Absence of Pericarditis Recurrence in Rilonacept-Treated Patients With COVID-19 and SARS-CoV-2 Vaccination: Results From the RHAPSODY Long-term Extension
Antonio Brucato, Lucia Trotta, Michael Arad, Paul C. Cremer, Antonella Insalaco, Marc Klutstein, Martin LeWinter, David Lin, Sushil A. Luis, Yishay Wasserstrum, JoAnn Clair, Sheldon Wang, Allan L. Klein, Massimo Imazio, John F. Paolini, Antonio Abbate, Antonio Abbate

TL;DR
Rilonacept treatment prevents pericarditis recurrence even during or after SARS-CoV-2 vaccination or mild to moderate COVID-19 infection.
Contribution
Demonstrates that rilonacept should be continued during SARS-CoV-2 vaccination or infection to prevent pericarditis recurrence.
Findings
No pericarditis recurrences were observed in patients vaccinated against SARS-CoV-2.
Continued rilonacept treatment during or after mild/moderate COVID-19 did not worsen disease severity.
Stopping rilonacept increased pericarditis recurrence risk.
Abstract
Rilonacept inhibits the interleukin-1 pathway, and extended treatment in patients with recurrent pericarditis (RP) reduced recurrence risk by 98% in the phase 3 trial, RHAPSODY long-term extension (LTE). Severe acute respiratory syndrome (SARS)-CoV-2 vaccination and/or infection may trigger pericarditis recurrence, and in clinical practice, it is unknown whether to continue rilonacept during SARS-CoV-2 infection. This post-hoc analysis of the RHAPSODY LTE aimed to inform rilonacept management in RP patients vaccinated against SARS-CoV-2 or who contract COVID-19. Analysis was conducted from May 2020 to June 2022. The LTE portion of RHAPSODY LTE enabled up to 24 months of additional open-label rilonacept treatment beyond the pivotal study. Rilonacept efficacy data in preventing pericarditis recurrence were assessed, and concomitant SARS-CoV-2 vaccination and COVID-19 adverse event data…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
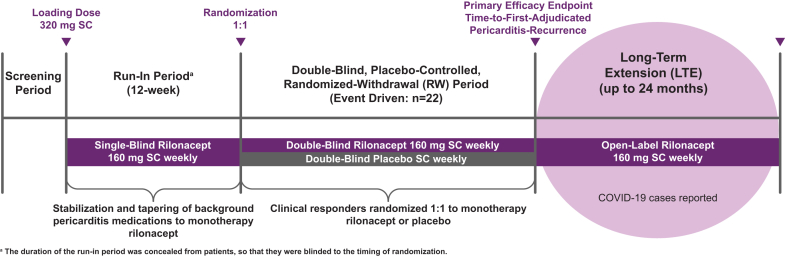 Figure 1
Figure 1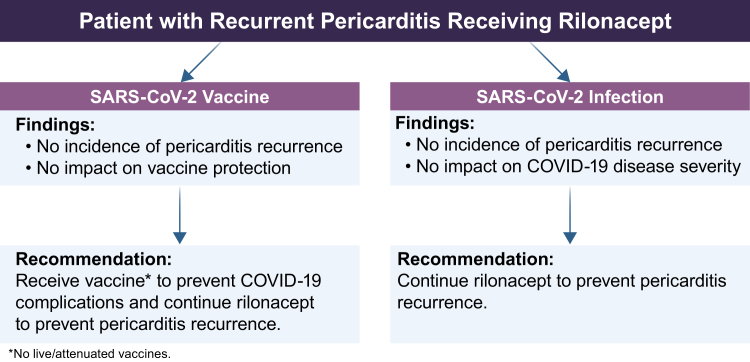 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSpanish Culture and Identity · Youth Culture and Social Dynamics
Recurrent pericarditis (RP) is a chronic autoinflammatory disease of 3-year median duration requiring prolonged treatment to prevent recurrence.1, 2, 3 The interleukin-1 (IL-1) cytokine family dominates the inflammatory response in RP, and IL-1 pathway inhibition reduces recurrence risk in patients with RP.4 Rilonacept reduced pericarditis recurrence risk by 96% (hazard ratio in a Cox proportional-hazards model, 0.04; 95% confidence interval, 0.01-0.18; P < 0.0001 by log-rank test) in the phase-3 study Rilonacept Inhibition of Interleukin-1 Alpha and Beta for Recurrent Pericarditis: a Pivotal Symptomatology and Outcomes Study (RHAPSODY).5 The RHAPSODY long-term extension (LTE) results showed persistent (98%) risk reduction, whereas premature rilonacept cessation increased recurrence risk.6
The RHAPSODY LTE took place during the peak of the COVID-19 pandemic. Although COVID-19 was not a primary study outcome, it provided a valuable opportunity for gaining additional on-treatment efficacy and safety insights regarding RP relating to severe acute respiratory syndrome (SARS)-CoV-2 vaccination and COVID-19 infection, refining clinical decision-making regarding rilonacept therapy under these circumstances.
Methods
Study design and patients
This was a post-hoc analysis of 74 patients between 12 and 75 years of age participating in the 24-month open-label RHAPSODY LTE (NCT03737110),5 conducted from May 2020 to June 2022 (Fig. 1) in 4 countries (n = 45 in the US; n = 29 in Italy, Israel, and Australia). A total of 69 patients completed the RHAPSODY LTE (27 [39.1%] male, 42 [60.9%] female): US sites concluded in April 2021 after approval of rilonacept for use in RP by the US Food and Drug Administration; non-US patients remained until study closure (June 2022).Figure 1Rilonacept Inhibition of Interleukin-1 Alpha and Beta for Recurrent Pericarditis: a Pivotal Symptomatology and Outcomes Study (RHAPSODY) long-term extension (LTE) design—a phase 3, double-blind, placebo-controlled, event-driven, randomized-withdrawal (RW) trial of rilonacept in patients with recurrent pericarditis, which also included a long-term extension phase, allowing up to 24 months of additional open-label rilonacept treatment. SC, subcutaneous.
SARS-CoV-2 vaccines became available in November 2020. The vaccine series type was recorded as concomitant medication. COVID-19 complications were recorded as adverse events and were classified by investigators as mild, moderate, or severe, according to the US Food and Drug Administration adverse-event reporting guidelines.7 COVID-19 diagnoses were not adjudicated, and the disease detection method was not reported.
Outcome measures
Outcome measures included pericarditis recurrences in the setting of SARS-CoV-2 vaccine and COVID-19 cases related to clinical management.
Statistical analysis
Due to the small sample size and the unplanned pandemic, descriptive summary statistics are provided (n, mean, standard deviation [SD]), using SAS version 9.4 (SAS Institute, Cary, NC).
Results
Study population
In total, 74 RHAPSODY patients commenced the LTE (mean [SD] age, 44.2 [15.6] years; 40 women [54.1%] and 34 men [45.9%]; 68 [91.9%] White, 5 [6.8%] Black/African American, and 1 [1.4%] other). Mean RP disease duration at study entry was 2.5 years. Sixty-nine patients completed the RHAPSODY LTE; overall median (maximum) treatment duration was 22 (35) months. In April 2021, after rilonacept approval in the US for treatment of RP and after the US sites concluded, 32 of 45 US patients (71.1%) transitioned to commercial rilonacept after a median (maximum) 18 (27)-month treatment duration. Twenty-five non-US patients remained on rilonacept until study closure (through a 6-week safety follow-up) in June 2022 after a median (maximum) 28 (35)-month treatment duration.
SARS-CoV-2 vaccination
During the RHAPSODY LTE while on study treatment, 47 of 74 patients (63.5%) received at least 1 SARS-CoV-2 vaccine (no live-attenuated; messenger [m]RNA [n = 34], adenovirus [n = 2], and “unknown” [n = 11]); 44 of 74 (59.5%) were considered fully vaccinated (received a complete vaccine series), and 30 of 74 (40.5%) were partially vaccinated or unvaccinated.
COVID-19 incidence
No COVID-19 cases were reported during the randomized-withdrawal period (ended May 2020). A listing of prevalent SARS-CoV-2 variants during the conduct of the RHAPSODY LTE is found in Supplemental Table S2.8 A COVID-19 adverse event was reported in 16 of 74 patients (21.6%). COVID-19 cases were reported in 10 of 30 unvaccinated or partially vaccinated patients (33%; 13.5% of total enrollment) and in 6 of 44 fully vaccinated patients (14%; 8.1% of total enrollment). Among the 6 COVID-19 cases reported in fully vaccinated patients, 1 occurred about 11 months after, and a second case 14 months after, completion of the vaccine series (Supplemental Table S3).
COVID-19 severity and rilonacept treatment
COVID-19 severity was mild (n = 13), moderate (n = 2), or severe (n = 1). Twelve infected patients (75%) were receiving rilonacept at the time of COVID-19 diagnosis; 4 (25%) were off-treatment, 2 had previously “suspended” rilonacept for off-treatment observation at the 18-month decision milestone, and 2 were in the 6-week safety follow-up period after having discontinued treatment. Of those patients receiving rilonacept at the time of COVID-19 diagnosis, 10 of 12 (83.3%) continued rilonacept, 1 of 12 (8.3%) interrupted rilonacept for 4 weeks, and 1 of 12 (8.3%) permanently discontinued rilonacept. COVID-19 resolved in all but the 1 patient who permanently discontinued rilonacept; this patient had a prolonged severe COVID-19 course complicated by preexisting comorbidities.
Pericarditis recurrence outcomes
Among the 12 of 16 patients (75%) receiving rilonacept at the time of infection, no patients (0 of 12) experienced a pericarditis recurrence during or after the COVID-19 adverse event. Of the 2 of 16 patients (12.5%) who had previously “suspended” rilonacept for off-treatment observation at the 18-month decision milestone, 1 investigator-assessed pericarditis recurrence (without C-reactive protein elevation) occurred in the peri-COVID-19 period (18 days after infection), approximately 4.5 months after rilonacept cessation. No pericarditis recurrences were reported in the 2 of 16 patients (12.5%) whose COVID-19 cases occurred after the end of rilonacept treatment visits and during the 6-week safety follow-up period (Table 1). Among the 58 of 74 patients (78%) without a COVID-19 infection, no pericarditis recurrences were temporally associated with SARS-CoV-2 vaccination.Table 1. Severe acute respiratory syndrome (SARS)-CoV-2 infections grouped by vaccination status and whether patients were receiving rilonacept at the time of infection; pericarditis recurrences are also reportedSeverityPatients with COVID infection, n = 16Vaccinated n = 6 (37.5%)Partially vaccinated or unvaccinated n = 10 (62.5%)Total n = 16 (100%)Mild, n = 135 of 6 (83.3)8 of 10 (80.0)13 of 16 (81.3)Moderate, n = 21 of 6 (16.7)1 of 10 (10.0)2 of 16 (12.5)Severe, n = 101 of 10 (10.0)1 of 16 (6.3)On rilonacept, n = 125 of 67 of 1012 of 16 (75.0) Mild, n = 94 of 5 (80.0)5 of 7 (71.4)9 of 12 (75.0) Moderate, n = 21 of 5 (20.0)1 of 7 (14.2)2 of 12 (16.7) Severe, n = 101 of 7 (14.2)1 of 12 (8.3) Pericarditis recurrence000Off rilonacept, n = 41 of 63 of 104 of 16 (25.0) Mild, n = 41 of 1 (100)∗3 of 3 (100)4 of 4 (100) Moderate, n = 0000 Severe, n = 0000 Pericarditis recurrence01 of 3 (33.3)†1 of 4 (25.0)Values are n (%).∗COVID-19 adverse event was reported during the safety follow-up period, 1 month after the patient had stopped rilonacept treatment.†One pericarditis recurrence (without C-reactive protein elevation) occurred in the peri-COVID-19 period (18 days after infection), approximately 4.5 months after rilonacept cessation.
Discussion
RP is a chronic condition, and physicians commonly must decide how to manage treatments during intercurrent events, such as infections or vaccinations, particularly when biologics agents are used. Use of an anti–IL-1 agent during COVID-19 and/or other infections could be useful, and the interruption of the drug might facilitate a recurrence of pericarditis. The RHAPSODY LTE took place during the height of the COVID-19 pandemic, providing the opportunity to study rilonacept use in patients with RP who were vaccinated against SARS-CoV-2 and/or contracted COVID-19.
We observed that rilonacept did not appear to interfere with the protective effect of SARS-CoV-2 vaccination; as expected, patients who were fully vaccinated experienced a lower incidence of COVID-19, compared to patients who were unvaccinated or partially vaccinated in the setting of rilonacept treatment.9
An inappropriate and exuberant innate immune response contributes to COVID-19 morbidity, and higher levels of proinflammatory cytokines, including IL-1ß, are associated with more severe disease.10 Inhibition of IL-1 signaling reduced mortality and the need for invasive mechanical ventilation among patients hospitalized with COVID-19.11 In line with these observations, we found that rilonacept treatment did not appear to impact the safety of patients with COVID-19.
Similar to other viruses, SARS-CoV-2 may retrigger autoinflammatory processes that contribute to pericarditis recurrence. Among patients participating in the RHAPSODY LTE, premature cessation of rilonacept led to pericarditis recurrences, regardless of COVID-19 or vaccination status.
Limitations
The descriptive analyses reported here were not prespecified, because of the unpredictable circumstances of the pandemic. The sample size related to vaccination and infection was small (44 patients were fully vaccinated, 30 patients were partially vaccinated or unvaccinated; 16 SARS-CoV-2 infections reported), and the cohort was not randomized. Administration of Paxlovid and the presence of anti-SARS-CoV-2 monoclonal antibodies were not captured in this study. Recurrences were investigator-assessed and were not externally adjudicated.
Conclusions
In this size-limited analysis, rilonacept did not appear to interfere with SARS-CoV-2 vaccine protection. The results suggest that patients with RP being treated with rilonacept should receive a SARS-CoV-2 vaccination series to reduce possible complications from COVID-19. Continued rilonacept treatment during COVID-19 was well tolerated, supporting a recommendation that RP patients should continue rilonacept regardless of COVID-19 status to prevent pericarditis recurrence (Fig. 2). The data presented support the further study of the relationships among RP, vaccination, and infection in the setting of anti-IL-1 therapies.Figure 2. Summary of post-hoc analysis findings and clinical recommendations rubric. Among patients on rilonacept in the Rilonacept Inhibition of Interleukin-1 Alpha and Beta for Recurrent Pericarditis: a Pivotal Symptomatology and Outcomes Study (RHAPSODY) long-term extension (LTE) (n = 74), no pericarditis recurrences were associated temporally with severe acute respiratory syndrome (SARS)-CoV-2 vaccination, and no impact on vaccine protection was observed. After SARS-CoV-2 infection, no patients had a pericarditis recurrence, and it had no impact on COVID-19 severity. It is recommended that patients with recurrent pericarditis receiving rilonacept receive a SARS-CoV-2 vaccine and continue rilonacept to prevent pericarditis recurrence.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Imazio M.Idiopathic recurrent pericarditis as an immune-mediated disease: current insights into pathogenesis and emerging treatment options Expert Rev Clin Immunol 102014148714922530799510.1586/1744666 X.2014.965150 · doi ↗ · pubmed ↗
- 2Klein A.Cremer P.Kontzias A.US database study of clinical burden and unmet need in recurrent pericarditis J Am Heart Assoc 102021 e 01895010.1161/JAHA.120.018950 PMC 847569134284595 · doi ↗ · pubmed ↗
- 3Lin D.Laliberte F.Majeski C.Disease and economic burden associated with recurrent pericarditis in a privately insured United States population Adv Ther 382021512751433441772410.1007/s 12325-021-01868-7PMC 8478772 · doi ↗ · pubmed ↗
- 4Del Pinto R.Ferri C.Recurrent pericarditis is less scary: the new therapeutic solutions Eur Heart J Suppl 23Suppl E 2021 E 83E 863465036110.1093/eurheartj/suab 097PMC 8503402 · doi ↗ · pubmed ↗
- 5Klein A.L.Imazio M.Cremer P.Phase 3 study of IL-1 trap rilonacept in recurrent pericarditis N Engl J Med 384202131413320089010.1056/NEJ Moa 2027892 · doi ↗ · pubmed ↗
- 6Imazio M.Klein A.L.Brucato A.Sustained Pericarditis Recurrence Risk Reduction With Long-Term Rilonacept J Am Heart Assoc 1362024 e 03251610.1161/JAHA.123.032516 PMC 1101003938471825 · doi ↗ · pubmed ↗
- 7US Food & Drug Administration FDA Adverse Event Reporting System (FAERS) public dashboard Available at:https://www.fda.gov/drugs/questions-and-answers-fdas-adverse-event-reporting-system-faers/fda-adverse-event-reporting-system-faers-public-dashboard
- 8Institute of Social and Preventive Medicine University of Bern, Switzerland, and SID Swiss Institute of Bioinformatics. Co Variants Available at:https://covariants.org/