Palpebral leishmaniasis
Mohammad Sharifi, Tayebe Shiravi, Ali Bolouki, Mehrdad Motamed Shariati

TL;DR
Leishmaniasis can look like other eye conditions, but the presence of kinetoplasts helps confirm the diagnosis under a microscope.
Contribution
The paper highlights the diagnostic importance of identifying kinetoplasts in leishmaniasis.
Findings
Leishmaniasis can resemble hordeolum or skin cancers clinically.
Microscopic detection of kinetoplasts confirms leishmaniasis diagnosis.
Abstract
Leishmaniasis can mimic many conditions, including hordeolum, basal cell carcinoma, and squamous cell carcinoma. The presence of kinetoplast in free‐form or intramacrophage amastigotes, ensuring us to establish the microscopic diagnosis of leishmaniasis.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
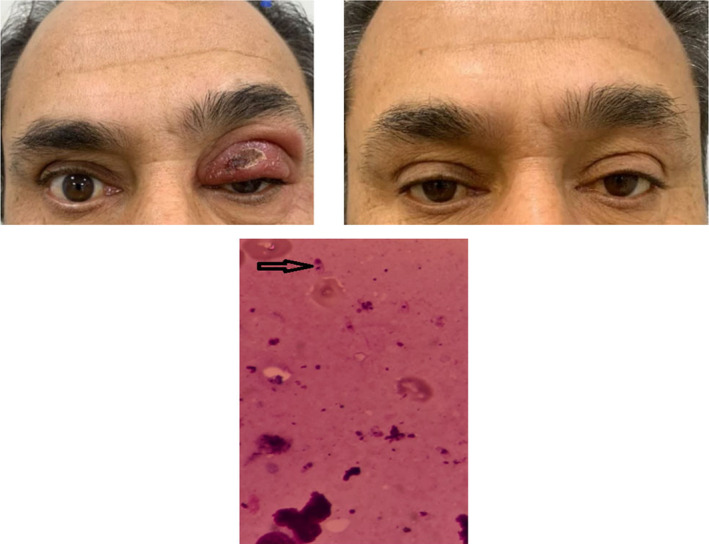 FIGURE 1
FIGURE 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsResearch on Leishmaniasis Studies
CASE PRESENTATION
1
A 50 y/o man presented with a progressive left upper eyelid skin ulcer since 6 months ago. During this period, he received topical and systemic antibiotics with the diagnosis of skin bacterial infection. On the examination, a 10 × 15 mm lesion was observed, which involved the left upper eyelid (Figure 1). Slit lamp examination, fundus examination, and intraocular pressures were unremarkable. Visual acuity was 10/10 in the eyes. Systemic examination excluded lymphadenopathy.
Ocular leishmanial lesion involving the left upper eyelid before the treatment (left upper) and 6 months after treatment (right upper). Direct smear from the skin ulcer shows amastigotes in the cytoplasm of macrophages (lower image, black arrow).
Considering the endemicity of leishmania in the area where the patient lived, Mashhad, we suspected leishmaniasis. A direct smear of the lesion revealed Leishman bodies. Pathology examination showed leishmania organisms within and next to macrophages (Figure 1). Also, we suggested the PCR test. However, the patient refused to do it. The patient was diagnosed with palpebral leishmaniosis and treated with systemic Glucantime (20 mg/kg) daily for 3 weeks. The option of treatment with intralesional injections of meglumine antimoniate was offered to the patient. He refused local treatment.
DISCUSSION
2
Leishmaniasis is classified into Old and New World cutaneous leishmaniasis, mucocutaneous and visceral leishmaniasis. Cutaneous leishmaniasis is characterized by single or multiple ulcerative skin lesions, usually on the face or extremities. Cutaneous leishmaniasis is common in Iran and is usually caused by L. major or L. tropica. Leishmania is transmitted by a sandfly infected with leishmania parasites. Infection of the eyelid is rare because eyelashes and eyelid movements usually prevent the sandfly from biting the skin of there. Adnexal leishmaniosis is a challenging diagnosis in non‐endemic areas and is not accompanied by any cutaneous lesions elsewhere on the body.1
Leishmaniasis can mimic many conditions, including chronic blepharitis, hordeolum, basal cell carcinoma, and squamous cell carcinoma, so we need a high index of suspicion to diagnose it immediately. Palpebral involvement can lead to ectropion and trichiasis, emphasizing early diagnosis and treatment Cutaneous leishmaniasis is usually a self‐limiting disease. However, if left untreated, eyelid leishmaniasis can spread to the conjunctiva and cornea, causing conjunctivitis and interstitial keratitis.2
Treatment of ocular leishmaniasis includes systemic meglumine antimoniate 20 mg/kg for at least 3 weeks and allopurinol. Intralesional meglumine antimoniate can also be used twice weekly for at least 2 weeks. Another choice is paromomycin ointment. Also, intra‐lesion injection of meglumine antimoniate is effective as a systemic treatment but is more effective than paromomycin ointment.3
One of the important points in the mentioned case is the absence of scars after recovery. A scar on the edge of the eyelid can lead to complications such as ectropion and exposure keratopathy.
AUTHOR CONTRIBUTIONS
Mohammad Sharifi: Investigation; writing – review and editing. Tayebe Shiravi: Data curation; writing – original draft. Ali Bolouki: Data curation; writing – original draft; writing – review and editing. Mehrdad Motamed Shariati: Conceptualization; data curation; supervision; writing – original draft; writing – review and editing.
FUNDING INFORMATION
The authors received no funding.
CONFLICT OF INTEREST STATEMENT
The authors declare that they have no competing interests.
CONSENT
Written informed consent was obtained from the patient to publish this report in accordance with the journal's patient consent policy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sadeghian G , Moradi S , Hanjani S . Ocular leishmaniasis: a case report. Dermatol Online J. 2005;11(2):19.16150227 · pubmed ↗
- 2Chu FC , Rodrigues MM , Cogan DG , Neva FA . Leishmaniasis affecting the eyelids. Arch Ophthalmol. 1983;101(1):84‐91.6849660 10.1001/archopht.1983.01040010086015 · doi ↗ · pubmed ↗
- 3Mignot G , Bhattacharya Y , Reddy A . Ocular Leishmaniasis‐a systematic review. Indian J Ophthalmol. 2021;69(5):1052.33913831 10.4103/ijo.IJO_2232_20PMC 8186621 · doi ↗ · pubmed ↗