Maternal Weight Gain in Early Pregnancy with Healthy Live Offspring: Based on the China Birth Cohort Study
Jingjing Wang, Simin Zhang, Qiao Li, Xiaowei Xiong, Qingqing Wu

TL;DR
This study examines how maternal weight gain in early pregnancy relates to gestational age among Chinese women with healthy live offspring.
Contribution
The study provides new insights into maternal weight gain patterns in early pregnancy for Chinese women with healthy offspring.
Findings
A linear correlation was found between gestational age and maternal weight gain (0.55 + 0.05 × GA).
The association remained robust across subgroups like BMI, ethnicity, and physical activity levels.
Abstract
Background: Research on maternal weight gain in early pregnancy with healthy live offspring is lacking for Chinese women. Based on the China birth cohort study (CBCS), we aimed to explore maternal weight gain in different groups. Methods: Singleton pregnancies of 6 + 0~13 + 6 weeks of gestation from the CBCS were considered, not including missing data or outliers, those lost at follow-up, or those with non-typical conditions of the offspring. Maternal first-trimester weight and body mass index (BMI) gain was considered as the early pregnancy weight minus the pre-pregnancy weight. Using Pearson’s or Spearman’s correlation and linear regression models to explore the relationship between maternal weight and BMI gain and gestational age (GA), stratified and sensitivity analyses were carried out to identify the study’s robustness. Results: There were 25,292 singleton pregnancies with healthy…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
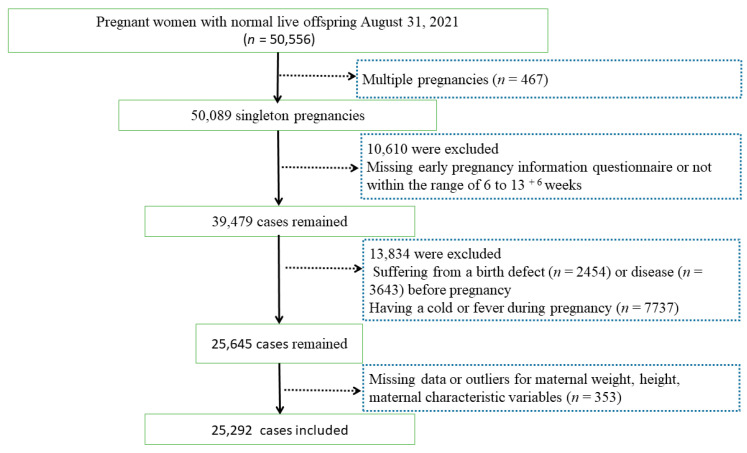 Figure 1
Figure 1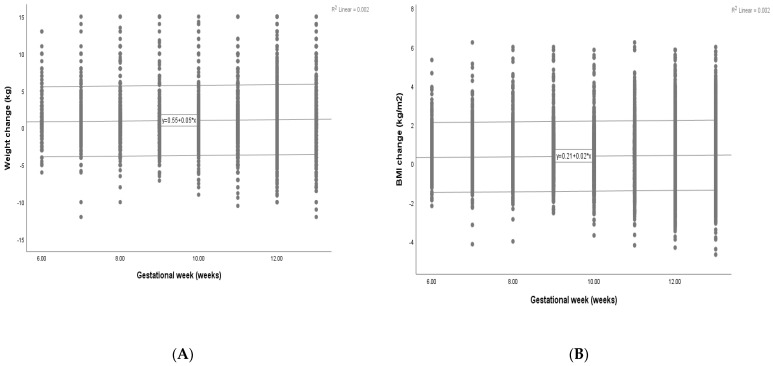 Figure 2
Figure 2- —National Key Research and Development Program of China
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGestational Diabetes Research and Management · Pregnancy and preeclampsia studies · Birth, Development, and Health
1. Background
Gestational weight gain (GWG) has become one of the hottest issues in modern obstetrics [1,2]. It has been identified as a strong and potentially controllable predictor of pregnancy and long-term health outcomes in women and infants, and is associated with various adverse outcomes [2,3,4,5,6]. An expert review [3] showed excessive GWG existed in about 48% of pregnant individuals in the United States and is associated with an increased risk of maternal and fetal complications. Analyzing the metabolomic profiles of children at birth, 6 months, and 12 months of age with maternal GWG, Guixeres-Esteve et al. [4] suggested that some metabolic shifts occurred during the first 12 months of life, which GWG may have modulated. Fritsche et al. [5] analyzed the relationship between maternal GWG and offspring autonomic nervous system (ANS) function in 2-year-old children and suggested that GWG has a critical impact on the development of the ANS. Excessive GWG may also increase the risk of neurodevelopmental disorders in offspring [6]. In addition, many factors affect GWG during pregnancy, such as behavioral, obstetric, and anthropometry characteristics [7]. The role of GWG should not be underrated [8].
The U.S. Institute of Medicine (IOM) provided recommendations on the total GWG (a gain of 12.5–18 kg for women with a pre-pregnancy body mass index (BMI) < 18.5, 11.5–16 kg for those with a BMI of 18.5–24.9, 7–11 kg for a BMI of 25–29.9, and 5–9 kg for a BMI ≥ 30) as well as for rates of GWG (0.44–0.58, 0.35–0.50, 0.23–0.33, and 0.17–0.27 kg/week, respectively) during the second and third trimesters based on BMI [9]. A systematic review and meta-analysis included 23 studies and found that, compared to GWG within the IOM-recommended levels, those with greater than or less than the guideline recommendations were associated with a higher risk of adverse maternal and infant outcomes [10]. Although the IOM guidelines are not universally implemented, they provide clinicians with a basis for practice [11,12]. However, some studies have reported inconsistent results on the link between GWG in particular BMI categories and adverse pregnancy outcomes, and what constitutes adequate GWG is relatively confusing [1,13,14,15].
Most studies have focused on the total GWG and rates of GWG during the second and third trimesters. Maternal weight gain in early pregnancy is also essential to women and infants. Calculating maternal weight gain for periods of <20 weeks, 21–29 weeks, and ≥30 weeks, Young et al. [16] analyzed 864 mother–child pairs in Vietnam and found that weight gain in the less-than-20-weeks group had the most remarkable association with postpartum weight retention and maternal (β 0.67, 95% CI 0.07 to 0.87) or child (β 0.42, 95% CI 0.15 to 0.69) percentage of body fat at 6 to 7 years. Additionally, our previous study, based on the China birth cohort study (CBCS), found that excessive weight gain in early pregnancy may be a potential predictor of fetal congenital heart disease (CHD) [15]. We hypothesized that maternal weight and BMI gain during early pregnancy were associated with gestational age (GA). The potential association might differ by maternal and fetal status, and little research has explored this association in cases with healthy live offspring based on a multicenter cohort study of Chinese women. Therefore, our study aimed to describe maternal weight and BMI gain with healthy live offspring in early pregnancy and analyze its relationship with GA, adjusted for maternal age, maternal pre-pregnancy BMI, morning sickness, and other confounding factors.
2. Methods
2.1. Study Design and Data Sources
The CBCS [17], a prospective, longitudinal, multi-center birth cohort study in China, started in November 2017, and data on pregnant women with healthy live offspring (n = 50,556) were extracted from the electronic system of the CBCS on 31 August 2021. The exclusion criteria included multiple pregnancies (n = 467); a missing early pregnancy information questionnaire or not being within the range of 6 to 13 ^+ 6^ weeks (n = 10,610); suffering from a birth defect (n = 2454) or disease (3643) before pregnancy, such as congenital heart defect, cleft lip and palate, polydactyly, heart disease, hypertension, diabetes, hepatitis B, thyroid disease, genital inflammation, periodontal disease; having a cold or fever during pregnancy (n = 7737); missing data or outliers for maternal weight or height (n = 305); missing maternal characteristic variables (n = 48), such as age, ethnicity, smoking or drinking status. Thus, 25,292 singleton pregnancies were ultimately included (Figure 1). The research was approved by the Ethics Committee of Beijing Obstetrics and Gynecology Hospital, Capital Medical University (Reference No. 2018-KY-003-02).
2.2. Data Collection and Measurements
In the CBCS, women were enrolled in early pregnancy and completed the baseline questionnaire by themselves during early pregnancy. Participation in the study was voluntary, and informed consent was obtained in writing. Their weights were accurately measured using an electronic scale (BW-150; UWE, Beijing, China), with the participants wearing light clothes, no shoes, and empty pockets [18]. This study collected the following information: (a) Demographic characteristics, including investigation date, maternal birth date, weight, height, ethnicity, education, family income, and occupation. (b) Current pregnancy information, including folic acid (FA) and multivitamin use in early/pre-pregnancy, last menstrual period, conception mode, and parity. (c) Lifestyle behaviors, including maternal alcohol consumption, smoking, and secondhand smoke exposure. Table 1 shows the calculation and classification of variables.
2.3. Statistical Analysis
Data calculations and statistical analyses were performed using IBM SPSS Statistics V.25 and SAS V.9.4 software. A p value of less than 0.05 was considered statistically significant. Quantitative data were expressed by the mean and standard deviation or the median and quartile range. As appropriate, the t-test, ANOVA test, Wilcoxon test, or Kruskal–Wallis H test was performed to calculate differences in the maternal weight and BMI gain among the maternal characteristics. The reference values for the 5th, 10th, 25th, 50th, 75th, 90th, and 95th percentiles for seven gestational periods (from 7 to 13 weeks) were calculated. Pearson’s correlation, Spearman’s correlation, and linear regression models were used to explore the relationship between maternal weight and BMI change and GA. Stratification was carried out to identify the robustness of the association of the maternal weight and BMI change in early pregnancy with GA in subgroups, including age (<35 years or ≥35 years), BMI (normal, low, overweight, or obesity), ethnicity (Han or Minority), family income (<200,000 or ≥200,000 CNY/year), physical activity (moderate, light, or active), educational level (college or university, high school or below, or postgraduate), parity (multipara or nullipara), smoking or drinking status (yes or no), morning sickness (yes or no), and FA and/or multivitamin supplementation (yes or no). A sensitivity analysis was performed in cases with normal or majority maternal status.
3. Results
3.1. Characteristics
Among all participants, 25,292 singleton pregnancies with healthy live offspring were ultimately enrolled, of which 1797 (7.1%), 3226 (12.8%), 2992 (11.8%), 2183 (8.6%), 1705 (6.7%), 2716 (10.7%), 7082 (28.0%), and 3591 (14.2%) cases answered the questionnaire in the periods of 6, 7, 8, 9, 10, 11, 12, and 13 gestational weeks, respectively. The mean and median ages were 29.6 ± 4.3 years and 29 (27, 32) years, respectively. The means of the maternal weight and BMI gain in early pregnancy were 1.0 ± 2.4 kg and 0.39 ± 0.92 kg/m^2^, while the medians were 1.0 (0.0, 2.0) kg and 0.37 (0.00, 0.78) kg/m^2^, respectively. Table A1 and Table A2 in the Appendix A show the percentiles of weight gain and BMI change in different gestational weeks. Table 2 presents the significant differences in maternal weight and BMI change among age, BMI, ethnicity, income, educational level, parity, smoking or drinking status, morning sickness, FA and/or multivitamin supplementation, and GA (all with p-values < 0.05).
3.2. Relationship between Maternal Weight and BMI Gain and GA
Maternal weight and BMI gain demonstrated linear correlations with GA (p = 0.001, <0.001). The scatter plot of the maternal weight and BMI gain shows progressive changes with advancing gestation (Figure 2). The mean maternal weight change increased slightly from 0.85 kg in 6 weeks to 1.20 kg in 13 weeks (weight gain = 0.55 + 0.05 × GA (weeks), p < 0.001, r^2^ = 0.002). Similarly, the maternal BMI change shows a linear increase (BMI change = 0.21 + 0.02 × GA (weeks), p < 0.001, r^2^ = 0.002).
3.3. Stratified Analyses
The association of the maternal weight and BMI change in early pregnancy with GA was also found in subgroups, including age (<35 years or ≥35 years), BMI (normal or low), Han ethnicity, family income (<200,000 or ≥200,000 CNY/year), educational level (college or university, high school or below, and postgraduate), moderate levels of physical activity, parity (multipara or nullipara), smoking or drinking status (yes or no), natural conception, morning sickness (yes or no), and with FA and/or multivitamin supplementation (Table 3).
3.4. Sensitivity Analysis
Cases with normal or majority maternal status, including maternal normal BMI, Han ethnicity, natural conception, with FA and/or multivitamin supplementation, and without smoking or drinking status or morning sickness were selected, and 7431 cases were included to perform sensitivity analysis. The association of maternal weight and BMI gain in early pregnancy with GA was still found (Table 4). The mean maternal weight gain increased slightly from 0.76 kg at 6 weeks to 1.32 kg at 13 weeks, while the maternal BMI increased from 0.28 kg/m^2^ to 0.49 kg/m^2^.
4. Discussion
4.1. Main Findings of This Study
This study included a relatively large sample size of 25,292 singleton pregnancies with healthy live offspring based on the China birth cohort study, allowing us to explore the potential association of maternal weight and BMI change in early pregnancy with GA in subgroups, including maternal demographic characteristics, current pregnancy information, and lifestyle behaviors. There was a slight correlation between GA and maternal weight and BMI gain. The association remained robust especially in pregnant women with typical or low pre-pregnancy BMI, Han ethnicity, moderate levels of physical activity, natural conception, and with FA and/or multivitamin supplementation, regardless of maternal age, family income, educational level, parity, morning sickness, smoking or drinking status. Furthermore, the associations of maternal weight and BMI gain in early pregnancy with GA were also shown in the normal or majority maternal status.
4.2. Possible Reasons and Comparison with Previous Studies
A retrospective study [19] with 9075 singleton pregnant women in China found that the 2009 IOM guideline was more suitable for pregnant women with inadequate GWG. Meanwhile, another retrospective cohort study [20] comprising 20,593 singleton pregnant women in Beijing, China, found that the IOM guidelines were suitable for Chinese women with underweight pre-pregnancy BMI. Maternal weight gain in early pregnancy is also associated with the outcomes of pregnant women and fetuses. Gaillard et al. [21] analyzed 5,908 mothers and their children from a population-based prospective cohort study and found that higher weight gain in early but not in mid or late pregnancy was associated with an adverse cardio-metabolic profile in offspring. Additionally, Young et al. [22] used secondary data with 1436 cases from a randomized controlled trial in Vietnam and found that compared to ≥ 30 weeks’ gestation, 1 SD increase in maternal conditional weight gain in the first 20 weeks had three times the influence on birth weight and was associated with a 43% reduction in small for gestational age (SGA) risk (OR 0.57, 95% CI 0.46 to 0.70). As we all know, maternal weight gain is associated with GA and could be influenced by multiverse factors, such as demographic characteristics, intervention, breastfeeding practices, diet, and physical activity.
Nausea and vomiting during pregnancy (NVP), also called morning sickness, usually begins at 4–6 weeks of gestation, peaks at 8–12 weeks, and often disappears naturally at mid-pregnancy, affecting 70% of pregnant women [23,24,25]. The risk of severe NVP may be influenced by a protein released by fetal cells in the placenta [26], which could affect maternal weight gain. The association of maternal weight and BMI change in early pregnancy with GA was found in both those with morning sickness and those without. Unfortunately, the lack of information on cases suffering from hyperemesis gravidarum and on the second and third trimesters limits the study.
Previous guidelines and recommendations have suggested that appropriate maternal weight gain differs by the pre-pregnancy BMI range [9,11]. Ukah et al. explored the association between GWG and severe adverse birth outcomes in the US by calculating the optimal, low, and excess weight gain in each BMI category [27]. This study also found an association of maternal weight and BMI change in early pregnancy with GA in typical or low BMI subgroups but not in the overweight or obesity group. One possible reason may be that women who are overweight or obese before pregnancy are more focused on their weight management during pregnancy. The other reason may be that 73.5% of participants had typical BMI, and those with overweight (10.6%) or obesity (2.1%) were lower. Additionally, pregnant women with underweight, overweight, or obese status may be more coached by their doctors to gain or lose weight.
This study also found the association of maternal weight and BMI change in early pregnancy with GA in the multipara and nullipara subgroups. Cohen et al. conducted a population-based observational study in Canada and found that women whose firstborn experienced certain adverse perinatal events gained more weight and were more likely to transition to a higher BMI category in their subsequent pregnancy [28]. Unfortunately, the details of the firstborn in the multipara group were lacking in this study, which may lead to a bias.
Because the cases with abnormal BMI, minority ethnicity, assisted reproduction, without FA and/or multivitamin supplementation, and smoking or drinking status were relatively small in this study, and because morning sickness could affect maternal weight gain in early pregnancy, a sensitivity analysis was carried out to identify the study’s robustness by selecting cases with normal or majority maternal status. An association of maternal weight and BMI change in early pregnancy with GA was still found.
4.3. Limitations of the Study
Several limitations must be acknowledged. First, although this study included a relatively large sample size of singleton pregnancies with healthy live offspring based on the CBCS, not all confounders affecting maternal weight were included, and some related influence on these unknown factors cannot be ruled out. Second, the maternal weight in the periods of 6-14 gestational weeks was not measured continuously, and there were no data on the weight gain during the second and third trimesters. Third, since the last follow-up was performed after delivery, the healthy live-born offspring defined in this study may also have conditions such as disease or defects in later infancy. Fourth, GA was calculated as the first date of the last menstrual cycle in this study and not determined by ultrasound, which may lead to bias. Furthermore, many essential data (lifestyle behaviors, including maternal alcohol consumption, smoking, and exposure to passive smoking) were collected through questionnaires, and there may be information bias. All of these factors may lead to biased estimates and indicate that the validation of our results is necessary, especially in longitudinal data with continuous maternal weight measurement and prolonged follow-up time of offspring.
5. Conclusions
Although the association of GA and maternal pre-pregnancy weight and BMI gain is weak, a slight correlation was shown, especially in pregnant women with a typical or low pre-pregnancy BMI, Han ethnicity, moderate levels of physical activity, natural conception, and with FA and/or multivitamin supplementation. However, this study does not suggest that weight gain during early pregnancy is better than weight loss. This finding may be helpful for determining the appropriate range of maternal weight gain in early pregnancy with healthy live offspring in China and other countries.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lee F.K. Horng H.C. Wang P.H. Body weight and pregnancy Taiwan J. Obstet. Gynecol.20195889990010.1016/j.tjog.2019.03.01331759554 · doi ↗ · pubmed ↗
- 2Horng H.C. Lee W.L. Wang P.H. Maternal weight gain and birth weight J. Chin. Med. Assoc.20218474174210.1097/JCMA.000000000000056334108428 PMC 12965998 · doi ↗ · pubmed ↗
- 3Gascoigne E.L. Webster C.M. Honart A.W. Wang P. Smith-Ryan A. Manuck T.A. Physical activity and pregnancy outcomes: An expert review Am. J. Obstet. Gynecol. MFM 2023510075810.1016/j.ajogmf.2022.10075836174931 PMC 9772147 · doi ↗ · pubmed ↗
- 4Guixeres-Esteve T. Ponce-Zanón F. Morales J.M. Lurbe E. Alvarez-Pitti J. Monleón D. Impact of Maternal Weight Gain on the Newborn Metabolome Metabolites 20231356110.3390/metabo 1304056137110219 PMC 10142613 · doi ↗ · pubmed ↗
- 5Fritsche L. Hartkopf J. Hummel J. Löffler D.S. Yamazaki H. Häring H.-U. Peter A. Birkenfeld A.L. Wagner R. Fritsche A. Maternal Weight Gain during Pregnancy and the Developing Autonomic Nervous System-Possible Impact of GDM Nutrients 202214522010.3390/nu 1424522036558379 PMC 9784678 · doi ↗ · pubmed ↗
- 6Chen S. Fan M. Lee B.K. Dalman C. Karlsson H. Gardner R.M. Rates of maternal weight gain over the course of pregnancy and offspring risk of neurodevelopmental disorders BMC Med.20232110810.1186/s 12916-023-02799-636959571 PMC 10035205 · doi ↗ · pubmed ↗
- 7Manera F. Fernandes R.C. Höfelmann D.A. Trajectory Patterns of Gestational Weight Gain J. Am. Nutr. Assoc.20234264365010.1080/27697061.2022.212509936219394 · doi ↗ · pubmed ↗
- 8Santos M.S. Santos T. Fonseca L. Saraiva M. Pichel F. Pinto C. Pereira M.T. Vilaverde J. Almeida M.C. Dores J. Inappropriate gestational weight gain impact on maternofetal outcomes in gestational diabetes Ann. Med.20235520721410.1080/07853890.2022.215906336538030 PMC 9788720 · doi ↗ · pubmed ↗