Modified Z-plasty of the Patellar Ligament with Reinforcement of the Quadriceps Tendon in the Treatment of Patella Baja
Tiago António Almeida Orange Costa, Francisco Bernardes, José Miradouro, Joana Pereira, Pedro Barreira, João Carvalho

TL;DR
A modified Z-plasty technique combined with quadriceps tendon reinforcement successfully treated patella baja in a patient after knee surgery.
Contribution
A novel soft tissue surgical approach for patella baja is described with significant functional improvement.
Findings
The patient's Lysholm Knee Score improved from 16 to 81 after the procedure.
Early mobilization and return to daily activities were achieved following the surgery.
Abstract
Patella baja is an infrequent knee pathology, but it is limiting due to joint stiffness and localized pain in the anterior region of the knee. It may occur after trauma, prolonged immobilization or local surgical intervention. The striking pathological finding is the shortening and increase in thickness of the patellar ligament. Several surgical techniques have been described for its treatment, and there is no standardized treatment. We describe the case of a 73-year-old female patient who presented with knee stiffness, significant functional deficit, and patella baja after total knee arthroplasty. She underwent a recently described soft tissue surgical procedure, with excellent functional evolution, improving from a Lysholm Knee Score of 16 to 81 points, allowing early mobilization and return to daily life activities. A patela baixa é uma patologia do joelho pouco frequente, mas…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Fig. 1
Fig. 1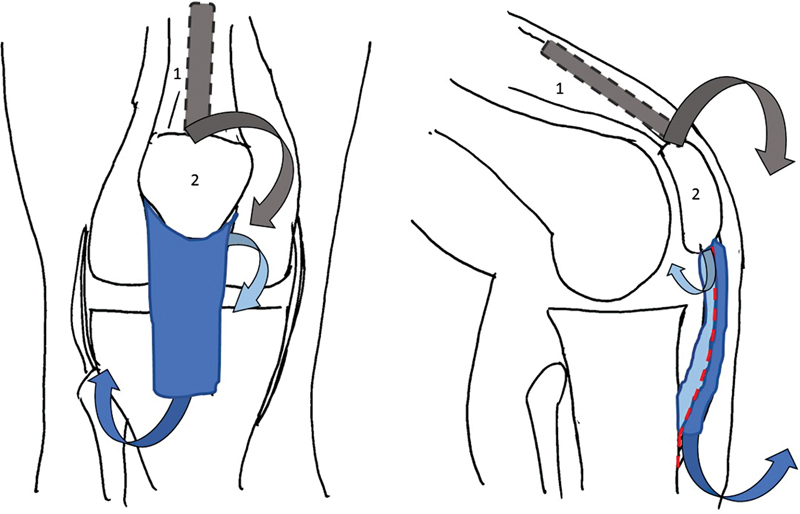 Fig. 2
Fig. 2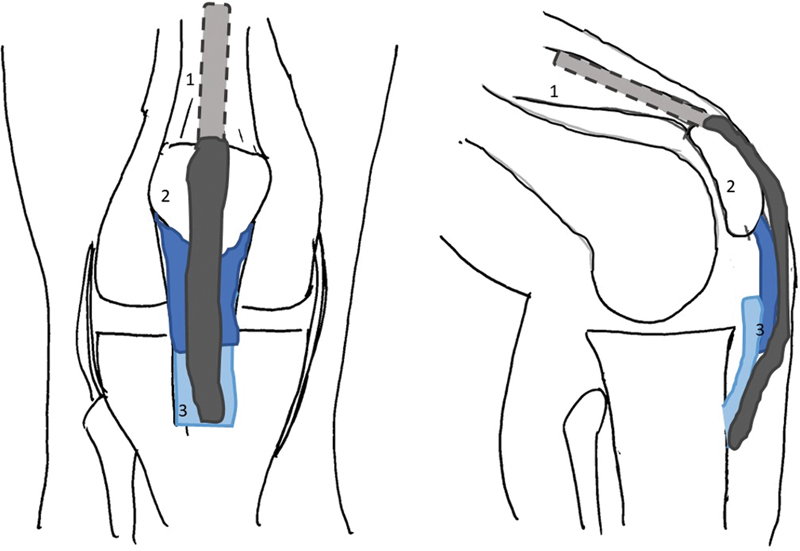 Fig. 3
Fig. 3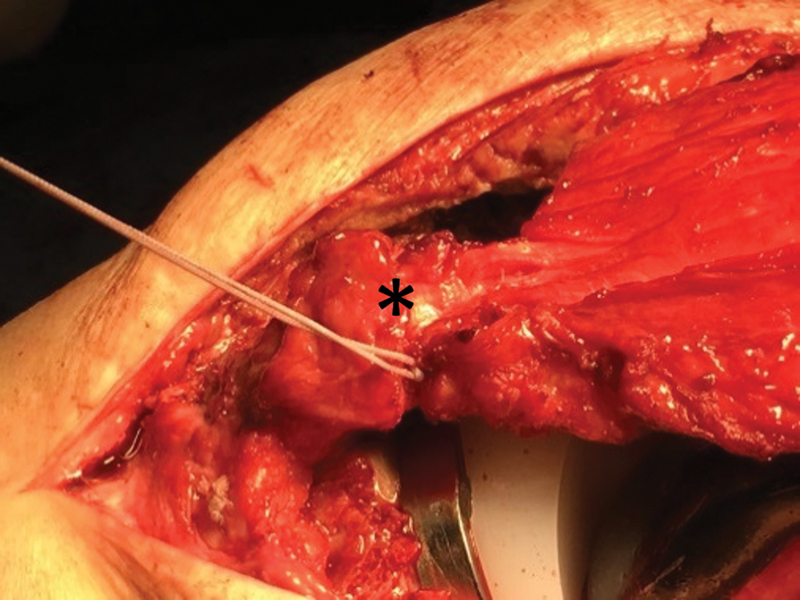 Fig. 4
Fig. 4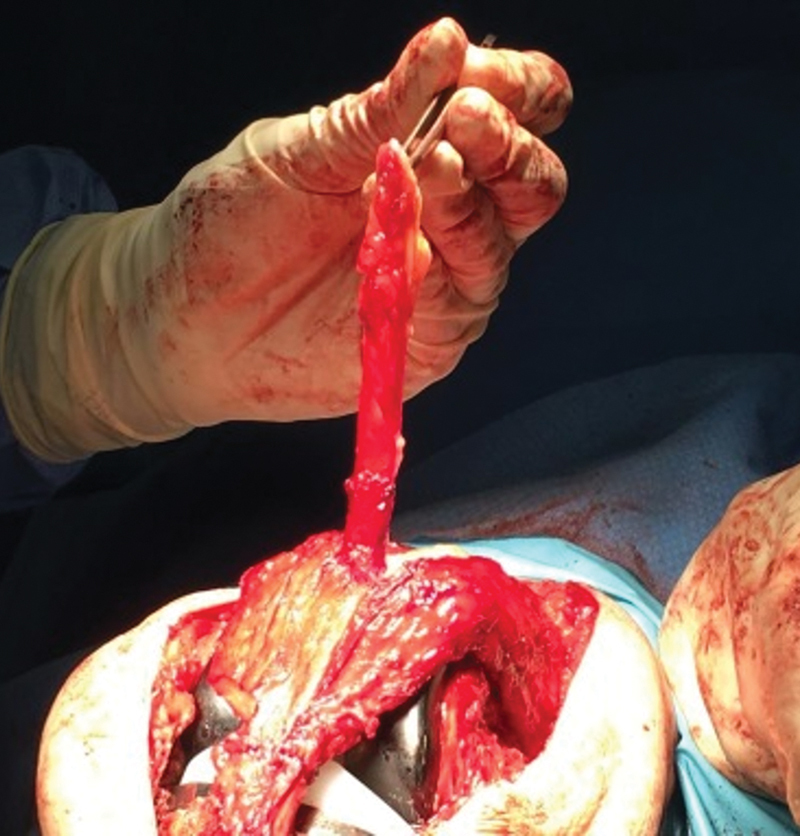 Fig. 5
Fig. 5 Fig. 6
Fig. 6 Fig. 7
Fig. 7Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLower Extremity Biomechanics and Pathologies · Sports injuries and prevention · Foot and Ankle Surgery
Introduction
Patella baja is a pathology defined as the decrease in the distance between the inferior apex of the patella and the proximal articular surface of the tibia, in a patient with symptoms of gonalgia and mobility deficit. 1 2 3 4 5
It is associated with chronic gonalgia, mechanical conflict of the patella, quadriceps muscle insufficiency and decreased range of motion. 1 2 3 4 5 6 7 8 9
Key anatomopathological findings are shortening and increase in ligament thickness, intra-articular fibrosis and Hoffa's fat, tissue retraction and weakness or dysfunction of the quadriceps muscle. 1 2 3 4 5 6 7 8 9
There are several radiological methods to assess patellar height: Insall-Salvati ratio, Blackburne-Peel index and Caton-Deschamps index. 1 4 5 In describing this case, the authors used the Caton-Deschamps index, with values < 0.6 indicating the existence of patella baja. 1 4 5 7
Both surgical procedures and trauma and knee immobilization predispose to the development of patella baja. 1 2 3 4 5 6 7 8 Recent studies show incidence rates of patella baja after total knee arthroplasty of up to 38%. 1 4 7 8 9 This high incidence rate is due to excessive excision of Hoffa's fat, aggressive manipulation of the patellar ligament and release of the lateral patellar retinaculum, which in turn lead to ischemic phenomena, anomalous scarring and tendinous retraction. 1 2 3 7 8 9
There are multiple surgical procedures described for the treatment of this pathology with an impact on blood supply, on the vector of forces and on patellar tilt, with the aim of correcting the underlying etiology and recovering the normal height of the patella, but none is the standard treatment. 1 2 3 6 8 9 The objective of this clinical case was to describe a surgical technique used to correct the shortening and thickness of the patellar ligament.
Case Report
A 73-year-old patient presented with knee stiffness with flexion deficit and, radiologically, patella baja after total arthroplasty of the right knee. The functional limitation, according to the Lysholm Knee Score, was 16 points, with a maximum flexion of 45°, pain and weakness of the extensor apparatus, being resistant to conservative treatment. Initially, the Caton-Deschamps index was 0.49 ( Fig. 1 ).
Lateral radiograph of the knee showing the preoperative Caton-Deschamps index 0.49.
Surgical Technique and Rehabilitation
The patient underwent a combined surgical procedure of patellar ligament repair for lengthening and reinforcement with part of the quadriceps tendon. The polyethylene on the upper articular surface of the tibia was replaced with a thinner one, and the patellar component was removed.
As the patellar ligament thickened, the technique involved dividing the ligament in its thickness, obtaining an anterior and a posterior component of equal thickness. 6 The anterior component was detached, distally, at the level of the anterior tibial tuberosity, and the posterior component, proximally, at the level of the patella 6 ( Fig. 2 ). With the knee at 90° of flexion, the two ligament ends were fixed with at least 5mm of overlap with absorbable suture 6 ( Figs. 3 and 4 ). A bundle of the superficial quadriceps tendon, approximately 1cm wide and 10cm long, was isolated ( Fig. 5 ) and mobilized distally to reinforce the patellar ligament 6 ( Fig. 6 ). Quadriceps excision site was reinforced with absorbable sutures, presenting low morbidity. 6
Scheme of the surgical procedure: patellar ligament was divided in two, according to its thickness. The anterior bundle (dark blue) was detached anteriorly at the level of the anterior tibial tuberosity, the posterior bundle (light blue) was detached at the level of the distal apex of the patella. Also note the acquisition of a bundle of the quadriceps tendon (gray). (1–Quadriceps Tendon; 2–Patella; 3–Patellar Ligament).
Scheme of the surgical procedure: suture of the two bundles of the patellar ligament (dark blue and light blue), with at least 5 mm of overlap. Note the ligament reinforcement with a quadriceps tendon bundle (dark grey). (1–Quadriceps Tendon; 2–Patella; 3–Patellar Ligament)
Intraoperative image demonstrating the suture of the two bundles of the patellar ligament, with at least 5mm of overlap.
Intraoperative image demonstrating mobilization of the quadriceps tendon bundle.
Intraoperative image demonstrating reinforcement of the patellar ligament with a quadriceps tendon bundle. (yellow arrow)
During the first month, immediate mobilization and rehabilitation treatment were necessary to strengthen the quadriceps and prevent relapse of the patella baja, being limited to partial load and maximum flexion of 45°. 6 9 Muscle strengthening and joint rehabilitation was maintained with the support of physical medicine and rehabilitation for three months. At six months of follow-up, the functional results were excellent, with functional results of Lysholm Knee Score of 81 points, maximum flexion of 110° and Caton-Deschamps index of 1.17 ( Fig. 7 ). The patient resumed her daily activities after the first month after the surgery.
Lateral radiograph of the knee showing a Caton-Deschamps index of 1.17 postoperatively.
Discussion
Patella baja is a devastating complication of knee trauma or surgery, and early diagnosis and treatment are essential for the best functional outcome. 1 2 3 4 5 6 7 8
There are several surgical techniques described for correction of soft and bony parts, however there is no standard treatment for this pathology. 1 2 3 6 8 9
Proximal mobilization of the anterior tibial tuberosity restores patellar height, but is not recommended when there is quadriceps muscle dysfunction and does not correct the shortening and thickness of the patellar ligament. 1 2 3 4 5 6 9 10
There are, however, several options for stretching the patellar ligament, such as the use of autologous grafts or allografts from the hamstring tendons or bone-tendon-bone and stretching of the patellar ligament using the Ilizarov technique. 1 2 3 4 5 6 7 8 9 10 More recently, modified Z-plasty has been described, which has some advantages compared to other techniques. 3 4 5 6 7 9
Modified Z-plasty has the advantages of obtaining greater elongation and maintenance of alignment of tendon fibers, keeping the vector of forces and blood vascularization unaltered. 6 Other advantages of this surgical technique are the prevention of subcutaneous and tendon defects, which leads to a lower risk of complications and early rehabilitation. 6
According to the existing literature, the clinical result of the presented patient is similar to other Z-plasty variants, with the advantage of maintaining the alignment of tendinous fibers and greater overlap between the two ligament tops, not altering the vector of forces and reducing the risk bankruptcy. 1 2 3 4 5 6 7 8 9 10 Compared to bone procedures, the surgical approach is less aggressive, rehabilitation and mobilization are earlier, and it also presents a lower risk of failure. 1 2 3 4 5 6 7 8 9 10
There are several surgical techniques for the treatment of patella baja, however there is no standard treatment. The surgical technique presented has the advantages of approaching the underlying pathology, ease of execution and reproducibility, mobilization, recovery and return to daily activities after the first month after surgery, as described in the case presented.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lum Z C Saiz A M Pereira G C Meehan J P Patella Baja in Total Knee Arthroplasty J Am Acad Orthop Surg 2020280831632331934927 10.5435/JAAOS-D-19-00422 · doi ↗ · pubmed ↗
- 2Kennedy M I Aman Z De Phillipo N N La Prade R F Patellar Tendon Tenotomy for Treatment of Patella Baja and Extension Deficiency Arthrosc Tech 2019803 e 317e 32031016128 10.1016/j.eats.2018.11.010PMC 6475627 · doi ↗ · pubmed ↗
- 3Schmidt S Mengis N Rippke J N Zimmermann F Milinkovic D D Balcarek P Treatment of acquired patella baja by proximalization tibial tubercle osteotomy significantly improved knee joint function but overall patient-reported outcome measures remain diminished after two to four years of follow-up Arch Orthop Trauma Surg 2022142102481248733730219 10.1007/s 00402-021-03863-7 · doi ↗ · pubmed ↗
- 4Moulton L S Davies A P Management of extreme patella baja using in-situ hamstring tendon autograft Knee 2014210591691925002139 10.1016/j.knee.2014.06.002 · doi ↗ · pubmed ↗
- 5Salem K H Sheth M R Variables affecting patellar height in patients undergoing primary total knee replacement Int Orthop 202145061477148233277664 10.1007/s 00264-020-04890-6PMC 8178142 · doi ↗ · pubmed ↗
- 6Bruhin V F Preiss S Salzmann G M Harder L P Frontal Tendon Lengthening Plasty for Treatment of Structural Patella Baja Arthrosc Tech 2016506 e 1395 e 140028149738 10.1016/j.eats.2016.08.004PMC 5263852 · doi ↗ · pubmed ↗
- 7Fiquet C White N Gaillard R Servien E Neyret P Lustig S Combined Patellar Tendon lengthening and partial Extensor Mechanism Allograft reconstruction for the treatment of patella infera: A case report Knee 2019260251552030712961 10.1016/j.knee.2018.12.012 · doi ↗ · pubmed ↗
- 8Perelli S Ibañez M Morales-Marin C Patellar Tendon Lengthening: Rescue Procedure for Patella Baja Arthrosc Tech 2019901 e 1e 832021766 10.1016/j.eats.2019.08.012PMC 6993128 · doi ↗ · pubmed ↗