The appropriateness of empirical antibiotic therapy in the management of symptomatic urinary tract infection patients—a cross-sectional study in Nairobi County, Kenya
Hellen A Onyango, Derek J Sloan, Katherine Keenan, Mike Kesby, Caroline Ngugi, Humphrey Gitonga, Robert Hammond

TL;DR
This study assesses how well antibiotics prescribed without lab tests treat urinary tract infections in Nairobi, Kenya, finding that less than half of prescriptions matched the bacteria's resistance patterns.
Contribution
The study provides insights into the effectiveness of empirical antibiotic prescriptions for UTIs in a low-resource setting with high antibiotic resistance.
Findings
Only 53% of empirically prescribed antibiotics matched the susceptibility of isolated UTI pathogens.
Fluoroquinolones were the most commonly prescribed antibiotics for UTI patients.
Antimicrobial resistance surveillance is recommended to improve empirical treatment in resource-limited areas.
Abstract
In low- and middle-income countries, symptomatic urinary tract infection (UTI) patients are often prescribed antibiotics without microbiological confirmation. UTIs caused by antibiotic-resistant bacteria are increasingly common, and this heightens the risk of empirical treatment failure. This study evaluates the appropriateness of empirical antibiotic therapy to UTI patients in Nairobi County, Kenya. A hospital-based, cross-sectional study was conducted in Nairobi County, Kenya, amongst symptomatic adult and child patients. UTI was defined as a monoculture growth with colony counts of ≥104 cfu/mL. Antimicrobial susceptibility testing was performed by the Kirby–Bauer disc diffusion method. Empirical therapy was considered appropriate if the pathogen isolated was susceptible to the prescribed antibiotic and inappropriate if the pathogen was resistant to the prescribed antibiotic. A…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1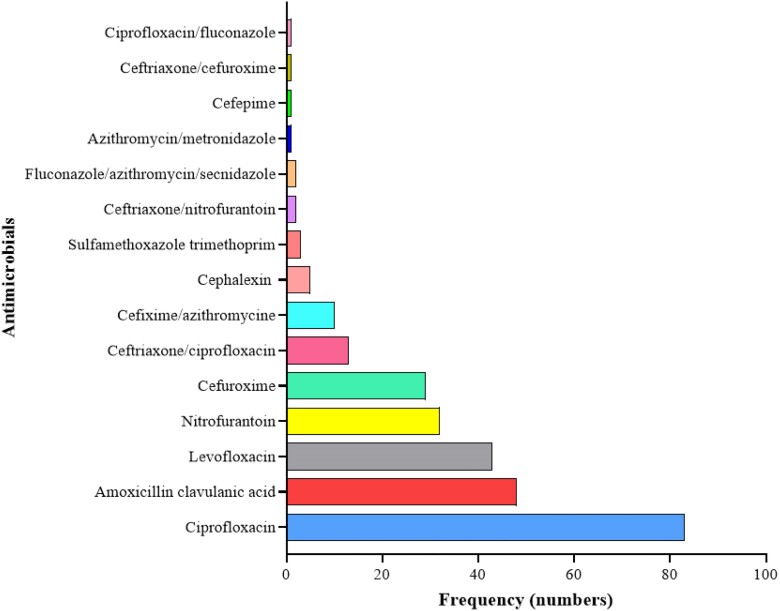 Figure 2
Figure 2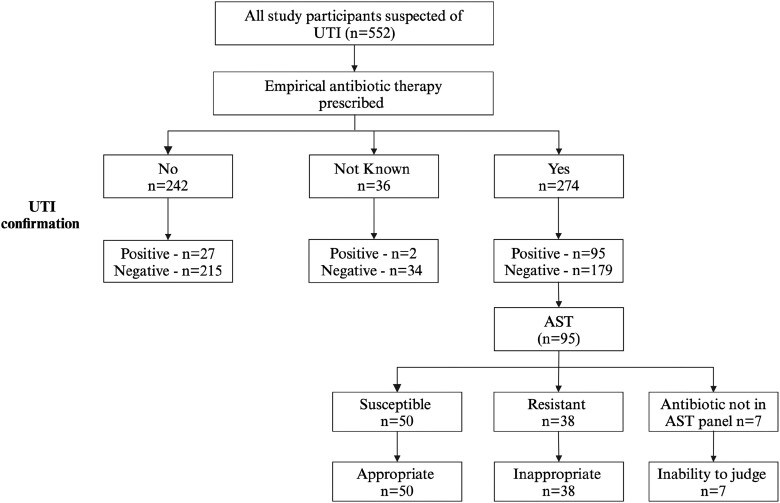 Figure 3
Figure 3| Variable | UTI (+)* | UTI (−)* | |
|---|---|---|---|
| Response |
|
| |
| Average | 124 (22.5) | 428 (77.5) | |
| Gender | Male | 32 (26) | 122 (29) |
| Female | 92 (74) | 306 (71) | |
| Age | 5–10 | 9 (7.2) | 21 (5) |
| 11–20 | 12 (9.6) | 37 (8.6) | |
| 21–30 | 56 (45) | 183 (43) | |
| 31–40 | 25 (20) | 103 (24) | |
| 41–50 | 12 (9.6) | 54 (13) | |
| >50 | 10 (8) | 30 (7) | |
| Medication taken in two weeks prior to recruitment | No medication | 76 (61) | 240 (56) |
| Yes—antibiotics | 37 (30) | 131 (31) | |
| Yes—other medications | 11 (8.8) | 57 (13) |
| Organism groups | No. of organisms tested | AMR, | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
| AMP | AMC | CAZ | CRO | FEP | FOX | GEN | CIP | SXT | NIT | CXM | ERY | LNZ | |
|
| 64 | 53 (83) | 30 (47) | 29 (45) | 33 (52) | 29 (45) | 8 (12) | 15 (22) | 39 (61) | 49 (77) | 3 (5) | 58 (91) | N/A | N/A |
|
| 21 | 20 (95) | 13 (62) | 13 (62) | 14 (67) | 14 (67) | 6 (29) | 7 (33) | 19 (91) | 14 (67) | 10 (48) | 19 (91) | N/A | N/A |
|
| 7 | 4 (57) | 4 (57) | 0 | 0 | 0 | 0 | 1 (14) | 2 (29) | 4 (57) | 7 (100) | 3 (43) | N/A | N/A |
|
| 2 | 2 (100) | 2 (100) | 1 (50) | 1 (50) | 0 | 2 (100) | 0 | 0 | 2 (100) | 2 (100) | 2 (100) | N/A | N/A |
|
| 2 | 1 (50) | 0 | 0 | 1 (50) | 0 | 0 | 0 | 0 | 0 | 1 (50) | 1 (50) | N/A | N/A |
|
| 1 | 1 (100) | 1 (100) | 1 (100) | 1 (100) | 1 (100) | 1 (100) | 1 (100) | 1 (100) | 1 (100) | 1 (100) | 1 (100) | N/A | N/A |
|
| 14 | 12 (86) | 4 (29) | N/A | N/A | N/A | 3 (21) | 3 (21) | 8 (57) | 11 (79) | 1 (7) | N/A | 8 (57) | 0 |
| CoNS | 7 | 7 (100) | 3 (43) | N/A | N/A | N/A | 3 (43) | 1 (14) | 5 (71) | 1 (14) | 1 (14) | N/A | 55 (71) | 0 |
|
| 6 | 0 | 0 | N/A | N/A | N/A | 6 (100) | 6 (100) | 5 (83) | 2 (33) | 1 (17) | N/A | 6 (100) | 0 |
- —Scottish Funding Council10.13039/501100000360
- —Global Challenges Research Fund10.13039/100016270
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrinary Tract Infections Management · Antimicrobial Resistance in Staphylococcus · Bacterial Identification and Susceptibility Testing
Introduction
Antimicrobial resistance (AMR) is the ability of microorganisms to circumvent the toxic action of antimicrobial substances that otherwise would kill or inhibit them.^1^ The prevalence of resistance in common disease-causing bacteria has increased globally, both in healthcare and in community settings.^2^ Consequently, the WHO has now listed AMR as an emerging public health threat believed to account for over 700 000 deaths per year.^3^ The burden of AMR is estimated to be highest in the low- and middle-income countries (LMICs), particularly in Africa,^4^ where morbidity and mortality from infectious diseases are high and health facilities less well-resourced than those in high-income regions.^5,6^ Large regional, interdisciplinary studies, including the Holistic Approach to Unravel Antimicrobial Resistance in East Africa (HATUA) project which was run across Kenya, Uganda and Tanzania, have reported multiple drivers of AMR. Relevant factors ranged from inappropriate antibiotic prescriptions to widespread non-prescription-based dispensing of antimicrobials for self-medication, antibiotic use in animals and environmental factors such as sanitation, as well as social-economic and structural drivers including the cost of seeking healthcare.^7–9^ In hospital settings, factors such as inadequate diagnostic capabilities, poor antibiotic stewardship practices, poor adherence to treatment guidelines and lack of AMR surveillance have been associated with resistance.^6,10^
Urinary tract infections (UTIs) are amongst the most common community-acquired bacterial infections and are the second most frequent clinical indication for antibiotic use^11^ after respiratory infections.^12^ Patients with suspected UTI are often initiated on antibiotic treatment before culture results are available. However, in some cases, approximately 40% of the bacteria that cause UTI are resistant to the antimicrobials prescribed.^13^ In the recent past, the prevalence of multi-drug-resistant bacteria associated with UTI has increased,^14^ making selection of therapy for community-acquired UTI complex. Guidelines for uncomplicated UTI treatment recommend customization of therapy based on local practice, circulating resistant organisms, drug availability and price.^15^ In Nairobi County, Kenya, where this study was undertaken, nitrofurantoin 100 mg, amoxicillin–clavulanic acid 625 mg and amikacin 15–30 mg/kg are the recommended empirical antimicrobial therapy for community-acquired UTIs.^16^ For recurrent infections, the guideline recommends that empirical therapy be guided by previous culture results pending urine culture and sensitivity results. Once available, therapy is tailored to prescribe the most narrow spectrum efficacious antibiotic wherever possible.^16^
The selection of empirical therapy for UTI management is dependent on the knowledge of circulating pathogens and their AMR patterns.^17^ Of concern, therefore, is the lack of susceptibility data for community-acquired UTIs in many LMICs, including Kenya. This is mostly due to the challenges with culture and susceptibility testing, some of which include infrastructural constraints, limited funding, prolonged turnaround times (TATs) and lack of skilled personnel.^4,18^ There is relatively limited information on the appropriateness of empirical antibiotic therapy in the management of community-acquired UTIs in LMICs. This study seeks to address the paucity of microbiological information on management of microbiologically confirmed UTI in symptomatic patients and evaluates the appropriateness of empirical UTI treatment based on culture and susceptibility results.
Materials and methods
Study design
A hospital-based cross-sectional study design was employed to recruit adult and child patients with UTI-like symptoms between July 2022 and April 2023.
Study setting
The participants were recruited from Mama Lucy Kibaki Hospital (MLKH) and Mbagathi County Hospital (MCH) located within Nairobi County, as shown in Figure 1. The Kenyan healthcare system is structured in a hierarchical manner consisting of six levels I–VI in ascending order. MLKH and MCH are Level V public referral hospitals. MCH and MLKH serve a large catchment area comprising both the middle and low socio-economic groups. The two hospitals were selected as there was limited information on the resistance profiles of circulating uropathogens and UTI patients are often treated empirically without culture confirmation.
Location of study sites, MLKH and MCH within Nairobi County, Kenya.
Participant recruitment and sample collection
A resident clinician identified adult (≥18 years) and child (5–17 years) outpatients presenting with one or more symptoms suggestive of UTI or for other causes that made the clinician to believe they might also have a UTI. The symptoms included lower abdominal pain, dysuria, strong persistent urge to urinate, haematuria, frequent micturition and/or unexplained fever (≥38°C), persistent irritability and suprapubic pain/tenderness to palpation in children. In addition to meeting the criteria of a presumptive UTI case, the participants had to meet the following criteria: report living within a 50 km radius from the hospital facility, have a mobile telephone number and be able to speak/understand/write either English or Kiswahili. The study objectives were explained, and patients willing to participate were taken through informed consent document in their preferred language. Consent was obtained from adult patients (≥18 years). Assent and consent were obtained for participants aged 13–17 years. Parents/guardians of participants aged <13 years consented on their behalf. Consenting participants signed and dated the consent forms. Participants/guardians who were not able to sign marked the consent with a thumb print. Consenting participants were issued with a unique identifiable number which linked their bar-coded consent form, demographic data questionnaire, and urine sample collection container. Self-collected midstream urine on a 20 mL sterile plain screw-capped universal bottle was obtained from each patient after guidance on the collection procedure. Parents/guardians were guided on how to collect midstream urine from their children. The samples were stored in a cool box (4°C) and transported to the Kenya Medical Research Institute (KEMRI) laboratory for processing within 2 h.
Data collection
A questionnaire was used to collect self-reported demographic information (age and gender) and previous antimicrobial use. Data regarding empirical antibiotic treatment were obtained from prescriptions administered to the patients during the hospital visit. All data were captured electronically into an epicollect database (https://five.epicollect.net is a free open-source data collection tool) and later linked to the laboratory urine culture results.
Microbiological tests
Urine culture
Using a standard sterile loop, an aliquot (10 µL) of urine was plated directly on cystine lactose electrolyte deficient (CLED) agar, blood agar (BA) and MacConkey agar (Oxoid, Basingstoke, UK) and incubated aerobically at 35°C–37°C for 24 hours. After an overnight incubation, quantification of colony-forming units (cfus) was done by counting the number of colonies on a plate and multiplying by the dilution factor, as previously described by Miles et al.^19^ Pure bacterial growth yielding colony counts of ≥10 000 (10^4^) cfu/mL was interpreted as a confirmed UTI case. A mixed culture (with more than one colony type) or growth of <10 000 (10^4^) cfu/mL was non-confirmatory for UTI.
The organisms were identified to the species level using colonial morphological characteristics on CLED, BA, MacConkey agar (Oxoid, Basingstoke, UK), Gram stain (Sigma-Aldrich, USA) and standard biochemical tests. Sulphide indole motility test, methyl red, oxidase, urease, triple sugar iron and citrate utilization were used to identify Gram-negative organisms.^20^ Coagulase, catalase and haemolytic patterns on BA were used to confirm the presence of Gram-positive bacteria. Where necessary, the analytical profile index (20E) test was used to confirm the identity of strains following the manufacturer’s guidelines (bioMerieux, Charbonnieres, Les Bains, France).
Antimicrobial susceptibility test
Antimicrobial susceptibility testing (AST) was performed according to the Kirby–Bauer disc diffusion method.^21^ The panel of antibiotic discs (Oxoid, Basingstoke, UK) tested included first line, amoxicillin–clavulanic acid (20/10 μg), nitrofurantoin (300 μg) and sulfamethoxazole/trimethoprim (23.75/1.25 μg), and second line, ciprofloxacin (5 μg) antibiotics used in the treatment of UTI as per local practice.^16^ Other antibiotics included in the panel were ceftazidime (30 μg), ceftriaxone (30 μg), cefepime (30 μg), cefoxitin (30 μg), gentamycin (10 μg), cefuroxime (30 μg), erythromycin (15 μg) and linezolid (30 μg). Susceptibility or resistance to the tested antibiotics was determined using the zone diameter interpretative criteria (breakpoints) according to the CLSI guidelines.^22^ Isolates that showed intermediate resistance to a given antibiotic were interpreted as resistant to that antibiotic. Escherichia coli (ATCC 25922) and Staphylococcus aureus (ATCC 25923) were used as quality control organisms to validate antibiotic disc potency and quality of the test media.
Evaluation of the appropriateness of empirical treatment
Appropriateness of empiric treatment was assessed by evaluating the treatment prescribed during the initial hospital visit with the subsequent laboratory urine culture and susceptibility results. The hospital visit during which the patient was recruited, and urine sample obtained, was defined as the initial visit. Empirical treatment was taken as any antibiotic treatment prescribed to the patient during the initial visit prior to urine culture results. Appropriateness was assessed on an individual patient basis for those patients whose urine specimen yielded significant bacterial growth for UTI (≥10^4^ cfu/mL). Appropriate empirical antibiotic therapy (AEAT) was considered if a UTI was confirmed on urine culture and the antibiotics prescribed were effective in inhibiting growth of the isolated pathogen in vitro.^23^ Inappropriate empirical antibiotic therapy (IEAT) was defined as UTI confirmed on laboratory culture, but with an isolated pathogen which was resistant to the antibiotic prescribed in vitro.^23^ AEAT was expressed as the percentage of patients with a culture-positive urine specimen and isolated pathogen tested as sensitive to the antibiotic prescribed. Conversely, IAET was expressed as the percentage of patients with a culture-positive urine specimen who had an empiric prescription for which the isolated pathogen was tested as resistant.
Statistical analysis
Data were downloaded from epicollect into Microsoft Excel (Microsoft Corp, Redmond, Washington, USA) and were analysed using STATA 16 (StataCorp. 2019. Stata 183 Statistical Software: Release 16. College Station, TX: StataCorp LLC). The questionnaire data were linked to urinalysis, empirical prescription and AST data using anonymous patient identifiers. Baseline characteristics of the study population were reported as median [interquartile range (IQR)] for age or as counts and percentages for categorical data. Differences between categorical variables were compared using the χ^2^ test or Fisher’s exact test where applicable. Statistical significance was considered at probability value of <0.05.
Ethical approval
This study received approval from the University of St. Andrews Teaching and Research Ethics Committee, UK (approval no. MD15749); Jomo Kenyatta University of Agriculture and Technology Institutional Ethics Review Board, Kenya (approval no. JKU/IERC/02316/0166); and National Commission for Science Technology and Innovation, Kenya (approval no. P/21/12520). Nairobi Metropolitan Services, MLKH and MDH provided approvals for the access to the study sites. Informed consent was obtained from each participant included in the study.
Results
Characteristics of the study participants
Participants’ characteristics are shown in Table 1. Five hundred and fifty-two were enrolled. The majority were adults, 494 (89.4%), and females accounted for 398 (72%). The most frequent age bracket was 21–30 with a median age of 29 years (IQR: 24–36). Amongst the 552 enrolled patients, 236 (43%) had taken medication 2 weeks prior to enrolment, 168 (71%) of these had taken antibiotics, whilst 68 (29%) had taken medications other than antibiotics.
Proportion of microbiologically confirmed UTI
The overall proportion of culture-confirmed UTI amongst the studied population was 22.5% (124/552), being significantly higher in females than males (Table 1). Of these, 274 (49.6%) received empirically prescribed antibiotic treatment, and 242 (43.8%) did not receive any antibiotic treatment, whilst for 36 (6.5%), it was not known whether they received an antibiotic or not (participants could not be reached by phone or failed to come back to the hospital for the laboratory results). Amongst the 274 that received empirical antibiotic therapy, urine culture-confirmed UTI in 95 (35%). Of the 242 that did not receive therapy, 27 (11.1%) had UTI confirmed. Amongst those whose therapy status was not known, two (5.5%) had confirmed UTI. There was a significant difference in UTI detection between those who received empirical therapy and those who did not (P value of <0.05).
Microbiological characteristics
A total of 124 bacterial isolates were characterized from the 552 urine samples analysed, 97 (78%) of which were Gram-negative. The predominant uropathogen was E. coli, 64 (52%), followed by Klebsiella spp., 21 (17%); S. aureus, 14 (11.3%); coagulase-negative staphylococci (CoNS), 7 (5.6%); Enterococcus faecalis, 6 (4.8%), Proteus spp., 7 (5.6%); Acinetobacter baumannii, 1 (0.8%); Pseudomonas aeruginosa, 2 (1.6); and Citrobacter koseri, 2 (1.6%).
AMR patterns
AMR profiles of the 124 isolated UTI pathogens are shown in Table 2. For Gram-negative organisms, resistance towards common UTI treatments—β-lactams, fluoroquinolones and aminoglycosides—ranged from 24% to 57%. Within the bacterial groups, E. coli, the predominant uropathogen, showed high resistance to sulfamethoxazole/trimethoprim at 77%, ciprofloxacin at 61%, amoxicillin–clavulanic acid at 47% and ceftriaxone at 52%, whilst nitrofurantoin was the most effective agent for E. coli. The overall resistance of Gram-positive bacteria was 52% for sulfamethoxazole/trimethoprim, 67% for ciprofloxacin and 26% for amoxicillin–clavulanic acid. Nitrofurantoin and linezolid were the most effective agents against Gram-positive isolates.
Empirical antimicrobial prescribing
There were 15 antibiotics and antibiotic combinations prescribed empirically. Most of the patients 244 (89.0%) received one antibiotic and 28 (10.2%) received 2 antibiotics, whilst 2 (0.7%) received 3 antibiotics (Figure 2). Antimicrobial treatment was prescribed to 49.6% of all patients, with a first-line empirical treatment recommended in national guidelines utilized in 29.6% of cases. The most frequently prescribed antibiotics were ciprofloxacin (30.3%), amoxicillin–clavulanic acid (17.5%), levofloxacin (15.7%), nitrofurantoin (11.6%) and cefuroxime (10.6%), whilst the least prescribed were sulfamethoxazole/trimethoprim (1.1%) and cefepime (0.4%). Ceftriaxone/ciprofloxacin and cefixime/azithromycin were the most prescribed combination therapies at 4.7% and 3.2%, respectively.
An overview of empirical antimicrobial prescribing at the outpatient departments of MLKH and MCH, Nairobi County, Kenya.
Appropriateness of empirical antibiotic treatment (AEAT)
Of the 95 patients with bacteriological confirmation of UTI, the antimicrobial susceptibility results were compared with the empirical therapy prescribed. The most prescribed antibiotics empirically were found to be inappropriate as follows: ciprofloxacin was prescribed 27 times, but in 11 cases (41%), the isolated organisms were resistant; for amoxicillin–clavulanic acid, in 12 (40%) out of the 30 prescriptions, organisms were resistant; for nitrofurantoin, 4 (27%) of the 15 prescriptions proved to be inappropriate, and finally, cefuroxime was prescribed 7 times, but 6 (88%) cases were inappropriate. Overall, most patients 50 (53%) received appropriate empirical therapy, whilst for 38 (40%), the therapy was found to be inappropriate. The appropriateness of empirical therapy to 7 (7%) patients could not be determined as the antibiotics prescribed (levofloxacin and cefixime/azithromycin) were not in the AST panel (Figure 3).
Evaluation of appropriateness of empirical therapy. Appropriateness or inappropriateness was expressed as a percentage based on n = 95 patients who had laboratory-confirmed UTI and had susceptible or resistant AST results, respectively.
Discussion
This study determined the proportion of microbiologically confirmed UTI cases amongst 552 symptomatic patients and evaluated the appropriateness of empiric antibiotic therapy prescribed to symptomatic UTI patients. Our findings suggest that in about 40% of the cases, empirical antimicrobial prescribing for UTI proves inappropriate in the context of subsequent urine culture and susceptibility results. IEAT can be associated with significant adverse outcomes. Whilst changing to the right antibiotic upon receipt of the culture results is beneficial and necessary for targeted therapy, it may not fully mitigate the disadvantages of not having the correct antibiotic from the onset.^23^ IEAT may promote selection pressures that can result in the growth of resistant bacterial populations, which not only affects the individual patient but also poses a broader public health threat to everyone. Furthermore, IEAT can result in unnecessary healthcare costs including expenses associated with additional tests and treatment for complications.^24^ These consequences underscore the importance of judicious antibiotic prescribing to optimize patient outcomes and preserve the effectiveness of antibiotics for future generations.
It is challenging to find comparable studies because of the wide variation in the way that IEAT is defined. Nevertheless, a recent study by Maina et al.^25^ investigated the appropriateness of antibiotic use across a range of disease conditions amongst 1502 patients in Kenyan public hospitals. Amongst other findings, these results showed that 26% of 94 patients who had UTI and 68% of 135 patients in the surgical unit received empirical treatment that was inappropriate for the pathogens isolated. Higher rates ranging from 54% to 87% of IEAT in UTI have been reported by other studies.^26–30^ However, whilst our study defined inappropriate treatment according to the criteria outlined by Davey et al.,^23^ these studies had a combination of definitions which included antibiotic prescriptions without bacteriological confirmation, prescription of an antibiotic to which isolated pathogen was resistant, inappropriate antibiotic dosage, lack of sensitivity testing and therapy not being within the treatment guidelines.
Overall, only 1 in 5 patients suspected of having UTI had bacteriological confirmation by the criteria applied in this study (monoculture growth of 10^4^ cfu/mL). However, a considerable proportion of the patients, 168 (30%), had taken antibiotics prior to the initial hospital visit. This highlights the challenge of conducting and interpreting microbiology culture results in patients previously exposed to antibiotics, as prior research has demonstrated that antibiotic exposure is a strong predictor of negative culture outcomes.^31^ This further illustrates the difficulty healthcare providers face in deciding on the need for antibiotic prescriptions based solely on clinical symptoms. Evidence on how well symptoms predict the true presence of UTI when compared with urine culture has shown varied results and is estimated to have an error rate of up to 33%.^31^ In this study, 11% of patients had laboratory confirmation of UTIs, yet they did not receive empirical treatment. These findings are comparable with those reported by Alkhawaldeh et al.^26^ and Zhu et al.^29^, in which 15.7% and 12.5% patients, respectively, did not receive empirical treatment but were confirmed to have UTI by the culture method. Whilst treating only after the microbiological results are obtained ensures that the correct antimicrobial therapy is chosen, the strategy increases the risk of a worse outcome. These findings highlight the need of a near point-of-care test that can detect UTI and provide preliminary antimicrobial susceptibility reports to guide decision-making in UTI management.
There was a wide variation of empirical antimicrobial prescribing practice amongst prescribers, with differences in preference for certain antimicrobials seen. This was most striking in relation to the prescription of fluoroquinolones (ciprofloxacin and levofloxacin), β-lactam/β-lactamase inhibitor combinations (AMC) and nitrofurantoin. Despite being a second-line therapy, more than half 140 (51%) of the patients received fluoroquinolones. This is high considering the already reported high resistance^32^ and adverse ecological effects^33^ associated with this class of antimicrobials. A further 6.3% of the patients received sulfamethoxazole/trimethoprim despite this antibiotic not being amongst the recommended empirical treatments^16^ and local resistance patterns already exceeding 20%.^32^ One possible explanation to these findings is the absence of sufficient laboratory support, which influences prescription pattern and choice, leading to a predominance of broad-spectrum prescriptions and polypharmacy.^34^ The high-grade resistance exhibited against amoxicillin–clavulanic acid makes this agent suboptimal for UTI treatment in the absence of laboratory support, notwithstanding that it is recommended in the national guidelines as first-line empirical therapy. This illustrates a clear need for more comprehensive national surveillance and perhaps a review of the guidelines. In contrast, nitrofurantoin was an appropriate agent for both Gram-positive and Gram-negative bacteria, and its empirical use is encouraged in the absence of any contraindication.^35^
The high proportion of resistance amongst UTI pathogens reported in this study and in neighbouring countries^17,36^ can likely be explained by records of inappropriate antibiotic use which is one of the key drivers of AMR. This could be caused by inadequate microbiology diagnostics, lack of updated antibiotic susceptibility data and self-treatment using over-the-counter antibiotics, a widespread practice in many LMICs.^37^ Some challenges identified in laboratory diagnostics have been the long TAT, high cost of investigation and lack of trust in and utilization of laboratory results by clinicians.^38^ Performing culture and susceptibility tests may contribute to higher healthcare costs for patients. However, it is essential to consider this added expense in light of the potential savings from avoiding inappropriate or unnecessary treatment that are not supported by laboratory data.
This study has some limitations. First, the patients were only recruited from the outpatient departments of two health facilities, so generalization of findings to other settings, even within Kenya, should be made with caution. Nevertheless, patients were sequentially recruited without stringent selection criteria and the same approach was taken to investigation of every participant which minimized bias and increased the likelihood that the results reflected the general population and routine medical practices. Further, the findings do not give insights into the appropriateness of prescription in private health facilities or in inpatients. However, it is considered satisfactory to provide background information on appropriateness of empirical treatment. Secondly, the population of outpatients who presented with symptoms suggestive of UTI may have had other underlying conditions given that UTI symptoms may overlap with those of other diseases. However, we assumed that all antibiotics prescribed during initial hospital visit before the AST results (when each patient was recruited into the study and urine collected) were for the UTI episode.
Conclusion
The study has demonstrated that achieving appropriate empirical antibiotic treatment for UTIs is a difficult task, especially in the era of increased AMR in clinical infections, situations of limited resource and much habitual over-the-counter antibiotic use. At present, optimal empiric therapy is not being achieved. This situation could be improved if capacity for delivering accurate and timely susceptibility results to clinicians to aid their clinical decision-making could be achieved. Finally, it is crucial to enhance routine AMR surveillance to support effective antimicrobial stewardship practices in healthcare facilities.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Harbottle H, Thakur S, Zhao S et al Genetics of antimicrobial resistance. Anim Biotechnol 2006; 17: 111–24. 10.1080/1049539060095709217127523 · doi ↗ · pubmed ↗
- 2World Health Organization . Global Antimicrobial Resistance and Use Surveillance System 2022. https://www.who.int/publications/i/item/9789240062702
- 3O’Neill J . Antimicrobial resistance: tackling a crisis for the health and wealth of nations. The Review on Antimicrobial Resistance, 2014. https://wellcomecollection.org/works/rdpck 35v.
- 4Murray CJ, Ikuta KS, Sharara F et al Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet 2022; 399: 629–55. 10.1016/S 0140-6736(21)02724-035065702 PMC 8841637 · doi ↗ · pubmed ↗
- 5Petti CA, Polage CR, Quinn TC et al Laboratory medicine in Africa: a barrier to effective health care. Clin Infect Dis 2006; 42: 377–82. 10.1086/49936316392084 · doi ↗ · pubmed ↗
- 6Elbireer AM, Jackson JB, Sendagire H et al The good, the bad, and the unknown: quality of clinical laboratories in Kampala, Uganda. P Lo S One 2013; 8: e 64661. 10.1371/journal.pone.006466123737993 PMC 3667826 · doi ↗ · pubmed ↗
- 7Asiimwe BB, Kiiru J, Mshana SE et al Protocol for an interdisciplinary cross-sectional study investigating the social, biological and community-level drivers of antimicrobial resistance (AMR): Holistic Approach to Unravel Antibacterial Resistance in East Africa (HATUA). BMJ Open 2021; 11: 414–18. 10.1136/bmjopen-2020-041418 PMC 794225134006022 · doi ↗ · pubmed ↗
- 8Ndaki PM, Mushi MF, Mwanga JR et al Dispensing antibiotics without prescription at community pharmacies and accredited drug dispensing outlets in Tanzania: a cross-sectional study. Antibiotics (Basel) 2021; 10: 1025. 10.3390/antibiotics 1008102534439074 PMC 8389015 · doi ↗ · pubmed ↗