Conservative Approach to Type III Ulnar Club Hand: Case Report
Gabriel Chartuni Teixeira Cury, Leonardo Álaf Lucinda de Sá, Cler David Oliveira, Nathália Vieira Caires, Arnaldo Gonçalves de Jesus Filho, Bruno Gonçalves Schroder e Souza

TL;DR
A 6-year-old boy with severe ulnar club hand improved through conservative physical therapy, showing functional gains without surgery.
Contribution
Demonstrates successful conservative management of type III ulnar club hand through physical therapy and long-term follow-up.
Findings
Conservative physical therapy improved strength and functional skills in a type III ulnar club hand case.
Outpatient follow-up until skeletal maturity is essential to monitor for potential surgical needs.
Patients with severe ulnar dysplasia can achieve daily life functionality through rehabilitation.
Abstract
Ulnar club hand is a rare condition of the upper limbs, for which treatment depends on the degree of morphological and functional impairment, correlating with the radiographic classification of Dobyns, Wood, and Bayne. The aim of the present study is to report a case of a 6-year-old male patient, followed up for type III ulnar club hand (total ulnar dysplasia). Despite the initial difficulty of manipulating objects and performing everyday tasks, conservative physical therapy treatment provided strength gain and development of functional skills for daily life. We conclude that patients with type III deformity can be properly managed with rehabilitation although they require outpatient follow-up until skeletal maturity is reached, as dynamic deformities and new functional limitations may lead to need for corrective surgeries. A mão torta ulnar é uma rara afecção de membros superiores,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
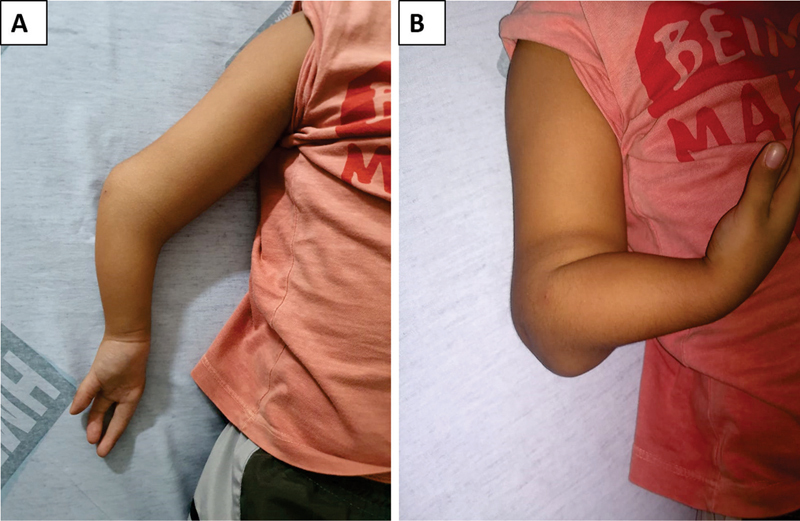 Fig. 1
Fig. 1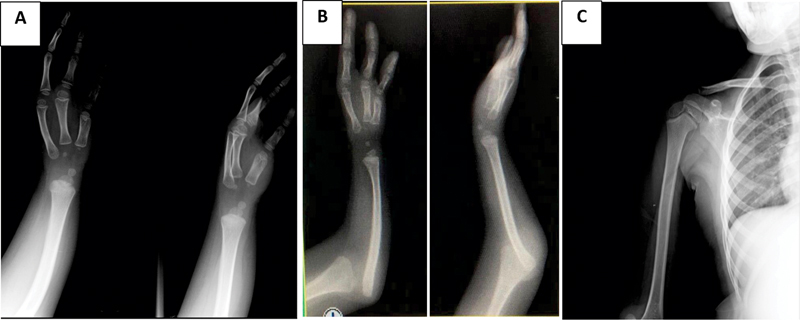 Fig. 2
Fig. 2 Fig. 3
Fig. 3| 1. Strengthening of the right upper limb using a 0.5 kg shin force associated with the ball throwing activity, using an elastic band; |
| 2. Strengthening of the phalanges of the right radiocarpic joint using wax mass, exercises for fingers and hands and rubber ball; |
| 3. Strengthening of periscapular muscles associated with playful activities; |
| 4. Joint mobilization of the scapular and glenohumeral; |
| 5. Osteokinematic mobilization of the glenohumeral with assisting scapular; |
| 6. Motor coordination training (learning to use phalanges individually); |
| 7. Training function (tie shoelace, get dressed, open bottle). |
| Before physical therapy | After physical therapy | |
|---|---|---|
|
| Limitation of the use of individual phalanx in the right hand | Acquisition of the ability to use individual phalanx (muscle strength: grade 4/5) |
|
| Right upper limb hypotonia | Maintained |
|
| Patient could feed himself | Maintained |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital limb and hand anomalies · Neurogenetic and Muscular Disorders Research · Orthopedic Surgery and Rehabilitation
Introduction
Ulnar club hand (UCH) is a rare congenital condition. 1 In Brazil, an incidence of 1.6% of UCH was reported. 2 This is one of the rarest congenital deformities of the upper limbs. 2
Ulnar club hand is a longitudinal failure in the formation of the ulna (phocomelia), which may be totally or partially absent. 3 It is more frequent in men, on the right side, and unilateral in 70% of cases. The incomplete form is the most common. 4
The deformity is characterized by the forearm being short and curved to the radial side, with the hand diverted in the ulnar direction. 4 Other associated abnormalities may be present. 4 The elbow function may be compromised to different degrees (from stiffness to increased mobility, with instability). 1 5 In older children, dislocation of the radial head may occur. 1
Dobyns, Wood, and Bayne rank this condition in four types. In type I, there is ulna hypoplasia, small ulnar deviation, radio arching, and no anlage. In type II, there is partial dysplasia of the ulna (middle or distal third), the proximal joint of the ulna with the humerus is present, there is distal anlage and dislocation of the head of the radius. In type III, total dysplasia of the ulna occurs, there is no anlage, the radio is arched, and the head of the radio is dislocated (with elbow instability). In type IV, there is radio-humeral synostosis and anlage is usually present. 6
The objective of the present study is to present a case of type III UCH, in which the challenge was the choice of treatment. We discuss the elements that guide the therapeutic indication, those related to clinical follow-up, and present the functional results after 2 years of follow-up.
Case Report
A 4-year-old male patient was admitted to a specialized outpatient clinic due to malformation of the right upper limb (RUL). The diagnosis of UCH had been performed by morphological ultrasound and confirmed after birth. In addition to UCH, left testicular agenesis was diagnosed. There was a family history of type III spinal muscular atrophy (paternal). This study was approved by the CEP (CAAE:97048518.9.0000.5103).
A typical deformity of UCH associated with agenesis of the fourth and fifth chirodactyls was evident ( Fig. 1 ). It was not possible to identify formation of fibrous or cartilaginous bar (anlage). There was important functional limitation and difficulties in manipulating objects as well as hypoesthesia at the medial edge of the third finger.
Ectoscopy of the deformity. (A) Anterior face of the member. (B) Profile with bending.
Radiographs ( Fig. 2 ) showed complete absence of ulna, dislocation of the head of the radio and centralized carpal bones. There was no glenohumeral dysplasia on the shoulder.
(A) Ulnar club hand type III of Dobyns, Wood, and Bayne – Total dysplasia of the ulna and absence of 4th and 5th right chirodactyls, and their respective metacarpals with preserved joint relationship. (B) Dislocation of the radio head. (C) Absence of deformities of the proximal humerus.
Given the limitations for daily life, the patient visited our outpatient clinic, where he received indication for physical therapy treatment. The goal was to optimize fine motor activity and functional gain (such as using the cell phone, getting dressed independently and putting on shoes). The treatment was performed for 9 months (1 hour, 3 times a week) ( Chart 1 ).
Chart 1: Physiotherapeutic procedures performed by the patient during the physiotherapy period
The result of physical therapy was measured by the goal attainment scale (GAS) 7 , which included three tasks agreed on by family members and therapists. The objectives were: to improve the functionality of the RUL with gain of fine movements; to improve the palmar grip; to reduce scapular dyskinesia during abduction to pick up a toy on the shelf. At 2 months, the patient showed improvement in 2 tasks (video-compared RUL function and improvement of palmar grip in daily tasks).
In the consultation after physical therapy, we applied the disabilities of the arm, shoulder and hand (DASH) questionnaire. 8 As the patient was a child, questions 7, 8, 12 and 21 could not be applied because they addressed typical adult functions. This modification led us to consider not the absolute score (38.33 points), but its weighted value (46%), classifying the dysfunction as moderate. Chart 2 lists other findings.
Chart 2: Activity assessment before and after physiotherapy
The patient maintains follow-up after 2 years, asymptomatic and with stable condition, performs the movement of thumb tweezers, despite not presenting function of the opponent muscles. The flexor musculature of the three fingers is normal, o the patient is able to play with the cell phone, dress independently and perform other daily tasks ( Fig. 3 ). We chose not to indicate surgery at this time, although the approach can be reviewed, especially if there is loss of thumb tweezer ability, worsening of elbow stability, progressive loss of function, or pain.
Illustrative images of limb functionality using electronic device and demonstrating clamp function.
Discussion
Our case is illustrative of UCH because it includes a male patient and involvement of the right side. 4 In the literature, partial ulna agenesis (Bayne II) is the most frequent phenotype, which is different from our case. 1 5 6 We did not identify cases similar to ours in the national literature.
The agenesis of metacarpals and phalanges observed is also reported in most studies. 1 5 We did not identify concomitant musculoskeletal abnormalities or limitation of elbow mobility, unlike other authors. 5 6
The treatment in cases of UCH requires a multi-professional and individualized approach. 9 Most children are treated without surgery, especially in unilateral UCH. 9 In cases requiring surgery, the goal is to improve the function of the affected limb. 9
To evaluate the gain of function, we can use objective scales (e.g. DASH) or other more subjective scales (e.g.: GAS). Although validated, the DASH questionnaire has disadvantages because it involves a longer period of application and is specific to adults. Therefore, GAS is preferred by us, because it is more practical. It involves defining a set of objectives and specifies a range of possible outcomes for each objective (on a scale that contains 5 levels, from -2 to +2). It is used to evaluate performance after a specified intervention period. 7
The surgical approach in the cases of Bayne II was advocated by Monteiro and Schachinger. 1 5 In patients with Bayne IV, conservative treatment is recommended. 10 We did not identify recommendations for Bayne III. In this case, conservative treatment was chosen due to the patient's age and good response to physiotherapy with adequate adaptation to day-to-day activities.
The prognosis of UCH will depend on factors such as: unilateralism, association with syndromes, the number of fingers present, the degree of atrophy of the limbs, and the presence of sindactyly. 9 In our case, the function of the elbow and wrist joints may worsen with growth, which justifies serial follow-ups and eventual interventions. 1 However, the follow-up of the last 2 years showed satisfactory developments.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Monteiro A V Chiconelli J R Deficiência ulnar congênita: conduta de tratamento Rev Bras Ortop 19973208637640
- 2Pinto H B Pais A P Vitorio S C Brandão R Moreira A AD Molinaro L R Case Study of Congenital Anomalies of the Upper Limb in Reference Ambulatory Care Facility Acta Ortop Bras 2018260532532730464714 10.1590/1413-785220182605197649 PMC 6220662 · doi ↗ · pubmed ↗
- 3Swanson A BA classification for congenital limb malformations J Hand Surg Am 19761018221021591 10.1016/s 0363-5023(76)80021-4 · doi ↗ · pubmed ↗
- 4Panda A Gamanagatti S Jana M Gupta A K Skeletal dysplasias: A radiographic approach and review of common non-lethal skeletal dysplasias World J Radiol 201461080882525349664 10.4329/wjr.v 6.i 10.808PMC 4209426 · doi ↗ · pubmed ↗
- 5Schachinger F Girsch W Farr S Soft-Tissue Distraction Prior to Single Bone Forearm Surgery in Ulnar Longitudinal Deficiency: A Report of Two Cases J Hand Surg Asian Pac Vol 2018230115315729409418 10.1142/S 2424835518720116 · doi ↗ · pubmed ↗
- 6Bayne L G Ulnar club hand (Ulnar deficiencies)New York Churchill Livingstone 1993288303
- 7Mc Dougall J Wright V The ICF-CY and Goal Attainment Scaling: benefits of their combined use for pediatric practice Disabil Rehabil 200931161362137219340620 10.1080/09638280802572973 · doi ↗ · pubmed ↗
- 8Orfale A G Araújo P M Ferraz M B Natour J Translation into Brazilian Portuguese, cultural adaptation and evaluation of the reliability of the Disabilities of the Arm, Shoulder and Hand Questionnaire Braz J Med Biol Res 2005380229330215785841 10.1590/s 0100-879x 2005000200018 · doi ↗ · pubmed ↗