Bilateral Jaw Mycobacterium Abscessus Mimicking Actinomycosis: A Postoperative Complication of Wisdom Teeth Extraction
Michael Johanis, Karan S Cheema, Peter A Young, Gordon H Bae

TL;DR
A case of jaw infection caused by Mycobacterium abscessus was mistaken for actinomycosis after a dental procedure, highlighting the need for accurate diagnosis.
Contribution
This case highlights the diagnostic challenges of Mycobacterium abscessus mimicking actinomycosis and emphasizes the importance of microbial cultures.
Findings
Mycobacterium abscessus infection was misdiagnosed as Actinomycoses israelii following wisdom teeth extraction.
Dual antibiotic therapy with azithromycin and omadacycline led to clinical and radiographic improvement.
Genetic mutations in Mycobacterium abscessus affect macrolide susceptibility, requiring tailored treatment.
Abstract
The incidence of nontuberculous mycobacteria infections has surged over recent decades. Mycobacterium abscessus is one example that can present unique diagnostic challenges due to its variable antibiotic resistance profile and its clinical similarities to Actinomycoses israelii in postodontogenic infections. The authors report a case of a 22-year-old healthy female presenting with bilateral mandibular nodules following wisdom teeth extraction. After a presumptive diagnosis of actinomycosis, cultures revealed a Mycobacterium abscessus infection susceptible to macrolides. Magnetic resonance imaging depicted bilateral sinus tracts without osteomyelitis. The patient opted for dual antibiotic therapy, consisting of azithromycin and omadacycline, without surgical intervention. Given her clinical and radiographic improvement after three months, the patient elected to continue dual antibiotic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
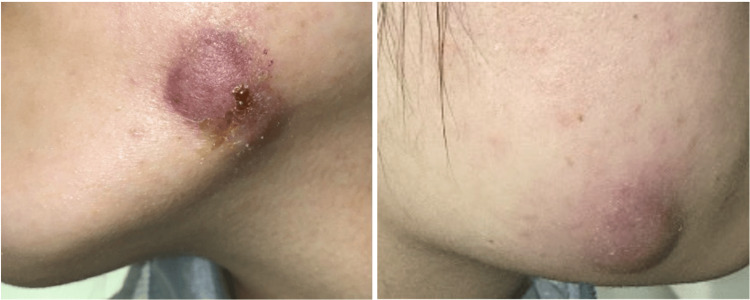 Figure 1
Figure 1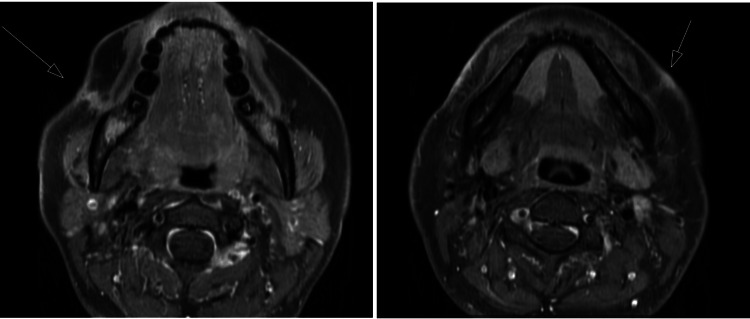 Figure 2
Figure 2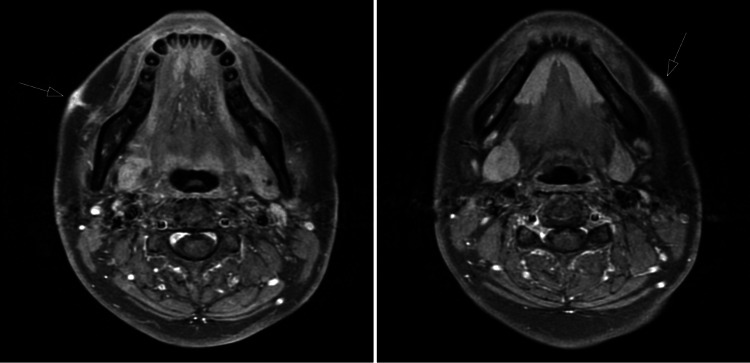 Figure 3
Figure 3| Antibiotic | Mycobacterium abscessus group (MIC MCG/ML) | |
| Amikacin | 32 ug/mL | Intermediate |
| Cefoxitin | 32 ug/mL | Intermediate |
| Ciprofloxacin | >4 ug/mL | Resistant |
| Clarithromycin | <=0.06 ug/mL | Susceptible |
| Doxycycline | >16 ug/mL | Resistant |
| Imipenem | 16 ug/mL | Intermediate |
| Linezolid | 2 ug/mL | Susceptible |
| Minocycline | >8 ug/mL | Resistant |
| Moxifloxacin | >8 ug/mL | Resistant |
| Tigecycline | 0.25 ug/mL | No Interpretation |
| Trimethoprim/Sulfamethoxazole | >8 ug/mL | Resistant |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMycobacterium research and diagnosis · Actinomycetales infections and treatment · Infectious Diseases and Mycology
Introduction
There are over 150 species of nontuberculous mycobacteria (NTM), the incidence of which has increased significantly in the last few decades [1]. One study conducted at the Mayo Clinic found that the incidence of cutaneous NTM infection was about three-fold higher from 2000-2009 compared to that of 1980-1999 in the suburban county encompassing this institution; these increased rates can be attributed to a growing population of immunosuppressed patients, as well as an increase in cosmetic procedures, such as tattoos, body piercings, and liposuction [2,3]. In particular, Mycobacterium abscessus (M. abscessus), a gram-positive and acid-fast staining bacterium, is one rapidly growing NTM responsible for high rates of treatment failure due to its antimicrobial resistance [1]. M. abscessus can be misdiagnosed as Actinomycoses israelii (A. israelii) in postodontogenic infections, especially given the latter pathogen’s incidence following dental treatments. A. israelii is a gram-positive, non-acid-fast, and rod-shaped microbacterium that causes a chronic granulomatous infection [4,5].
Case presentation
A 22-year-old otherwise healthy female was referred for “bilateral inflamed cysts.” Initial evaluation showed erythematous to purpuric nodules located bilaterally about the mandible (Figures 1A, 1B). These lesions, which were firm, indurated, and painless, appeared four weeks after an uneventful extraction of her four wisdom teeth by an oral surgeon.
Initial clinical presentation of the superficial plaques located in the bilateral mandibular regions(A) An indurated superficial plaque at the patient’s left mandibular region that was incised and drained of pus, leading to crustation around the cyst. (B) A cyst on the patient’s right mandibular site, which was similarly incised and drained of pus.
After a presumptive diagnosis of actinomycosis, an incision, and drainage were performed on both nodules to remove purulent tissue and material. Pathological examination revealed granulation tissue showcasing mixed inflammation, with no organisms seen on the gram stain. Tissue cultures were notable for M. abscessus, which was susceptible to macrolides without rrl or erm (41) mutations; Table 1 outlines the antibiotic susceptibility results. Magnetic resonance imaging (MRI) with contrast of the affected area revealed a sinus tract extending from the right buccal space at the level of the mandibular angle to the skin. A similar tract was noted on the left but to a lesser degree. Notably, there were no bony changes suggestive of osteomyelitis (Figures 2A, 2B).
Initial MRI findings(A) A tract of edema and enhancement that extends to the skin surface, where there is mild puckering, thickening, and enhancement. (B) A linear tract of subcutaneous soft tissue edema and enhancement leading to the overlying skin surface, with mild skin thickening and enhancement but without puckering.
The patient was prescribed azithromycin 250 mg daily and omadacycline 300 mg daily, and she was also referred to oral and maxillofacial surgery for possible sinus tract excision. She opted for antibiotic therapy without surgical intervention; given the risk of the infection spreading or failing to improve by declining surgery, the patient opted for serial monitoring every three months. Repeat MRIs in three months showed improvement of the sinus tracts in the right buccal space and left perimandibular soft tissues (Figure 3). Given the radiographic improvement, the patient opted to continue dual antibiotic therapy for 12 months with clinical and radiographic monitoring.
MRI findings at a three-month follow-upNotable improvement of the sinus tracts in the right buccal space and left perimandibular soft tissues following empiric antibiotic therapy, which, in combination with the patient’s preference to avoid surgery, significantly influenced the decision to continue antibiotic therapy for 12 months with appropriate clinical and radiographic monitoring.
Discussion
The differential diagnoses of postoperative odontogenic infections should include both M. abscessus and A. israelii. Endemic to the Southeastern USA (from Florida to Texas), M. abscessus is a rapidly growing mycobacterium that can be misdiagnosed as A. israelii [6]. This bacterium has been largely associated with dental procedures due to its prevalence in contaminated water, such as during irrigation procedures, though it is unclear whether our patient contracted the infection via a water source. One Southern California pediatric dental clinic reported in 2021 an outbreak of 71 cases, the largest outbreak of invasive M. abscessus at any pediatric health center [7]. There have been other reported outbreaks caused by non-sterile techniques and contaminated materials, particularly after surgical procedures including Mohs surgery, liposuction, breast tissue augmentation, and other cosmetic procedures [3]. Similarly, A. israelii is often associated with contaminated materials, but this pathogen can also cause cervicofacial actinomycosis, also known as “lumpy jaw syndrome,” which is present in 50-70% of infections [8]. Actinomycosis is rare, but the main risk factors are exposure to contaminated water during dental surgery or trauma, contact with contaminated sand, poor oral hygiene, malnutrition, and residence in tropical countries [8].
Since an accurate diagnosis of these infections can be difficult based exclusively on physical examination, we suggest obtaining microbial cultures early; with cultures, antibiotic susceptibility will also be available. Most M. abscessus subspecies bolletii and M. abscessus subspecies abscessus isolates have an active inducible macrolide resistance (erm) gene, which confers resistance to clarithromycin, though the M. abscessus subspecies massiliense does not. This difference affects treatment decisions regarding macrolide-involved regimens [9]. Additionally, acquired resistance to clarithromycin can be caused by a single point mutation in the rrl gene encoding its drug target, 23 rRNA, independent of an erm mutation. Numerous point mutations (T1406A, A1408G, and C1409T) have been identified in the rrs gene, which encodes 16S rRNA, conferring resistance to aminoglycosides. [10].
Conclusions
The authors present a rare case of a bilateral jaw M. abscessus infection following wisdom teeth extraction. This case highlights the diagnostic utility of cultures, which in turn inform the treatment plan based on susceptibility results. Clinicians must be cognizant of the overlapping clinical features while being able to differentiate between and appropriately treat the two diseases.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A case report on Mycobacterium abscessus: an emerging pathogen Cureus Chohan A Choudhury S Taweesedt PT Dadhwal R Vakil AP Ali Z Franco R 014202210.7759/cureus.23072 PMC 899507735419221 · doi ↗ · pubmed ↗
- 2Increased incidence of cutaneous nontuberculous mycobacterial infection, 1980 to 2009: a population-based study Mayo Clin Proc Wentworth AB Drage LA Wengenack NL Wilson JW Lohse CM 38458820132321879710.1016/j.mayocp.2012.06.029PMC 3690780 · doi ↗ · pubmed ↗
- 3Mycobacterium abscessus subspecies abscessus infection associated with cosmetic surgical procedures: Cases series ID Cases Moreno-Izquierdo C Zurita J Contreras-Yametti FI Jara-Palacios MA 022202010.1016/j.idcr.2020.e 00992 PMC 764457733194548 · doi ↗ · pubmed ↗
- 4Actinomycosis Stat Pearls Sharma S Hashmi MF Valentino IIIDJ. Treasure Island, Florida Stat Pearls Publishing 2023 https://www.ncbi.nlm.nih.gov/books/NBK 482151/
- 5Treatment of Mycobacterium abscessus pulmonary disease Chest Griffith DE Daley CL 647516120223431467310.1016/j.chest.2021.07.035 · doi ↗ · pubmed ↗
- 6Nontuberculous mycobacterial pulmonary infections J Thorac Dis Johnson MM Odell JA 210220620142462428510.3978/j.issn.2072-1439.2013.12.24PMC 3949190 · doi ↗ · pubmed ↗
- 7Invasive Mycobacterium abscessus outbreak at a pediatric dental clinic Open Forum Infect Dis Singh J O'Donnell K Nieves DJ 08202110.1093/ofid/ofab 165PMC 818624434113683 · doi ↗ · pubmed ↗
- 8Actinomycosis: etiology, clinical features, diagnosis, treatment, and management Infect Drug Resist Valour F Sénéchal A Dupieux C 183197720142504527410.2147/IDR.S 39601 PMC 4094581 · doi ↗ · pubmed ↗