An extra-cardiac lesion with pseudo-kidney sign detected by transthoracic echocardiography
Satoshi Kurisu, Hitoshi Fujiwara, Hiroko Todo, Yoshiro Tachiyama

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
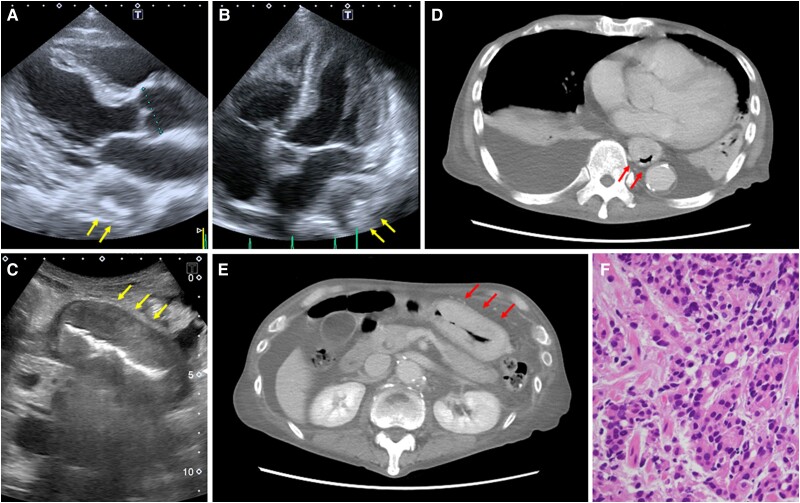 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal disorders and treatments · Gastrointestinal Tumor Research and Treatment · Eosinophilic Esophagitis
Case description
Transthoracic echocardiography (TTE) is a widely used modality for the assessment of cardiac structure and function. We report a patient with an extra-cardiac lesion detected by TTE, leading to a diagnosis of gastric cancer.
A 79-year-old man with dyspnoea and lower extremity oedema persisting for 2 weeks was referred to our hospital. He presented with weight loss of 4 kg over the past 3 months. The patient had no significant past medical or drug history.
Laboratory investigations showed haemoglobin of 5.4 g/dL, albumin of 2.2 g/dL, iron of 8 µg/dL, and N-terminal pro-brain natriuretic peptide of 1407 pg/mL. Liver and renal functions were normal. A TTE showed an extra-cardiac lesion measuring 33 × 30 mm located immediately adjacent to the left atrium. The lesion was characterized by a large hypoechoic mass with a central hyperechoic area, the so-called pseudo-kidney sign^1,2^ (Figure 1A and B, arrows). Left ventricular ejection fraction was 68%, and E/e′, a surrogate for left ventricular filling pressure, was 10. No significant valvular heart diseases were found. Given these findings, his symptoms were attributed mainly to severe anaemia and hypoalbuminaemia. An abdominal ultrasound also revealed pseudo-kidney sign in the stomach (Figure 1C, arrows). Computed tomography scans showed that these lesions were located in the oesophagus and stomach (Figure 1D and E, arrows). An oesophagogastroscopy was subsequently performed, revealing a wide lesion from the antrum to the cardia, invading the thoracic oesophagus. The pathological examination showed poorly differentiated gastric adenocarcinoma (Figure 1F). The patient received palliative care and eventually died on hospital Day 35.
A transthoracic echocardiogram showed an extra-cardiac lesion measuring 33 × 30 mm located immediately adjacent to the left atrium. The lesion was characterized by a large hypoechoic mass with a central hyperechoic area, the so-called pseudo-kidney sign (A and B, arrows). An abdominal ultrasound also revealed pseudo-kidney sign in the stomach (C, arrows). Computed tomography scans showed that these lesions were located in the oesophagus and stomach (D and E, arrows). The pathological examination showed poorly differentiated gastric adenocarcinoma (F).
The differential diagnosis of extra-cardiac posterior mediastinal lesions detected by TTE includes metastatic lymph nodes and oesophageal lesions, the majority of which are oesophageal cancers.^3^ Clinicians should be aware that unexpected lesions with pseudo-kidney sign may be detected during routine TTE.
Consent: The authors confirm that written consent for submission and publication of this case report including images has been obtained from the patient in line with COPE guidance.
Funding: None declared.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Anderson DR . The pseudokidney sign. Radiology 1999;211:395–397.10228519 10.1148/radiology.211.2.r 99ma 21395 · doi ↗ · pubmed ↗
- 2Su YJ, Lai YC. The pseudo-kidney sign. J Emerg Med 2011;40:e 115–e 116.19703739 10.1016/j.jemermed.2009.05.040 · doi ↗ · pubmed ↗
- 3Yan L, Ruan Q, Qu C, Huang C, Fu L. The value of transthoracic echocardiography in the detection of extra-cardiac lesions. BMC Surg 2022;22:73.35219301 10.1186/s 12893-022-01519-w PMC 8882299 · doi ↗ · pubmed ↗