Radiologic Evaluation of Oral Health Status in Patients Admitted to the Intensive Care Unit: A Multi-Institutional Retrospective Study
Yesel Kim

TL;DR
This study finds that most ICU patients have oral health issues, with higher prevalence in males and older adults.
Contribution
The study provides multi-institutional data on oral health in ICU patients using radiologic evaluation.
Findings
67% of ICU patients had at least one oral lesion.
Males and those aged 40+ had significantly higher lesion prevalence.
Surgical ICU patients showed better oral health compared to others.
Abstract
Introduction: Surveys distributed among intensive care unit (ICU) nurses reveal a significant need for dental care, with many acknowledging poor oral hygiene management. Poor oral health in ICU patients is linked to systemic problems, including aspiration pneumonia, necessitating pre-intervention assessments for bacterial diseases and dental risks. This study aims to evaluate the oral health status of ICU patients across three institutions through retrospective analysis. Methods: This retrospective study assessed the oral health status of ICU patients, using computed tomography (CT) images from three institutions over ten years. Through CT images, the oral status was evaluated in terms of total and lost tooth count and the presence of oral lesions (periapical lesions, cysts and tumors, caries, tartar, moderate to severe periodontal bone loss, tooth fractures). Variables included gender,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
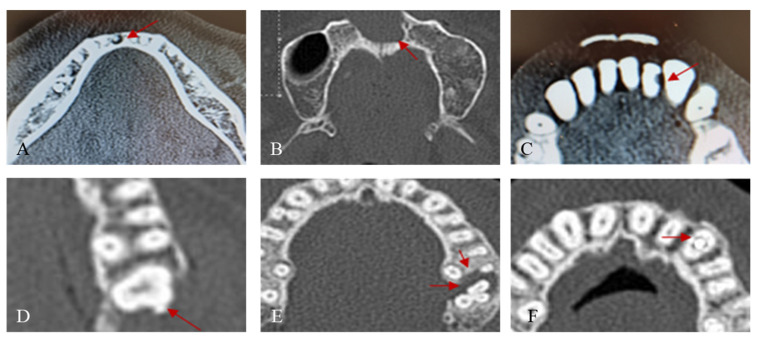 Figure 1
Figure 1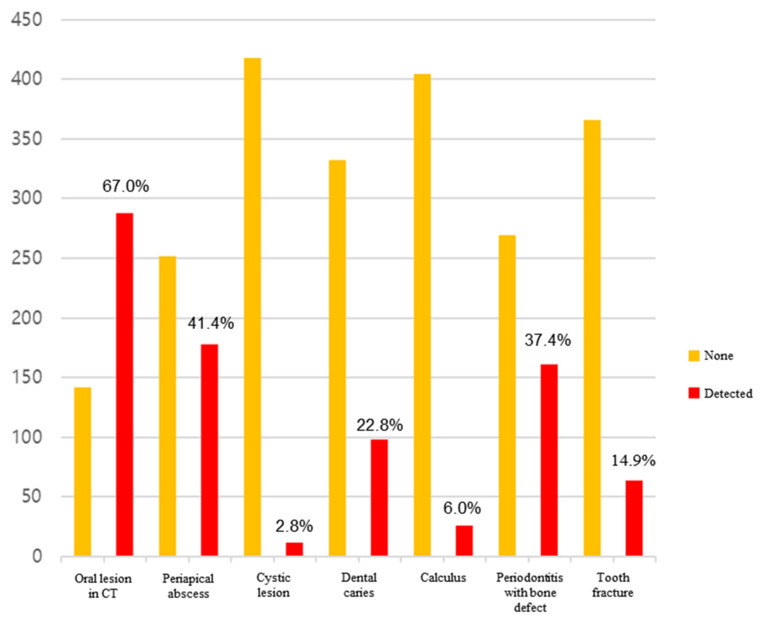 Figure 2
Figure 2- —Armed Forces Capital Hospital
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNosocomial Infections in ICU · Dental Research and COVID-19 · Airway Management and Intubation Techniques
1. Introduction
Patients in intensive care unit (ICUs) often experience oral dryness due to medication, oral lesions, mastication and swallowing disorders, and the lack of voluntary oral hygiene, with many finding it difficult to communicate their needs [1,2]. According to a survey by RJG de Araujo among ICU nurses, 86% felt the need for dental care, and 98% agreed that a dental team should be present in the ICU [3]. Survey results among ICU nurses indicate that 53–58% admit to the poor management of patients’ oral hygiene, and about 80% neglect oral care compared to other body parts. Oral dental issues can significantly contribute to systemic problems by serving as reservoirs for pathogens [4,5]. Before interventions begin, it is crucial to eliminate bacterial diseases, especially since poor oral hygiene in ICU patients is closely linked to aspiration pneumonia [6,7,8,9]. It is noted that tooth loss, prosthesis dislodgement, tooth damage, and temporomandibular joint dislocation often occur in patients with intubation, endoscopy, or oral devices for airway maintenance, yet these risks are rarely assessed beforehand [4].
Many inpatients in the ICU present with side effects and various conditions, including hyposalivation associated with medications, chewing and swallowing discomfort due to antineoplastic treatments, the presence of oral lesions caused by systemic diseases, and difficulty in maintaining oral hygiene during hospitalization [1,2,3]. Unfortunately, oral hygiene kits are insufficient and nursing teams are not qualified or trained to perform oral hygiene and provide proper oral care instructions [1]. It is not well known when a dentist should intervene in the hospital environment [3]. ICU patients find it challenging to visit the dentist, and poor oral hygiene is very common in ICU settings. A systematic review and meta-analysis in 2011 reported that the plaque index of hospitalized patients significantly increased, rising from 23% upon admission to 93% after 10 days of hospitalization [4]. Additionally, two studies reported a severe increase in the gingival inflammation index [5,6]. Particularly in the ICU, where monitoring organs and systems to prevent deterioration is crucial [3], the condition of the oral cavity is also important, emphasizing the role of hospital dentistry. Dentists and dental hygienists also work in multidisciplinary teams, especially in the hospital, which is essential when the ultimate goal is improving the quality of life of patients [7].
The 2020 Korean Nurses Association guidelines for oral care aim to enable patients to manage their own oral hygiene [8]. However, from a dental perspective, self-managed oral hygiene does not guarantee cleanliness. The guidelines recommend dental care in cases where patients do not express symptoms (pain, tooth mobility, and bleeding during brushing), making it challenging for nurses without dental expertise to perform accurate assessments (gingival swelling, calculus, discoloration of teeth or tongue, and ill-fitting prostheses) [9]. International studies show that 82.5% of patients admitted for non-dental reasons require active dental treatment, and 58.6% need invasive dental interventions, with over 62.2% at risk of oral complications during their stay and more than 34% harboring acute conditions (abscess drainage, tooth mobility, toothache, and the need for extraction) [9]. Nursing teams’ criteria for assessing oral conditions traditionally follow the Oral Assessment Guide (OAG) proposed by Eilers [10]. This assessment guideline is based on nurses’ observations using sight, hearing, and touch, but it excludes the evaluation of periodontal disease and dental caries, which are the most common bacterial diseases in the oral cavity. Therefore, it is necessary to assess the oral condition of ICU patients from a dental perspective and determine if more proactive dental intervention is needed beyond the current level of oral hygiene management based on the assessment results. The purpose of this study is to evaluate the oral health status of patients admitted to the ICUs of three domestic institutions over the past ten years through a multi-institutional retrospective analysis.
2. Material and Methods
This study was approved by the Institutional Review Board at Armed Forces Capital Hospital (AFCH-21-IRB-009), Seoul National University Bundang Hospital (B-2106/691-105), Gangnam Severence Hospital (3-2021-0199). This study was conducted according to the principles of the Declaration of Helsinki for research on humans.
The oral health status of patients admitted to the ICU from 1 March 2011 to 31 March 2021 was retrospectively assessed using facial CT, neck CT, and mandible CT images taken either during their ICU stay or immediately before ICU admission. The selection criteria were as follows: (1) individuals with at least one recorded image of facial CT, neck CT, or mandible CT, taken during their stay in the emergency room or while admitted to the ICU; and (2) adults aged 19 or older with a history of ICU admission. Exclusion criteria included (1) patients under 19, (2) patients with congenital deformities in the maxillofacial area, (3) patients admitted to the ICU under a dental primary care provider, and (4) patients without radiographic images available for evaluating oral status. A total of 450 individuals were selected for this multi-institutional study across three research institutions, with 20 individuals excluded due to unreadable images, resulting in a final sample size of 430 for analysis.
Oral lesions were identified by screening cross-sectional and longitudinal sections of the maxilla and mandible based on the oral plane in head and neck CT (facial CT, neck CT, and mandible CT), evaluating the number of remaining and lost teeth, and assessing the presence or absence of six types of oral lesions as per the defined criteria (Figure 1). The outcomes included (1) total and lost tooth counts of the subjects; (2) average MT index (missing permanent teeth index) per subject in the study group; and (3) the presence of oral lesions (periapical lesions, cysts and tumors, caries, calculus, moderate to severe periodontal bone loss, and tooth fractures). The variables included (1) gender, (2) age, (3) duration of ICU stay, (4) primary department at admission, and (5) type of ICU (surgical/medical ICU). The imaging exmainations were conducted by a dentist (J.K.Ku)
Descriptive statistics and frequency analyses were conducted for general characteristics. Differences in the number of remaining and lost teeth, assessed according to general characteristics, were analyzed using chi-square tests and independent-sample t-tests. Logistic regression analysis was performed to identify risk factors for the presence of oral lesions. Data are expressed as means ± standard deviations and analyzed using IBM SPSS Statistics 25.0 (IBM, Armonk, NY, USA).
3. Results
Out of the 450 study participants, 20 were excluded due to non-diagnostic images, leaving 430 (58 patients in Armed Forces Capital Hospital, 238 patients in Seoul National University Bundang Hospital, and 150 patients in Gangnam Severence Hospital) patients for final analysis. The head and neck CTs used for analysis comprised 48.1% neck CTs and 51.9% facial CTs. The gender distribution was 67% male and 33% female, with an average age of 56.6 years. The average ICU stay was 18.6 days, with surgical ICU types accounting for 83.7% of cases. In the CT scans of all patients, oral lesions were found in 67.0% of cases (Figure 1). The frequency of the discovered oral lesions was as follows: periapical abscess (41.4%), periodontitis with bone defect (37.4%), dental caries (22.8%), tooth fracture (14.9%), calculus (6.0%), and cystic lesion (2.8%). The results are given in descending order.
3.1. Differences in General Characteristics by Gender
The results of assessing the different types of medical department by gender showed that both men and women were most frequently seen in surgical departments. The type of ICU showed that the emergency department frequency was the highest for both men and women, with statistically significant differences (Table 1).
3.2. Differences in General Characteristics by Age
When assessing differences in institutions by age, the results showed statistically significant differences. The type of medical department visited for all three age groups was most frequently surgical (Table 2).
3.3. Evaluation of Oral Condition through the Analysis of Medical Records
3.3.1. Evaluation of Oral Condition of the Subjects through the Analysis of Medical Records
The average number of remaining teeth in the subjects was 23.2, with an average of 4.8 teeth lost (Table 3). The presence of oral lesions, as determined through CT image analysis, showed that 33% of subjects had at least one lesion.
3.3.2. Differences in Oral Health Status Assessment According to General Characteristics
When applied among study participants, the results of the Missing Permanent Teeth Index (MPTI) varied according to the general characteristics, with the highest MPTI observed at Bundang Seoul National University Hospital at 5.6, and the lowest at Gangnam Severance Hospital at 3.7. The MPTI increased with age, showing more than 8 teeth missing in individuals aged 60 and over compared to those aged 19–39. The index score was higher in the medical department, standing at 7.2, compared to the surgical department (Table 4).
The assessment of oral health status by gender showed that men had a higher frequency of having at least one oral lesion compared to women, and men also showed a higher frequency of tooth fractures (Table 5). Age-related assessments of oral health status revealed significant differences in the number of remaining and missing teeth. Furthermore, the presence of oral lesions increased with age, showing a statistically significant difference in terms of the frequency of having at least one lesion (Table 6). The assessment of oral health status by ICU type showed that the surgical department had a higher average number of remaining teeth (23.7) compared to the medical department (20.8), with statistically significant differences. Tooth fractures among oral lesions were more frequent in the surgical department, showing a statistically significant difference (Table 7).
3.3.3. Risk Factors Influencing the Prevalence of Oral Lesions
To identify the risk factors affecting the prevalence of oral lesions, logistic regression analysis was performed, focusing on variables that showed significance among oral examinations and general characteristics. The regression model was statistically significant (Hosmer and Lemeshow x^2^ = 7.189, p = 0.515), with an explanatory power of approximately 12.6% (Nagelkerke R^2^ = 0.126). The significance test of regression coefficients revealed that gender, age, and the duration of ICU stay have a significant impact on the occurrence of oral lesions. The prevalence of oral lesions increases by 1.03 times with each increase in age (Table 8).
4. Discussion
This study investigates the oral health of ICU patients over ten years across three institutions, recognizing that such patients often experience oral health issues due to factors like medication effects, lack of voluntary hygiene, and medical interventions. Oral health status reveals significant oral health issues among ICU patients, with the average number of remaining teeth being 23.2 and an average loss of 4.8 teeth. Sixty-seven percent of subjects had at least one oral lesion, detected via CT. The missing permanent teeth (MT) index score varied by age, hospital days, and types of ICU, with higher indices observed in older patients and those undergoing medical care. Oral lesions increased with age, and males were more likely to have them, including tooth fractures. Notably, patients aged 40 and older showed a significantly higher prevalence of dental abscesses, caries, and advanced periodontitis, highlighting the urgent need for proactive dental treatments and policy development for oral evaluation and management in ICU settings.
In 2021, Jun et al. published a review of studies on the oral health status of ICU patients [11]. Their systematic review identified indicators used to assess oral health from a dental perspective, including the plaque index [4,12], periodontitis (probing depth, bleeding on probing) [12,13], the number of teeth lost [12], dental caries [13], tooth fracture [13], odontogenic abscess [13], gingivitis [13], oral candidiasis [13,14], and mucositis [13], along with evaluations of the need for dental intervention [14,15,16]. These studies found that 65–90% of cases required dental treatment, diagnosed through visual and tactile examination by dental professionals. Bellissimo-Rodrigues et al. reported that gingivitis was the most frequently occurring oral condition requiring treatment [13]. Given that gingivitis, a bacterial disease, can increase the risk of ventilator-associated pneumonia (VAP) if left untreated due to plaque accumulation, The Center for Disease Control and Prevention recommends managing oral hygiene [17]. However, varieties of periodontitis with bone destruction, periapical abscess, cracked tooth, and tooth fracture are more serious dental diseases than gingivitis, and they cannot be resolved with oral hygiene management alone, requiring professional treatment by a dentist.
This study was conducted via examinations, using CT scans to determine the extent to which patients admitted to the ICU were affected by these serious conditions. Oral lesions requiring treatment were found in 66.97% (288/430) of patients, with an average of 1.5 oral lesions per patient (Figure 2). Among them, the three most frequently occurring conditions, periapical abscess (41.4%), periodontitis with bone defect (37.4%), and dental caries (22.8%), can cause severe symptoms if not treated aggressively. Additionally, they are more serious bacterial diseases than gingivitis. In particular, periapical abscesses can be difficult to diagnose without radiographic images, suggesting that a considerable number of ICU patients may be underdiagnosed. Additionally, many studies report that interventions by dental professionals significantly reduce the incidence of pneumonia and mortality due to respiratory diseases [13,17,18,19]. This study discovered that individuals aged 60 and above, particularly males (Table 8), face a statistically significant higher risk of developing oral lesions. Considering the frequency of gingivitis, candidiasis, mild calculus, and mild periodontitis that are not visible in radiographs, the need for active dental care among ICU patients is likely to increase. Consequently, it may be advisable to initially screen ICU patients in order to assess their oral health using radiographs or dental exams. This approach would enable immediate proactive dental treatment upon admission, especially for elderly male patients.
5. Conclusions
This study, based on a decade of record analysis, confirms that 67% of ICU patients had at least one oral lesion detectable on radiographs, with male patients aged 40 and older showing a significantly higher prevalence of oral lesions. This underscores the urgent need for proactive dental treatments and highlights the necessity of developing policies for oral evaluation and management in ICU patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Blum D.F.C. Silva J. Baeder F.M. Della BonaÁ. The practice of dentistry in intensive care units in brazil Rev. Bras. Ter. Intensiv.20183032733210.5935/0103-507X.2018004430183977 PMC 6180464 · doi ↗ · pubmed ↗
- 2Berti-Couto Sde A. Couto-Souza P.H. Jacobs R. Nackaerts O. Rubira-Bullen I.R. Westphalen F.H. Moysés S.J. Ignácio S.A. Costa M.B. Tolazzi A.L. Clinical diagnosis of hyposalivation in hospitalized patients J. Appl. Oral Sci.20122015716110.1590/S 1678-7757201200020000622666830 PMC 3894756 · doi ↗ · pubmed ↗
- 3Martinez B. Fidelis F. Mastrocolla L. Tempest L. Araujo T. Castro F. Abbud A. Kassis E. Filho I. Main aspects of hospital dentistry: Review of its importance Int. J. Adv. Res.201642099210610.21474/IJAR 01/2026 · doi ↗
- 4Fourrier F. Duvivier B. Boutigny H. Roussel-Delvallez M. Chopin C. Colonization of dental plaque: A source of nosocomial infections in intensive care unit patients Crit. Care Med.19982630130810.1097/00003246-199802000-000329468169 · doi ↗ · pubmed ↗
- 5Prendergast V. Hallberg I.R. Jahnke H. Kleiman C. Hagell P. Oral health, ventilator-associated pneumonia, and intracranial pressure in intubated patients in a neuroscience intensive care unit Am. J. Crit. Care Off. Publ. Am. Assoc. Crit.-Care Nurses 20091836837610.4037/ajcc 200962119556415 · doi ↗ · pubmed ↗
- 6Franklin D. Senior N. James I. Roberts G. Oral health status of children in a paediatric intensive care unit Intensiv. Care Med.20002631932410.1007/s 00134005115610823389 · doi ↗ · pubmed ↗
- 7Godoi A.P.T.d. Francesco A.R.d. Duarte A. Kemp A.P.T. Silva-Lovato C.H. Odontologia hospitalar no brasil: Uma visão geral Rev. Odontol. UNESP 200938105109
- 8Cho Y.-A. Lee S.-H. Kim K.-S. Im H.-M. Kim T.-H. Choi M.-Y. Seo H.-J. Park H.-S. Wang K.-H. Kim C.-H. Updates of nursing practice guideline for oral care J. Korean Clin. Nurs. Res.20203141153