Adrenocortical Tumor Associated With Pathogenic Variant in KCNJ5 and DNA Methylation of CYP11B2 in Primary Aldosteronism
Ko Aiga, Mitsuhiro Kometani, Masashi Demura, Takashi Yoneda

TL;DR
A case of adrenal tumor with a KCNJ5 mutation and CYP11B2 methylation is linked to a type of high blood pressure called primary aldosteronism.
Contribution
This case study links a pathogenic KCNJ5 variant and CYP11B2 DNA methylation to unilateral primary aldosteronism.
Findings
A pathogenic variant in KCNJ5 was detected in the aldosterone-producing adenoma.
DNA methylation in the CYP11B2 promoter region was associated with suppressed CYP11B2 expression.
Adrenal vein sampling confirmed left adrenal gland dominance despite no visible tumor on imaging.
Abstract
Primary aldosteronism (PA) is a subtype of secondary hypertension categorized as either unilateral PA (eg, aldosterone-producing adenoma [APA]) or bilateral PA. CYP11B2, an aldosterone synthase, is highly expressed in APA. Recent studies have revealed a high prevalence of pathogenic variants in KCNJ5 and the role of DNA methylation on CYP11B2 in APA. We present a case of unilateral PA with pathogenic variants in KCNJ5 and suppressed CYP11B2 expression. A 55-year-old woman with hypertension was referred to our hospital. A high aldosterone-renin ratio was observed; PA was confirmed using the captopril challenge test and the furosemide upright test. Although computed tomography showed no evident tumors in either adrenal gland, adrenal vein sampling revealed left gland dominance. Postoperatively, the aldosterone-renin ratio decreased and captopril challenge test showed negative findings.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
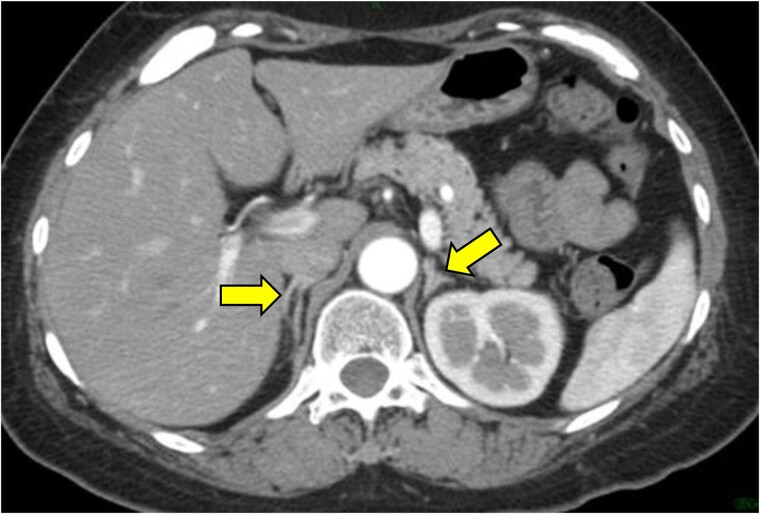 Figure 1
Figure 1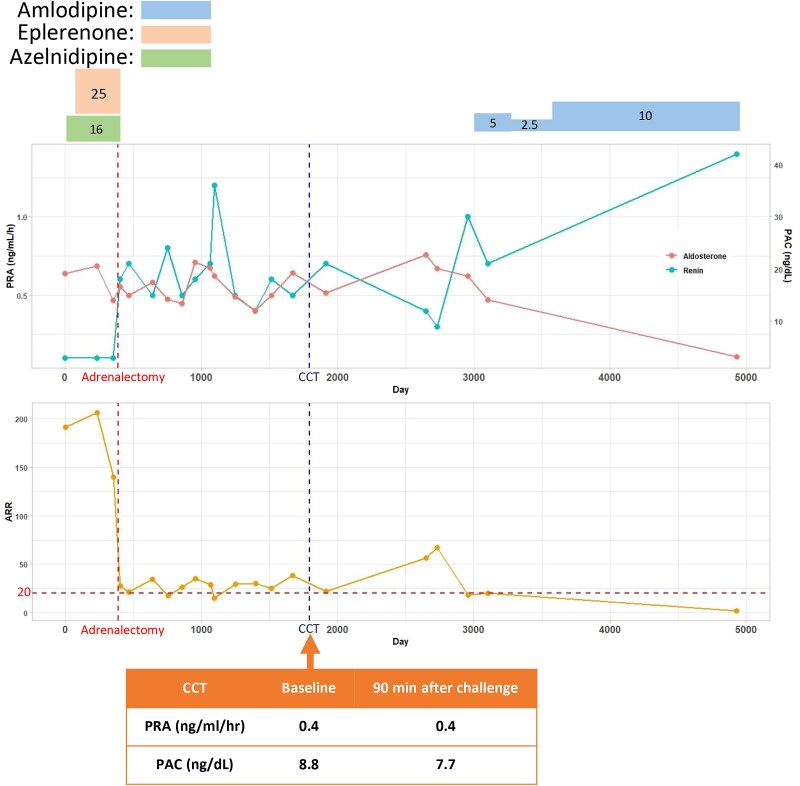 Figure 2
Figure 2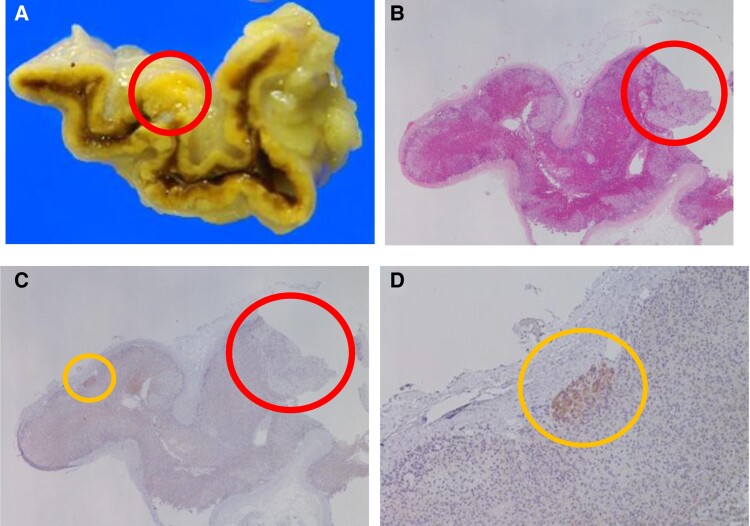 Figure 3
Figure 3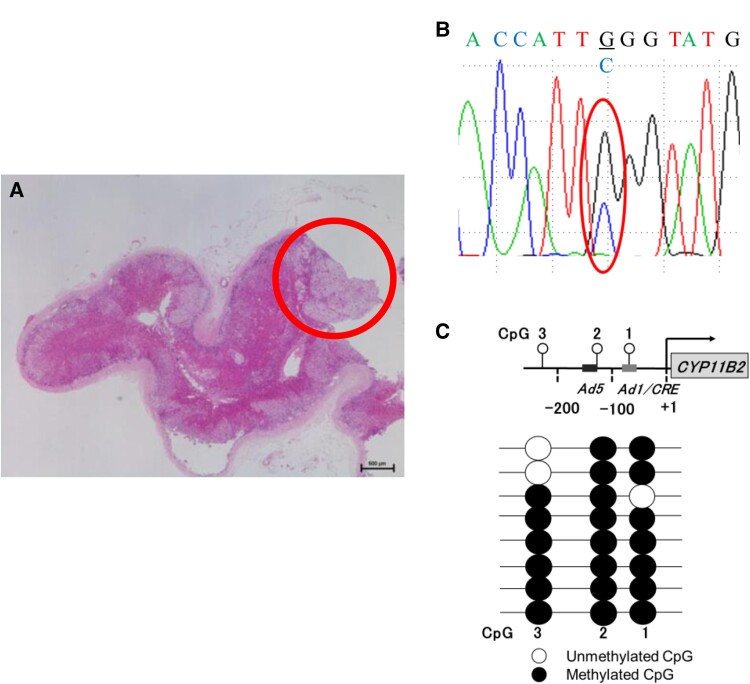 Figure 4
Figure 4| Preoperative | Baseline | 90-minutes after challenge | 120 in after challenge |
|---|---|---|---|
| FUT | PRA <0.1 (ng/mL/h) | PRA 0.3 (ng/mL/hr) | |
| CCT | PRA: 0.5 (ng/mL/h) | PRA: 0.2 (ng/mL/h) | — |
| Post-operative | Baseline | 90 minutes after challenge | 120 minutes after challenge |
| CCT | PRA: 0.4 (ng/mL/h) | PRA: 0.4 (ng/mL/h) |
| Location | PAC | F | PAC/F | SI | LI | CR |
|---|---|---|---|---|---|---|
| IVC | 7.3 (ng/dL) | 8 (µg/dL) | 0.91 (ng/dL)/(µg/dL) [0.033 (ng/dL)/(nmol/L)] | — | — | 3 |
| RAV | 294 (ng/dL) | 107 (µg/dL) [2952 (nmol/L)] | 2.75 (ng/dL)/(µg/dL) [0.10 (ng/dL)/(nmol/L)] | 13 | 2.7 | |
| LAV | 424 (ng/dL) | 57 (µg/dL) [1573 (nmol/L)] | 7.44 (ng/dL)/(µg/dL) [0.27 (ng/dL)/(nmol/L)] | 7 | — |
- —Japan Society for the Promotion of Science10.13039/501100001691
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHormonal Regulation and Hypertension · Adrenal and Paraganglionic Tumors · Cardiovascular, Neuropeptides, and Oxidative Stress Research
Introduction
Primary aldosteronism (PA) is a common form of secondary hypertension, which is characterized by hypersecretion of aldosterone. There is an increased risk of cardiovascular morbidity and mortality in PA because of excess aldosterone production (1). Based on etiology, PA is divided into 2 subtypes: unilateral PA, such as aldosterone-producing adenoma (APA), and bilateral PA, often referred to as idiopathic adrenal hyperaldosteronism (1). Additionally, adrenalectomy is the preferred treatment for APA because of its potential curative effect (1). Conversely, medications are administered lifelong for idiopathic adrenal hyperaldosteronism (1).
In the past decade, the relationship between APA, gene mutations, and DNA methylation has been explored (2, 3). Pathogenic variants in KCNJ5 induce the upregulation of CYP11B2 expression, an aldosterone synthase, leading to increased aldosterone production (4). Moreover, hypomethylation of the CYP11B2 promoter promotes the expression of CYP11B2 (2).
In this report, we present a case of adrenocortical adenoma in which a pathogenic variant in KCNJ5 was detected in the nodule of the resected tissue; however, it did not show positive CYP11B2 immunostaining. The DNA methylation status was further analyzed to explore the underlying molecular mechanisms.
Case Presentation
A 55-year-old woman with hypertension was referred to our department. At age 40 years, her blood pressure was 120 to 130/80-90 mm Hg. Thirteen years later, her systolic blood pressure began to rise to approximately 150 to 160 mm Hg. However, at age 55 years, the patient was hospitalized for cochlear implant surgery. Her systolic blood pressure remained elevated at 140 mm Hg during hospitalization. She was then referred to the endocrinology department for further evaluation.
Diagnostic Assessment
The patient was a social drinker with a smoking history of an average of 10 cigarettes per year when she was aged 20 to 23 years. She had a medical history of appendicitis at age 10 years. Her family history included hypertension and depression in her mother and liver cirrhosis in her father. She was on a prescription of calcium channel blockers (azelnidipine 16 mg) when she was referred to our hospital. On physical examination, the patient's height, weight, body mass index, blood pressure, pulse, and body temperature were 153 cm, 64 kg, 27 kg/m^2^, 149/92 mm Hg, 65 beats/min, and 36.8 °C, respectively. The laboratory data revealed plasma renin activity (PRA) suppression at 0.1 ng/mL/h (normal value: 0.2-2.7 ng/mL/h) and an elevated plasma aldosterone concentration (PAC) level at 19.1 ng/dL (normal value: 2-13 ng/dL). However, hypokalemia was not observed. The captopril challenge test (CCT) and furosemide upright test were performed, and both tests were positive (Table 1). Following the Japan Endocrine Society PA guidelines, the cutoff value of the CCT and furosemide upright test were assigned by the aldosterone-renin ratio: 200 (after 90 minutes) and PRA: 2.0 ng/mL/h (after 120 minutes), respectively (1). Based on these confirmatory tests, the patient was diagnosed with PA. Computed tomography (CT) was conducted to investigate the lateralization of the PA. However, no apparent lesions were observed in the CT images (Fig. 1). Adrenal vein sampling (AVS) without ACTH stimulation was performed to further clarify PA localization with the successful selection of both adrenal veins. Per the PA guidelines, the cutoff values of the selectivity index (SI), lateralization index (LI), and contralateral ratio (CR) were assigned as 2, 2, and 1, respectively (1, 5). SI, LI, and CR were used to evaluate the cannulation of the catheter, lateralization, and suppression of the nondominant glands, respectively. The results revealed that aldosterone was predominantly produced in the left adrenal gland (Table 2). However, the CR did not show the suppression of the nondominant adrenal gland.
Abdominal computed tomography (CT) imaging. No apparent tumor was observed from the CT imaging. The yellow arrows indicate adrenal glands.
Treatment
Based on the AVS results, the patient chose surgical treatment. Ninety-seven days before surgical treatment, the patient was prescribed 25 mg of eplerenone daily. A left adrenalectomy was performed.
Outcome and Follow-up
After adrenalectomy, PRA, PAC, and aldosterone-renin ratio improved, and CCT was negative 1400 days after the surgery (Fig. 2). Histopathological and genetic analyses were performed on the resected tissues. Macroscopic findings and hematoxylin and eosin staining revealed the presence of a 2-mm nodule in the resected tissue (Fig. 3). Genetic analysis of the nodule revealed a pathogenic variant in KCNJ5 (G151R) (Fig. 4). Notably, CYP11B2 immunostaining was negative for the nodule (Fig. 3). Furthermore, CYP11B2 immunostaining revealed the presence of an aldosterone-producing cell cluster (APCC) in the vicinity of the nodule (Fig. 3). To explore the mechanisms underlying the low expression of CYP11B2 in the nodule, we investigated the DNA methylation status in the promoter region of CYP11B2. The detailed method for DNA methylation analysis has previously been described by Demura et al (6). The analysis was performed to evaluate the methylation rates of 3 CpG sites upstream of the promoter region of CYP11B2 (Fig. 4). The rates of methylation in CpG1, CpG2, and CpG3 were 75% (6/8), 100% (8/8), and 87.5% (7/8), respectively. Two cis-acting regulatory elements, Ad1 and Ad5, are located in CpG1 and CpG2, respectively.
The timeline of adrenal hormones and captopril challenge test. Blue, orange, and green boxes represent amlodipine, eplerenone, and azelnidipine, respectively. The numbers inside the box show the quantity of medicine (units: mg/day for amlodipine, eplerenone, and azelnidipine, respectively). Red and blue dotted lines represent adrenalectomy and captopril challenge test results, respectively.
Pathological analysis. Gross pathological finding. The red circle indicates the 2-mm-sized nodule. (A) Microscopic finding (low magnification) with hematoxylin and eosin staining. The red circle indicates the nodule. (B) Microscopic finding (low magnification) with CYP11B2 immunohistochemistry results. (C) The red and orange circles indicate the nodule and aldosterone-producing cell cluster (APCC), respectively. Microscopic finding (high magnification) with CYP11B2 immunohistochemistry results. The orange circle indicates the APCC (D).
Gene and methylation analysis. Sanger sequencing and DNA methylation analysis were performed at the region of the red circle (nodule). (A) A pathogenic variant in KCNJ5 was detected in the nodule. The amino acid substitution was G151R. (B) DNA methylation analysis using a DNA methylation activity assay. White/black circles represent unmethylated and methylated CpG sites, respectively. The promoter region of CYP11B2 in the nodule was also investigated. (C).
Discussion
APA is known to express elevated levels of CYP11B2, shown through positive immunohistochemistry for CYP11B2 (4). Pathogenic variants in KCNJ5 exhibit the highest prevalence among APA-driving genes in Japan, accounting for 73% of all APAs (3). In the present case, we detected a pathogenic variant in KCNJ5 in the adrenocortical adenoma. Therefore, this case was initially considered a typical APA. However, histopathological analysis was negative for CYP11B2 expression in the nodule, but an APCC was confirmed in the adjacent adrenal gland. Furthermore, methylation of the promoter region of CYP11B2 was confirmed. This study is the first to investigate the relationship between DNA methylation and KCNJ5 mutant nodules with CYP11B2 negative immunostaining.
Recently, the criteria for confirmatory tests have been updated in Japan because of the replacement of the radioimmunoassay with the chemiluminescent enzyme immunoassay for PAC measurement. The present case was diagnosed and treated before the introduction of the chemiluminescent enzyme immunoassay method for PAC measurement. Further, the criteria for AVS without ACTH stimulation and confirmatory tests were followed as per the Japan Endocrine Society PA guidelines and the Endocrine Society PA guidelines, respectively. In the present case, the LI showed a slightly higher value than the cutoff value, which led to the left adrenalectomy. Conversely, the CR showed no suppression in the contralateral gland. Thus, asymmetrical PA with slightly left adrenal gland dominance could be considered. However, the recovery of blood pressure and hormone levels with negative CCT results after adrenalectomy supported left adrenal gland predominance. Although CR did not show the suppression of the nondominant adrenal gland as determined by the LI, the outcome of the adrenalectomy justified the validity of the LI. Although the negative result of CCT demonstrated the improvement of hormone abnormalities, the clinical outcome still seemed insufficient. The amlodipine dose increased after surgery, followed by the changes in PAC and PRA (Fig 2.). A mild APA-like lesion may have been in the contralateral adrenal gland. Therefore, regular follow-ups have been performed to check and control the hormone levels after the operation.
Recent findings have demonstrated that DNA methylation status at the CpG island in the promoter region of CYP11B2 regulates its expression (7). Studies have revealed that DNA methylation of CpG sites in the Ad1 and Ad5 elements in the promoter region of CYP11B2 inhibits the binding of the coactivator complex (CREB1, NGF1B, and NURR1) to its regions, inhibiting the coactivator complex from promoting the expression of CYP11B2 (2). Furthermore, hypermethylation promotes the binding of the corepressor complex (MECP2) to Ad1 and Ad5, which consequently suppresses the expression of CYP11B2 (2). A previous study also demonstrated the hypomethylation of CpG1(Ad1), CpG2(Ad5), and CpG3 in APA compared to the control: the mean value of methylation ratio of CpG1(Ad1), CpG2(Ad5), and CpG3 in APA were less than 20%, 50%, and 50%, respectively (8). In the present case, the DNA methylation rate at CpG sites near the Ad1 and Ad5 binding sites was higher than that in the previous report (CpG1[Ad1]: 75%, CpG [Ad2]: 100%), suggesting that CYP11B2 expression was suppressed (8). This result is consistent with negative CYP11B2 immunohistochemistry results but is inconsistent with APA characteristics. Furthermore, immunohistochemical analysis revealed a site of strong CYP11B2 expression in the vicinity of the adenoma, which was thought to be an APCC and might have been the responsible lesion.
The relationship between APA with the pathogenic variant in KCNJ5 and the DNA methylation status of CYP11B2 has not been elucidated. Previous studies confirmed hypomethylation in the promoter region of CYP11B2 in APA compared to the normal adrenal tissue (2). However, a previous report demonstrated that APA-driving genes inducing aldosterone excess (ie, KCNJ5 and ATP1A1) did not relate to DNA methylation status in the CYP11B2 promoter region (9). Based on the present case, the pathogenic variant in KCNJ5 did not cause hypomethylation in CYP11B2. Instead, CYP11B2 was methylated, which possibly led to the negative immunochemistry for CYP11B2. Other factors may have been involved in regulating DNA methylation in CYP11B2.
According to previous studies, nontumor unilateral PA had been reported in the literature (10). In the present case, APCC was detected through CYP11B2 immunostaining. However, the adenoma showed negative results for CYP11B2. This implied that APCC might have been the possible source of aldosterone excess. Nishimoto et al demonstrated the presence of nontumor lesions with small cell clusters named possible APCC to APA transitional lesions (pAATLs) by performing gene analysis and immunohistological evaluations (10). Although gene analysis and CYP11B1 immunostaining were not available because of limited resources, the APCC might have been a pAATL and could have been responsible for the lesion in the present case. However, APCC was detected in the healthy adrenal cortex by the donors (11). It was difficult to distinguish pAATLs and APCC without integrated immunohistochemistry.
Referring to the previous literature, the KCNJ5 mutant nodule with negative CYP11B2 immunostaining is rare in PA. Xie et al reported positive immunostaining for CY11B2 in all the multiple nodules with pathogenic variants in KCNJ5 (17/17), which implied a high prevalence of CY11B2 activation in nodules with pathogenic variants in KCNJ5 (12). However, several studies reported KCNJ5 mutant nodules with negative CYP11B2 immunostaining. A study reported by Sousa et al investigated the heterogeneity in CYP11B2 expression in adenomas with pathogenic variants in KCNJ5 (13). The study revealed 2 kinds of adrenocortical adenomas in 1 adrenal tissue: adrenocortical adenoma with CYP11B2 activation or without activation (13). This could have been explained by the DNA methylation status. Likewise, in the present case, DNA methylation at the promoter region of CYP11B2 might have been observed in the CYP11B2-deactivated adenoma. Based on the results of immunohistochemistry in the present case and the previous study, some adrenocortical adenomas with pathogenic variants in KCNJ5 may not be in charge of the lesion. Rather, aldosterone production could be suppressed. Thus, CYP11B2 immunohistochemistry should be conducted to accurately clarify the lesion of the unilateral PA.
In summary, we present a case of unilateral PA with adrenocortical adenoma. Although the pathogenic variant in KCNJ5 was detected, CYP11B2 expression was suppressed, as confirmed by the negative immunohistochemistry results of CYP11B2 and methylation at the promoter region of CYP11B2. This intriguing case prompts further research into the effects of the relationship between DNA methylation and adrenocortical adenoma.
Learning Points
Adrenal tumors with pathogenic variants in KCNJ5 do not always have a strong CYP11B2 expression.The aldosterone synthesis could possibly be suppressed by the DNA methylation of CYP11B2 in unilateral PA with adrenocortical adenoma.The criteria for AVS subtyping are still controversial. Postoperative evaluation, including pathological findings and clinical outcomes, should be confirmed to validate the AVS result.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nishikawa T, Omura M, Satoh F, et al Guidelines for the diagnosis and treatment of primary aldosteronism—the Japan Endocrine Society 2009. Endocr J. 2011;58(9):711‐721.21828936 10.1507/endocrj.ej 11-0133 · doi ↗ · pubmed ↗
- 2Takeda Y, Demura M, Yoneda T, Takeda Y. DNA methylation of the angiotensinogen gene, AGT, and the aldosterone synthase gene, CYP 11B 2 in cardiovascular diseases. Int J Mol Sci. 2021;22(9):4587.33925539 10.3390/ijms 22094587 PMC 8123855 · doi ↗ · pubmed ↗
- 3Scholl UI . Genetics of primary aldosteronism. Hypertension. 2022;79(5):887‐897.35139664 10.1161/HYPERTENSIONAHA.121.16498 PMC 8997684 · doi ↗ · pubmed ↗
- 4Oki K, Gomez-Sanches CE. The landscape of molecular mechanism for aldosterone production in aldosterone-producing adenoma. Endocr J. 2020;67(10):989‐995.32968034 10.1507/endocrj.EJ 20-0478 PMC 9044104 · doi ↗ · pubmed ↗
- 5Funder JW, Carey RM, Mantero F, et al The management of primary aldosteronism: case detection, diagnosis, and treatment: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2016;101(5):1889‐1916.26934393 10.1210/jc.2015-4061 · doi ↗ · pubmed ↗
- 6Wang F, Demura M, Cheng Y, et al Dynamic CCAAT/enhancer binding protein-associated changes of DNA methylation in the angiotensinogen gene. Hypertension. 2014;63(2):281‐288.24191285 10.1161/HYPERTENSIONAHA.113.02303 · doi ↗ · pubmed ↗
- 7Takeda Y, Demura M, Kometani M, Karashima S, Yoneda T, Takeda Y. Molecular and epigenetic control of aldosterone synthase, CYP 11B 2 and 11-hydroxylase, CYP 11B 1. Int J Mol Sci. 2023;24(6):5782.36982850 10.3390/ijms 24065782 PMC 10054571 · doi ↗ · pubmed ↗
- 8Takeda Y, Demura M, Wang F, et al Epigenetic regulation of aldosterone synthase gene by sodium and angiotensin II. J Am Heart Assoc. 2018;7(10):e 008281.29739797 10.1161/JAHA.117.008281 PMC 6015301 · doi ↗ · pubmed ↗