Doughnut-shaped endoscopic submucosal dissection for circumferential ileocecal valve adenoma
Yugo Suzuki, Kosuke Nomura, Hanako Inoue, Daisuke Kikuchi, Akira Matsui, Shu Hoteya

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
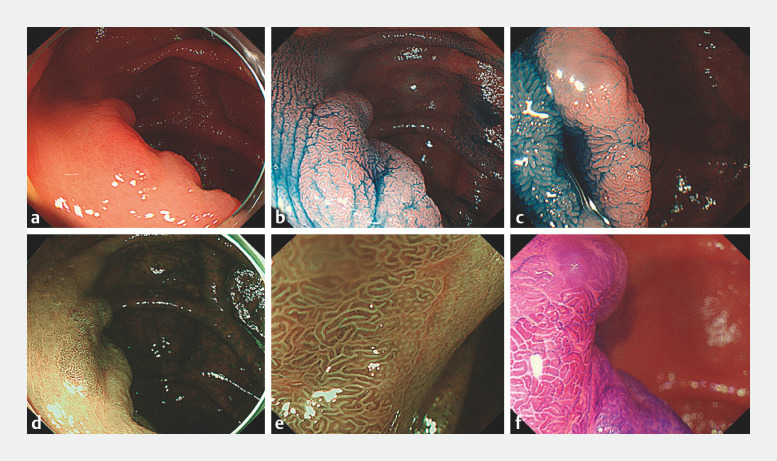 Fig. 1
Fig. 1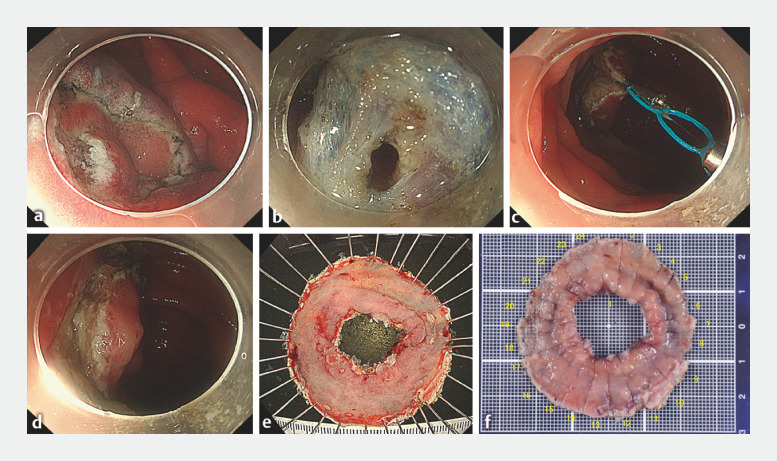 Fig. 2
Fig. 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastric Cancer Management and Outcomes · Metastasis and carcinoma case studies · Esophageal and GI Pathology
Endoscopic submucosal dissection (ESD) has not become established as a standard technique for treatment of ileocecal valve (ICV) lesions, and its efficacy has been reported as limited because of its technical difficulty and the time required 1 2 3 . Regarding circumferential lesions in particular, there have been few reports of treatment with ESD 4 .
A 40-year-old woman with type B cirrhosis and diabetes mellitus underwent screening lower gastrointestinal endoscopy and was found to have a large (30-mm) type 0-IIa lesion extending around the entire circumference of the ICV. The lesion was endoscopically diagnosed as adenoma by narrow-band imaging magnification and chromoendoscopy with crystal violet ( Fig. 1 ). Tissue biopsy confirmed the diagnosis of adenoma, and we performed ESD ( Video 1 ). The ESD procedure was performed using a PCF-H290TI (Olympus, Tokyo, Japan) and DualKnife J (KD-655Q; Olympus). A VIO 300D system (Erbe, Tübingen, Germany) was used as the electrosurgical unit. A multiloop traction device (Boston Scientific, Tokyo, Japan) was used to perform traction from the anorectal side. The lesion was resected en bloc without any adverse events, and histopathology confirmed R0 resection of a large tubular adenoma measuring 30 × 28 mm ( Fig. 2 ).
Pretreatment endoscopic evaluation. a An erythematous 0-IIa lesion is seen at the ileocecal valve. b, c The margin of the 0-IIa lesion is clearly delineated after spraying with 0.4% indigo carmine dye ( b anal side; c cecal side). d Narrow-band imaging (NBI). The lesion appears as a pale brownish area. e Magnifying NBI. A regular surface pattern and vessel pattern are observed; the lesion was diagnosed as Japan NBI Expert Team classification type 2A. f Magnified chromoendoscopy with crystal violet staining showed a type IV pit pattern.
Endoscopic procedure. a Circumferential dissection at the ileal border of the lesion. b Creation of a tunnel. c Attaching the multiloop traction device to the mucosal edge to elevate it. d Endoscopic submucosal dissection ulcer after resection. The lesion was resected en bloc without adverse events. e Doughnut-shaped endoscopic submucosal dissection specimen. The specimen size was 50 × 50 mm. f Pathology showed a tubular adenoma measuring 30 × 28 mm with negative margins.
Successful doughnut-shaped endoscopic submucosal dissection for a circumferential adenoma located at the ileocecal valve.Video 1
Complete resection rates for endoscopic treatment of superficial neoplasms extending into the ileocecal valve are low, and tumor recurrence is consequently a problem 1 . Curative resection by ESD, as in this case, has the major advantages of being less invasive and preserving function. No case of stenosis has been reported for total-circumferential lesions of the ICV among the 9 cases treated with ESD reported to date, including this case 4 5 . The ICV is where the ileal and cecal lumens meet vertically; therefore, the contraction tension during ulcer healing after ESD may radiate outward, which may help stretch the ICV open, without development of stricture 4 .
In conclusion, the doughnut-shaped ESD appears to be a safe, feasible, and effective method for removing circumferential lesions of the ICV.
Endoscopy_UCTN_Code_TTT_1AO_2AG_3AD
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Andrisani G Fukuchi T Antonelli G Superficial neoplasia involving the ileocecal valve: clinical outcomes of endoscopic submucosal dissection Dig Liver Dis 20215388989410.1016/j.dld.2021.03.00533762176 · doi ↗ · pubmed ↗
- 2Ishii N Itoh T Horiki N Endoscopic submucosal dissection with a combination of small-caliber-tip transparent hood and flex knife for large superficial colorectal neoplasias including ileocecal lesions Surg Endosc 2010241941194720112112 10.1007/s 00464-010-0883-7 · doi ↗ · pubmed ↗
- 3Nanda KS Tutticci N Burgess NG Endoscopic mucosal resection of laterally spreading lesions involving the ileocecal valve: technique, risk factors for failure, and outcomes Endoscopy 20154771071810.1055/s-0034-139173225763831 · doi ↗ · pubmed ↗
- 4Gurram KC Ly E Zhang XA novel technique of endoscopic submucosal dissection for circumferential ileocecal valve adenomas with terminal ileum involvement: the “doughnut resection” (with videos)Surg Endosc 2020341417142431728752 10.1007/s 00464-019-07202-1 · doi ↗ · pubmed ↗
- 5Kono M Takeuchi Y Higashino K Circumferential ileocecal valve removal for a colonic polyp using underwater endoscopic mucosal resection Endoscopy 202052 E 7E 810.1055/a-0977-251631398739 · doi ↗ · pubmed ↗