated for MIC:MFC ratio.Table 3MMV IDTrivial nameC.aurisC. albicansA. nigerMICMFCMFC:MICMICMFCMFC:MICMICMFCMFC:MICMMV1634492Eberconazole≥10>10≥1≥2≥42MMV1634494Isavuconazonium≥0.5≥48MMV1634386≥0.5≥24≥0.2≥416MMV637533Ketoconazole≥0.5≥520MMV002565OxfendazoleMMV396785Alexidine≥10>10≥1≥3>10≥3.3MMV1634363AN-2718≥10>10≥1MMV1634359Terbinafine≥2≥52.5≥2≥52.5MMV1782110≥1≥22MMV1634493Abafungin≥3≥82.6MMV344625Carbendazim≥10>10≥1MMV1634358Amorolfine≥10>10≥1≥2≥42MMV640014DeferasiroxMMV1782212≥10>10≥1MMV1782227TSC-INH≥10>10≥1MMV1782221≥10>10≥1MMV1782224Luliconazole≥4≥82MMV1782223MMV1782218≥10>10≥1MMV1782354Olorofim≥10>10≥1Minimum inhibitory concentration (MIC) and Minimum fungicidal Concentration (MFC) were denoted as concentration in μM. MIC and MFC ratio (MIC:MFC) values were interpreted as compounds exhibited MIC:MFC ratio of 1–2 were considered as fungicidal and more than 2 as fungistatic. Compounds that exhibited MIC or MFC of more than 10 μM were not considered as potent drug although some demonstrated MIC:MFC ratio of 1.Table 4. Characteristics of pandemic response box compounds showing inhibition against both bacterial and fungal pathogens.Table 4. Compound IDTrivial nameIUPAC nameStructureCytotoxicityCell survival at100μMMWMMV1578574Eravacycline(4S,4aS,5aR,12aR)-4-(dimethylamino)-7-fluoro-1,10,11,12a-tetrahydroxy-3,12-dioxo-9-[(2-pyrrolidin-1-ylacetyl)amino]-4a,5,5a,6-tetrahydro-4H-tetracene-2-carboxamideImage 173 %631.52MMV1578566Epetraborole3-[[(3S)-3-(aminomethyl)-1-hydroxy-3H-2,1-benzoxaborol-7-yl]oxy]propan-1-olImage 290 %273.56MMV1634390methyl N-[[3-(ethylcarbamoylamino)-5-(2-methylpyridin-4-yl)isoquinolin-8-yl]methyl]carbamateImage 368 %393.4MMV1578568Gepotidacin3-[[4-(3,4-dihydro-2H-pyrano[2,3-c]pyridin-6-ylmethylamino)piperidin-1-yl]methyl]-1,4,7-triazatricyclo[6.3.1.04,12]dodeca-6,8(12),9-triene-5,11-dioneImage 496 %448.5MMV1634386(2R)-2-(2,4-difluorophenyl)-1,1-difluoro-3-(tetrazol-1-yl)-1-[5-[4-(2,2,2-trifluoroethoxy)phenyl]pyridin-2-yl]propan-2-olImage 53 %527.4MMV1634359Terbinafine(E)-N,6,6-trimethyl-N-(naphthalen-1-ylmethyl)hept-2-en-4-yn-1-amineImage 637 %327.86MMV396785Alexidine1-(2-ethylhexyl)-3-[N-[6-[[N-[N-(2-ethylhexyl)carbamimidoyl]carbamimidoyl]amino]hexyl]carbamimidoyl]guanidineImage 71 %581.72Compounds ID, Trivial name, IUPAC name, Structure, cytotoxicity and Molecular weight were provided by the MMV. Cytotoxicity values represent the viable percentage of the mammalian cells at 100 μM drug concentration. *MW- molecular weight.
Fungicidal concentration
3.6
Most compounds did not inhibit the growth of the C. auris in subsequent plating on SDA up to 10 μM concentration. These compounds were eberconazole, alexidine, AN-2718, carbendazim, amorolfine, MMV1782212, TSC-INH, MMV1782221,MMV1782218 and olorofim. However, few compounds inhibited C. auris on subsequent plating such as isavuconazonium (≥4 μM), MMV1634386 (≥2 μM), terbinafine (≥5 μM), MMV1782110 (≥2 μM) and abafungin (≥8 μM). Compounds like eberconazole, MMV1634386 and amorolfine produced no visible colonies of C. albicans in antibiotic free SDA plates from 4μMconcentration. Ketoconazole and terbinafine showed fungicidal effect against C. albicans at a concentration 5 μM.Luliconazole exhibited highest MFC of 8 μM. No fungicidal activity was observed in case of A. niger, up to 10 μM concentration (Table 3).
Mode of antifungal action
3.7
Fungicidal and fungistatic modes of action of the drugs were determined by the MFC:MIC ratio. MMV1782110 showed fungicidal effect on C. auris, and few drugs exhibited fungistatic action towards C. auris such as isavuconazonium, MMV1634386, terbinafine and abafungin. Other compounds that inhibited C. auris exhibited more than, or equal to, 1 MFC:MIC ratio, despite the MIC of the compounds having been >10 μM and >10 μM of MFC, respectively. Eberconazole, amorolfine and luliconazole were potential fungicidal compounds against C. albicans. MMV1634386 and ketoconazole were found to be fungistatic on C. albicans. Alexidine, the only compound that inhibited A. niger, also turned out to be fungistatic (Table 3.). Thus, these compounds were considered as potential compounds in our study.
Discussion
4
MDR Pseudomonas spp. (20.5 %) [23]and Acinetobacter spp. (58.51 %) [24]infections are often associated with high mortality and morbidity in Asia. In India, a retrospective study conducted on bloodstream infections showed that 29.9 % (32/107) of the P. aeruginosa population was MDR, with 68.8 % (22/32) of mortality, whereas MDR A. baumannii resistant to carbapenem was 80.4 % (37/46), with a mortality rate of 67.6 % (25/37) [25]. Candida spp. is the primary causative agent of fungal diseases, while Aspergillus spp. acting as the second most-common cause of hospital acquired fungal infections [26]. However, emergence of resistance to one or more groups of antifungals aggravated the treatment for patients with primary or secondary fungal infections [27]. Factors that incite the discovery of new drugs are: (1) the health sector being in need of new drugs to treat invasive bacterial or fungal pathogens; and (2) the rapid development and spread of resistance among these pathogens. Several research laboratories explored the application of MMV compounds on pathogens causing tuberculosis, schistosomiasis and other parasite diseases [28]. In this study, we screened the 201 antibacterial and 46 antifungal compounds from the MMV Pandemic Response Box to identify novel activity effective against MDR A. baumannii and P. aeruginosa bacterial clinical isolates as well as MDR C. auris, C. albicans and A. niger fungal pathogen isolates from the patients. The drug candidates were designated as potential inhibitory compounds if they showed high percentage of inhibition, low MIC values, ability to reduce persister viability in the assays followed by comparison with cytotoxicity values (provided by MMV). Cytotoxicity values were not considered into account while selecting the compounds for the assays.
In our study, 29 compounds at 10 μM inhibited A. baumannii, with nine of those compounds such as determined to be effective. Samoan et al. screened Pandemic Response Box compounds, too, and identified antibacterial activity against A. baumannii, ATCC strain (19606 and BC-5) at 50 μM [29] and P. aeruginosaPAO1 at 20 μM, respectively [30]. Thirty pandemic response box compounds inhibited ATCC A. baumannii, and eleven compounds inhibited P. aeruginosa PAO1, respectively [29,30]. It should be noted that the compounds, which inhibited the ATCC strain of A. baumannii in a previous study, were not inhibiting the clinical field isolate utilized in the current study [29]. Despite showing robust activity in preliminary testing against both clinical pathogens, twenty compounds failed to reduce the bacterial survival on subsequent plating onto LB agar in the persister assay. The variability of the results observed amongst drug resistant strains and sensitive strains, spotlights the limiting factor on the compound efficacy towards different strains of same bacterial species that could poses pandemic potential.
MMV1634390 (methyl N-[[3-(ethylcarbamoylamino)-5-(2-methylpyridin-4-yl)isoquinolin-8yl[methyl]carbamate) exhibited a complete bactericidal effect against A. baumannii, as evidenced by absence of bacterial colonies in the persister assay. Three compounds, MMV1578568(gepotidacin), MMV1578574 (eravacycline) and MMV1578566 (epetraborole) were found to be effective against P. aeruginosa, with more than 90 % of inhibition producing few persister colonies. Hit compounds in our study such as MMV1578568 (gepotidacin), MMV1578574 (eravacycline) and MMV1578566 (epetraborole) on P. aeruginosa produced a persister frequency of 1–6.3 × 10^1^ ± 10^1^ CFU/ml after compound treatment (Table 1). It is known that A. baumannii and P. aeruginosa pathogens have evolved to persist and develop resistance mechanisms like target modification, increased activity of efflux pumps (RND-type), and porin alterations (Opr) under drug pressure [31]. Gepotidacin (MMV1578568), a novel triazaacenaphthylene class antibiotic that functions as a type IIA topoisomerase inhibitor [32]. Phase II (NCT02045797)clinical trial to assess safety, tolerability and efficacy of gepotidacin in study participants with gram-positive bacteria skin infections has been completed [33].
MMV1580854, MMV1579788, MMV1578574 (eravacycline) and MMV1578566 (epetraborole) (Table 1) exhibited inhibition against both A. baumannii (≥80 % of growth inhibition) and P. aeruginosa (>50 % of growth inhibition). Eravacycline is a broad-spectrum antibiotic that is effective against both aerobic and anaerobic Gram-positive and Gram-negative bacteria. The basic mechanism of action of eravacycline is the blockage of the incorporation of amino acids into the elongating peptide chain by binding with 30S ribosomal subunits, which results in impaired protein synthesis. Similarly to tigecycline, eravacycline is unaffected by the resistance mechanism of bacteria such as acquired efflux systems and ribosomal protection proteins [34]. In our investigation, eravacycline was found to reduce the growth of A. baumannii and P. aeruginosa by 92 % and 98 %, respectively. Even though, eravacycline being immune to the development of resistance among bacterial pathogens, improper usage of these novel drug candidate during field use in real world settings may act as resistance promoting factor and studies necessitating further research. Epetraborole is a novel boron-containing antibiotic that targets leucyl-tRNA synthetase; and is effective against Gram-negative bacteria by evading efflux mechanisms. Epetraborole is found to be active against Gram-negative bacteria including NDM-1, TEM-, OXA-, CTX-, and *KPC-*carbapenemase-producing Enterobacteriacae (K. pneumoniae, E. coli, P. aeruginosa, A. baumannii and P. mirabilis) [35]. In our study, epetraborole inhibited 92 % and 97 % of A. baumannii and P. aeruginosa, respectively. Epetraborole was also found to be a potent inhibitor of Mycobacterium abscessus [36]. Although the mechanism of inhibition of both MMV1580854 and MMV1579788 is unclear, and information regarding the functional properties of the drugs is not readily available, these compounds were active against both clinical pathogens in our study [37,38]. MMV1580854 and MMV1579788 inhibited A. baumannii (96 % and 84 % of inhibition) and P. aeruginosa (53 % and 93 % of inhibition). The cytotoxicity of these compounds was estimated to be reasonable, with a cell survival rate above 70 % for the compounds at 100 μM concentration [18]. The synergistic effects of eravacycline with other drugs like ceftazidime, imepenem and colistin are studied, among which the combination with ceftazidime proved successful against carbapenem resistant A. baumannii isolates [39]. Epetraborole in combination with norvaline improved the treatment efficacy against Mycobacterium spp. [40]. The respective modes of action of these drugs as mentioned in this context were crucial for evaluating the efficacy. While some of the compounds such as epetraborole and eravacycline have broad spectrum activity against the majority of gram-negative bacteria, further research is needed to determine the spectrum range of other MMV pandemic response box compounds.
During initial screening for fungal pathogens, 15 compounds inhibited C. auris, six compounds inhibited C. albicans, and one inhibited A. niger. All the inhibitory compounds were able to produce more than 90 % of growth inhibition of all three fungal strains. Few noteworthy compounds such as isavuconazonium (0.5 μM), MMV1634386 (0.5 μM), terbinafine (2 μM), MMV1782110 (1 μM) and abafungin (3 μM) were found to possess antifungal activity on C. auris at lower MIC. Other compounds that exhibited inhibition of C. auris at minimum inhibitory concentration more or equal to 10 μM were not considered effective antifungal compounds. MFC of these compounds were also more than MIC concentration suggesting higher dosage required. Abovementioned compounds were fungistatic towards C. auris, excluding MMV1782110; with a MFC: MIC ratio of 2, demonstrating fungicidal mode of action. C. albicans responded to the hit compounds at lower MIC. Fungistatic action towards C. albicans was displayed by MMV1634386, ketoconazole and terbinafine, whereas eberconazole, amorolfine and luliconazole exerted fungicidal effects. Alexidine was the only hit compound that demonstrated lower MIC (3 μM) but higher MFC (>10 μM) against A. niger. Oteseconazole and terbinafine were identified to be potential antifungal agents against both Candida species; however, compound MMV1782110 showed better fungicidal efficacy against C. auris. Cytotoxicity of the compounds were already provided by MMV [18].
MMV1634386 or oteseconazole ((2R)-2-(2,4-difluorophenyl)-1,1-difluoro-3-(tetrazol-1-yl)-1-[5-[4-(2,2,2-trifluoroethoxy)phenyl]pyridin-2-yl]propan-2-ol) is an azole that targets 14α demethylase or CYP51. The demethylase enzyme plays an important role in the formation of ergosterol responsible for cell membrane integrity [41]. Oteseconazole demonstrated potent invitro activity against azole resistant Candida species [42]. In a recent phase 3 randomized, double-blind clinical trial, participants having acute vulvovaginal candidiasis (VVC) (n = 219)with recurrence were treated with oteseconazole and compared with fluconazole treated control group. Rate VVC resolution was similar between oteseconazole and fluconazole (93.5 % and 95.8 %). Oteseconazole showed a better result in controlling recurrence by week 50 when compared to fluconazole (5.1 % vs. 42.2 %) [43]. In contrast to previous generations of azoles, oteseconazole has excellent selectivity towards CYP51 and reduced interaction with human cytochrome P450s because of the tetrazole moiety [41], whereas the earlier-generation drugs like ketoconazole and fluconazole have imidazole and triazole moieties that tend to have much higher human cytochrome interaction, resulting in drug-drug interaction [41]. Disadvantage of the drug is the embryo-fetal toxicity affecting the female reproductive potential. The drug was approved in April 2022 by the US Food and Drug Administration (FDA) [41]. In our study, oteseconazole produced inhibition at lower MIC towards test Candida strains.
Terbinafine is an allylamine derivative that targets squalene epoxidase (squalene monooxygenase),involved in the formation of ergosterol (squalene 2,3-epoxidase > lanosterol > ergosterol) in cell wall synthesis of fungi, with short duration of therapy as an advantage [44]. Due to the lipophilic nature of terbinafine, it tends to accumulate in fatty sites like adipose tissue, and nails [45]. Terbinafine in our study manifested fungistatic action on both Candida species although the activity was more towards fungicidal mode based on MFC:MIC ratio.
MMV1782110 or 3-(1,3-benzodioxol-5-yl)-N-[[4-(2-fluorophenyl) phenyl]methyl] propanamide is a novel compound with scanty information available [46]. The compound was subjected to antibacterial activity against P. aeruginosa and E. coli, against which it exhibited a MIC of 20 μM [46]. Alexidine or (1-(2-ethylhexyl)-3-[N-[6-[[N-[N-(2-ethylhexyl)carbamimidoyl] carbamimidoyl]amino] hexyl] carbamimidoyl]guanidine) is an amphipathic bisbiguanide that contains two (2-ethylhexyl)guanide units linked by hexamethylene [47]. Alexidine is an anticancer drug that inhibits mitochondrial phosphatase PTPMT1 in mammalian cells causing mitochondrial apoptosis [48]. It was also reported that alexidine displayed potential activity against clinically significant fluconazole resistant C. albicans, C. glabrata, C. parapsilosis and C. auris. Furthermore, this compound completely inhibited planktonic growth and biofilm formation of the filamentous fungi like A. fumigatus [49]. The compound completely eradicated filament formation of A. niger up from a concentration of 3 μM in our assay.
In this study, some of the antibacterial and antifungal compounds in the study demonstrated potential inhibitory activity against the clinical isolates. However, the efficacy of these compounds against the target pathogens in pre-clinical and clinical models has to be investigated to progress further. Furthermore, it should be taken into consideration that these compounds were not giving the same inhibitory activity against the entire spectrum of strains belonging to the same species. Analyzing each of these substances separately on a wide range of strains from various origins and representing different geographical regions would yield valuable information. Different phases of clinical trials of some compounds were underway to assess the safety, side effects and efficacy in various infections models. With limited data of pharmacokinetics and pharmacodynamics of the potent compounds, more investigation and clinical trials are in demand. Discovery of new drugs with proper stewardship and surveillance on the usage of these drugs, preventing overexploitation, is inevitable to mitigate the drug resistance. Moreover, these pathogens are silent-pandemic pathogens and drug resistance in these pathogens adds more complexity in eliminating these pathogens using individual drug than combination therapies. Screening of MMV novel drugs with existing high end drug molecules could yield valuable information. Drug resistance in pathogens were discovered shortly after the usage first antibiotic and been an unsettling threat ever since, long term sustainability of the new drugs for treatment of these drug resistant pathogens is questionable. This also emphasizes the need for the alternate therapeutic methods, including vaccines, early diagnostics, immune boosters and most importantly non-pharmaceutical interventions, that ensure safe and effective combat strategies against drug resistance.
In conclusion, eravacycline and epetraborole were the two most active broad-spectrum compounds against clinical field isolates of A. baumannii and P. aeruginosa. Phase III (NCT01844856) and phase II (NCT01381549) clinical trials for eravacycline and epetraborole were conducted, respectively [39,40]. Scanty information on two other compounds (MMV1580854 and MMV1579788) might be a limiting factor for understanding the mode of action. Furthermore, enzyme kinetics, pharmacokinetics/pharmacodynamics studies of these two drugs might reveal better insights of the compounds. Similarly, we identified few potent antifungal compounds inhibiting the invasive nosocomial fungal pathogens like Candida spp. and Aspergillus spp. Oteseconazole and terbinafine were effective antifungal candidates for C. albicans and C. auris. Alexidine was able to inhibit A. niger. MMV1782110 showed excellent inhibition of C. auris. The current study emphasizes the importance of drug discovery to mitigate drug resistance and fosters future investigations for alternate approaches.
Funding statement
The study was supported by the Indian Council of Medical Research (ICMR), New Delhi, India, extramural core research grant ID- AMR/ADHOC/242/2020-ECD-II.
CRediT authorship contribution statement
Seshan Sivasankar: Writing – review & editing, Writing – original draft, Methodology. Appalaraju Boppe: Writing – review & editing, Methodology. Martin Peter Grobusch: Writing – review & editing. Sankarganesh Jeyaraj: Writing – review & editing, Methodology, Investigation, Conceptualization.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Murray C.J.L.Ikuta K.S.Sharara F.Swetschinski L.Aguilar G.R.Gray A.Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis Lancet 399202262965510.1016/S 0140-6736(21)02724-035065702 PMC 8841637 · doi ↗ · pubmed ↗
- 2Fisher M.C.Alastruey-Izquierdo A.Berman J.Bicanic T.Bignell E.M.Bowyer P.Tackling the emerging threat of antifungal resistance to human health Nat Rev Microbiol 20202255757110.1038/s 41579-022-00720-135352028 PMC 8962932 · doi ↗ · pubmed ↗
- 3Pang Z.Raudonis R.Glick B.R.Lin T.-J.Cheng Z.Antibiotic resistance in Pseudomonas aeruginosa: mechanisms and alternative therapeutic strategies Biotechnol Adv 37201917719210.1016/j.biotechadv.2018.11.01330500353 · doi ↗ · pubmed ↗
- 4Kyriakidis I.Vasileiou E.Pana Z.D.Tragiannidis A.Acinetobacter baumannii antibiotic resistance mechanisms Pathogens 10202137310.3390/pathogens 1003037333808905 PMC 8003822 · doi ↗ · pubmed ↗
- 5Carvalheira A.Silva J.Teixeira P.Acinetobacter spp. in food and drinking water - a review Food Microbiol 95202110367510.1016/j.fm.2020.10367533397609 · doi ↗ · pubmed ↗
- 6Martis N.Leroy S.Blanc V.Colistin in multi-drug resistant Pseudomonas aeruginosa blood-stream infections: a narrative review for the clinician J Infect 69201411210.1016/j.jinf.2014.03.00124631777 · doi ↗ · pubmed ↗
- 7Lim L.M.Ly N.Anderson D.Yang J.C.Macander L.Jarkowski A.Resurgence of colistin: a review of resistance, toxicity, pharmacodynamics, and dosing Pharmacotherapy 3020101279129110.1592/phco.30.12.127921114395 PMC 4410713 · doi ↗ · pubmed ↗
- 8Azimi L.Lari A.R.Colistin-resistant Pseudomonas aeruginosa clinical strains with defective biofilm formation GMS Hyg Infect Control 142019 Doc 1210.3205/dgkh 00032831728266 PMC 6838732 · doi ↗ · pubmed ↗