Spondylodiscitis Following Perforated Acute Appendicitis: A Case Report
Polina Angelova, Atanas Davarski, Ivo Kehayov, Borislav Kitov

TL;DR
A 15-year-old boy developed spondylodiscitis after perforated appendicitis, requiring surgery and antibiotics to resolve symptoms.
Contribution
This is the third reported case of spondylodiscitis following perforated acute appendicitis, highlighting a rare complication.
Findings
Spondylodiscitis at T12-L1 spinal level occurred two months after perforated appendicitis surgery.
Discectomy, posterior pedicle-screw fixation, and antibiotics resolved the patient's symptoms.
Timely diagnosis and treatment are critical to prevent permanent neurological deficits in such cases.
Abstract
Spondylodiscitis is a multifactorial disease of significant medical and socioeconomic importance, the treatment of which presents a challenge to clinicians and surgeons. Acute appendicitis is a common inflammatory disease in children, with postoperative complications occurring in up to 55% of cases. We present the case of a 15-year-old male with symptoms of severe back pain and fever two months following surgery for perforated appendicitis. The computed tomography (CT) revealed spondylodiscitis of T12-L1 spinal level. Discectomy and posterior pedicle-screw fixation were performed, followed by antibiotic treatment resulted in the resolution of preoperative symptoms. To the best of our knowledge, this is the third case of spondylodiscitis after perforated acute appendicitis in literature. Timely diagnosis and treatment in cases of spondylodiscitis are prerequisites for lowering the rate…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
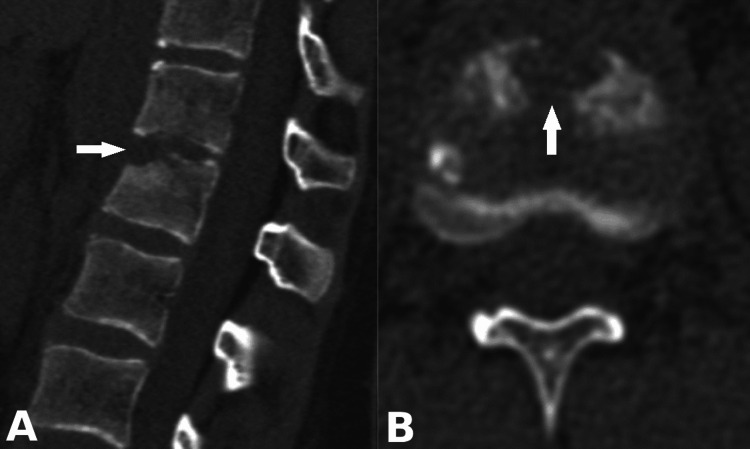 Figure 1
Figure 1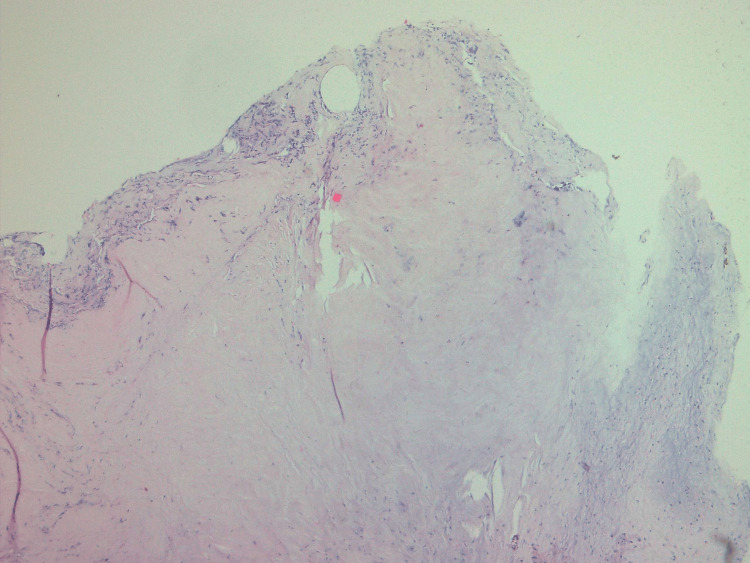 Figure 2
Figure 2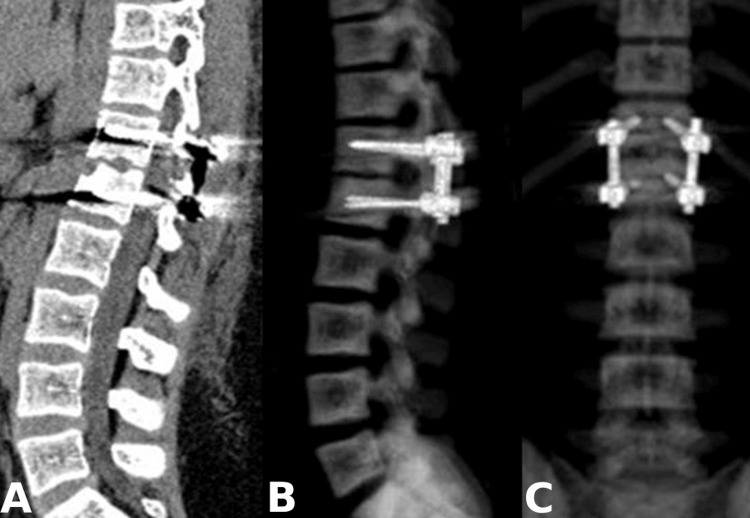 Figure 3
Figure 3| Case | Age | Gender | Location | Type of surgery | Microbiological finding | Conservative treatment |
| Çelik and Can [ | 24 yo | Female | L5-S1 | None | None | Intravenous Ciprofloxacin and Ampicillin sulbactam followed by oral Ciprofloxacin and Sultamicillin |
| AlTarayra et al. [ | 14 yo | Female | L3-L4 | None | Pseudomonas aeruginosa | Intravenous Vancomycin and Ceftazidime followed by Meropenem and Vancomycin |
| Our case | 15 yo | Male | T12-L1 | T12-L1 spinal fusion | Sterile cultures | Intravenous Ceftriaxone and Vancomycin |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfectious Diseases and Tuberculosis · Appendicitis Diagnosis and Management · Diagnosis and treatment of tuberculosis
Introduction
Acute appendicitis is one of the most common causes of emergency abdominal surgery worldwide, with an incidence of 100 per 100,000 people per year. In approximately 29% of cases, appendicitis is perforated [1]. In children, the incidence of perforated appendicitis is about 30%, as it can be much higher in younger children [2]. Morbidity and mortality are significantly higher in cases of perforated appendicitis (16%) in contrast with non-perforated appendicitis (5.6%) [1]. According to Ponsky et al., the risk of abdominal abscess, wound infection, or postoperative ileus is 39% in perforated and 8% in non-perforated appendicitis [3]. Other possible complications, such as enterocutaneous fistula and small bowel obstruction, are also reported [4]. The occurrence of spontaneous spondylodiscitis following surgery for perforated appendicitis in children is an extremely rare complication, and to the best of our knowledge, only two similar cases have been reported in the literature [1,5]. We present a rare case of spontaneous spondylodiscitis following perforated acute appendicitis.
Case presentation
We present the case of a 15-year-old patient with no previous medical history. The patient underwent surgery for purulent perforated appendicitis with local peritonitis. Following the appendectomy, the patient received antibiotic treatment with Amikacin, Meropenem, and Metronidazole for seven days. Two months later he presented with a fever (≥38°C) and severe back pain, which was increasing when standing. The blood pressure, pulse rate, and respiratory rate were normal for age. The symptoms were not relieved by conservative treatment with non-steroid anti-inflammatory drugs. Upon hospital admission, the neurological examination revealed severe back pain. No motor or sensory deficit was established.
Laboratory tests revealed leukocytosis (15.25 x 10^9 g/l), elevated erythrocyte sedimentation rate (47 mm/h), and C-reactive protein (57 mg/l). The thoracolumbar section CT presented the destruction of the lower endplate of T12 and the upper endplate of L1 - a neuroimaging characteristic of spondylodiscitis at the T12-L1 level (Figure 1).
(A) Sagittal and (B) axial preoperative CT images showing the destruction of the lower endplate of T12 and upper endplate of L1 vertebral bodies (arrows)
The neuroimaging data presented involvement of the anterior and middle spinal columns, which suggests future spinal instability. Therefore, the patient was operated on via right interlaminotomy and discectomy of the T12-L1 level. The intervertebral disc showed signs of chronic inflammation, consisting of fragments and bone sequestrations. Given the marked destruction of the T12 and L1 vertebral bodies and aiming to prevent future spinal instability, a short-segment posterior pedicle-screw fixation was subsequently performed (Figure 2). Short-segment fixation was performed considering the age of the patient and possible growth inhibition. The microbiological cultures were sterile. The histological examination revealed a degenerative intravertebral disc with infectious foci (Figure 3).
Histological examination demonstrating degenerative intravertebral disc with infectious foci (HE × 40)
Postoperative CT. (А) Sagittal reconstruction and (B and C) sagittal and coronal 3D-reconstruction showing posterior transpedicular fixation of T12 and L1 vertebral bodies
Following surgery, antibiotic treatment with Ceftriaxone and Vancomycin was administered for two weeks.
The postoperative period was uneventful, with complete resolution of the preoperative symptoms.
Discussion
Spinal infections include discitis, vertebral osteomyelitis, abscess, or spondylodiscitis. In cases of spondylodiscitis, the infection affects both the intervertebral disc and the adjacent vertebral bodies [6]. Spondylodiscitis represents 3-5% of all cases of osteomyelitis with annual incidence from 0.4 to 2.4 cases per 100,000 and a mortality rate reaching 11% [7].
Spondylodiscitis is rarely diagnosed in children with an annual incidence of 0.3 cases per 100,000, accounting for 3% of childhood osteoarticular infections [8]. The peak of the disease is observed at the age of 10-15 years, with a male predominance (m:f = 1.5-2:1) [1].
Pathogens can infect the spine in three ways: a) hematogenous dissemination (arterial or via Batson's venous plexus), b) direct external inoculation, and c) per continuitatem from adjacent affected tissues. Spondylodiscitis most often occurs through hematogenous spread from a distant infectious focus in the body [9]. In children, the arteries of the vertebral bodies have significant anastomoses with the arterial vessels penetrating the intervertebral disc [10]. With age, the disc gradually becomes avascular, and bacterial infection is prone to affect directly the vertebral body [11]. In our case, the infection started at the endplates of the vertebral bodies.
In cases of neurological deficits, spinal instability, bone destruction, or abscess formation, surgical treatment is required. Possible operative interventions for spondylodiscitis in the thoracolumbar region include anterior and posterior surgical approaches. Anterior access provides effective and efficient focal debridement, restoration of spinal stability, bone fusion, neural decompression, and deformity correction [12]. However, it is associated with greater surgical trauma and higher complication rates, such as including vascular and visceral injuries [13]. In recent years, posterior access has been increasingly used in spondylodiscitis in the thoracolumbar segment, including one-stage posterior debridement and instrumentation. The advantages of posterior access in thoracolumbar surgery include familiarity with the approach and widespread use of posterior pedicle screw placement among spinal surgeons [14]. Short and long spinal fusion techniques are almost equally used in cases of spondylodiscitis as long fixation is used more frequently in thoracolumbal junction [15]. In our case, short-segment fixation was performed considering the age of the patient and the possibility of growth inhibition.
There are discussions regarding the risk of implant infection following fusion surgery in cases of spondylodiscitis. Spinal instrumentation is a risk factor for contamination. However, the rate of re-operations due to infection relapse is higher in cases of decompression alone [16].
According to the literature, the most common pathogens causing hematogenous spondylodiscitis in children are Staphylococcus aureus, Streptococcus pyogenes, and Streptococcus pneumoniae. The incidence of sterile microbiological cultures varies from 21% to 41.7% [17,18]. In our case, the difficulty in isolating pathogens is due to the antibiotic therapy carried out following appendicitis surgery. In similar cases, other methods of detecting non-culturable bacteria, such as PCR, should be performed [19].
In the presented case, spondylodiscitis most likely occurred due to transferring the pyogenic microorganisms into the retroperitoneum during the laparotomy, as well as retrograde venous reflux from the pelvis to the paravertebral plexus due to the lack of valves in the draining spinal veins [20]. We present a comparison of our case and two similar cases that have been reported in the literature (Table 1).
Conclusions
Spondylodiscitis remains a severe and disabling spinal disease with a high mortality rate despite advances in surgical and antibiotic treatment. This condition should be considered in cases of children with back pain, radiculopathy, or myelopathy associated with fever and elevated inflammatory markers following acute appendicitis surgery. Prompt diagnosis and treatment are crucial for the outcome and the timely recovery of patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Spondylodiscitis following perforated acute appendicitis in a 14-year-old female: a case report Int J Surg Case Rep Al Tarayra M Abuzaina KN Hassouneh AW Aljabarein OY 1091841152024 https://doi.org/10.1016/j.ijscr.2023.1091843821155410.1016/j.ijscr.2023.109184 PMC 10788785 · doi ↗ · pubmed ↗
- 2Perforation risk in pediatric appendicitis: assessment and management Pediatric Health Med Ther Howell EC Dubina ED Lee SL 13514592018 https://doi.org/10.2147/PHMT.S 155302.3046467710.2147/PHMT.S 155302 PMC 6209076 · doi ↗ · pubmed ↗
- 3Hospital- and patient-level characteristics and the risk of appendiceal rupture and negative appendectomy in children JAMA Ponsky TA Huang ZJ Kittle K Eichelberger MR Gilbert JC Brody F Newman KD 1977198229220041550758310.1001/jama.292.16.1977 · doi ↗ · pubmed ↗
- 4Management of pediatric perforated appendicitis: comparing outcomes using early appendectomy versus solely medical management Pediatr Infect Dis J Bonadio W Rebillot K Ukwuoma O Saracino C Iskhakov A 9379413620172666973910.1097/INF.0000000000001025 · doi ↗ · pubmed ↗
- 5Infectious spondylodiscitis after appendectomy for perforated appendicitis: case report J PMR Sci Çelik C Can Can AGAG 142145202017 https://www.jpmrs.org/current-issue/infectious-spondylodiscitis-after-appendectomy-for-perforated-appendicitis-case-report-633
- 6Infectious discitis and spondylodiscitis in children Int J Mol Sci Principi N Esposito S 5391720162707059910.3390/ijms 17040539 PMC 4848995 · doi ↗ · pubmed ↗
- 7Epidemiological and clinical features of pyogenic spondylodiscitis Eur Rev Med Pharmacol Sci Fantoni M Trecarichi EM Rossi B 2716 Suppl 22012 https://pubmed.ncbi.nlm.nih.gov/22655478/22655478 · pubmed ↗
- 8The etiology, clinical presentation and long-term outcome of spondylodiscitis in children Pediatr Infect Dis J Kang HM Choi EH Lee HJ 0635201610.1097/INF.000000000000104326974751 · doi ↗ · pubmed ↗