Salvage circumferential endoscopic submucosal dissection of multifocal Barrett’s adenocarcinoma at an esophagogastric anastomosis
Sunil Gupta, Tony He, Jeffrey D. Mosko, Gary May, Christopher Teshima

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
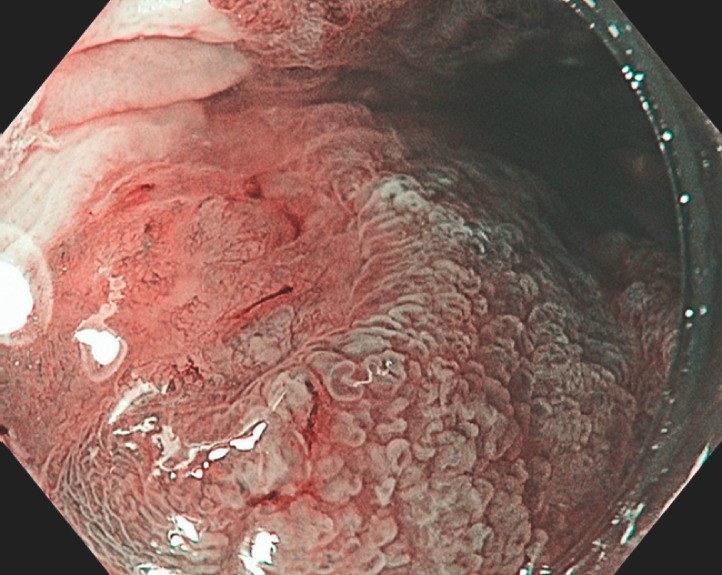 Fig. 1
Fig. 1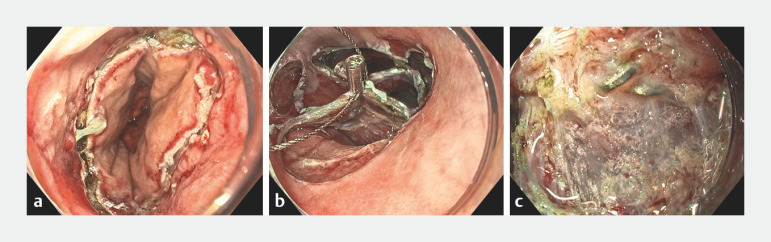 Fig. 2
Fig. 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastric Cancer Management and Outcomes · Esophageal Cancer Research and Treatment · Gastrointestinal Tumor Research and Treatment
A 69-year-old man underwent neoadjuvant chemoradiotherapy and Ivor Lewis esophagectomy with proximal gastrectomy for T3N0M0 esophageal adenocarcinoma. After 6 years, a new positron emission tomography (PET)-avid thickening was detected at the esophagogastric anastomosis. Endoscopy revealed a 3-cm circumferential segment of Barrett’s mucosa extending from the esophagogastric anastomosis into the remnant esophagus. This contained multiple areas of nodularity with irregular pit and vascular pattern that were concerning for multifocal early Barrett’s cancer ( Fig. 1 ). As the patient was not a candidate for further surgery or radiotherapy, we proceeded with salvage circumferential endoscopic submucosal dissection (ESD) ( Video 1 ).
Endoscopic image showing multifocal early Barrett’s adenocarcinoma at the esophagogastric anastomosis.
Salvage circumferential endoscopic submucosal dissection of multifocal Barrett’s adenocarcinoma at the esophagogastric anastomosis in a patient who was not a candidate for further surgery.Video 1
After the distal margin had been marked along the anastomotic line, a circumferential mucosal incision was created ( Fig. 2 a ). Submucosal dissection was then performed, aiming to remain above the surgical staples. Following this, four submucosal tunnels orientated at 12, 3, 6, and 9 o’clock were formed from the proximal to the distal margin. Clip-and-snare traction was used by grasping the 12- and 6-o’clock tunnels together ( Fig. 2 b ). While this facilitated straightforward dissection of the bridging submucosa between the 6- to 9-, 9- to 12-, and 12- to 3-o’clock tunnels, surgical staples embedded within severe fibrosis were encountered between the 3- and 6-o’clock tunnels ( Fig. 2 c ). As this indicated curvilinear proximal extension of the anastomotic line, we aimed to remain below the staples to avoid creating a full-thickness perforation. En bloc resection was achieved with traction assistance and with an occasional underwater approach. An area of muscle injury (10 mm) was closed with through-the-scope clips.
Endoscopic images showing: a the distal mucosal incision; b clip-and-snare traction being used following the creation of four submucosal tunnels; c surgical staples embedded within fibrosis in one of the tunnels.
The final histology revealed R0 excision of a poorly differentiated T1a esophageal adenocarcinoma. Endoscopy at 4 weeks demonstrated healing, with no residual Barrett’s mucosa noted. The patient will be closely monitored with serial imaging, endoscopy, and endoscopic ultrasound examinations 1 .
In nonoperative candidates, salvage ESD of an anastomotic lesion can be a safe and feasible procedure in expert hands. Traction and an underwater approach may assist when encountering areas of fibrosis or surgical staples. Further studies highlighting long-term patient and oncologic outcomes are required.
Endoscopy_UCTN_Code_TTT_1AO_2AG_3AD
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chan MW Nieuwenhuis E Jansen M Endoscopic follow-up of radically resected submucosal adenocarcinoma in Barrett’s esophagus: interim results of an ongoing prospective, International, multicenter cohort registry (PREFER trial)Gastrointest Endosc 202397 AB 1017 AB 1018