Anatomical Variants of the Origin of the Coronary Arteries: A Systematic Review and Meta-Analysis of Prevalence
Juan José Valenzuela Fuenzalida, Emelyn Sofia Becerra-Rodriguez, Alonso Sebastián Quivira Muñoz, Belén Baez Flores, Catalina Escalona Manzo, Mathias Orellana-Donoso, Pablo Nova-Baeza, Alejandra Suazo-Santibañez, Alejandro Bruna-Mejias, Juan Sanchis-Gimeno

TL;DR
This study reviews and analyzes the prevalence of anatomical variants in coronary artery origins and their clinical implications.
Contribution
The study provides a systematic review and meta-analysis of coronary artery origin variants and their prevalence.
Findings
The pooled prevalence of coronary artery origin variants was found to be 1%.
The funnel plot showed significant asymmetry, indicating potential bias or heterogeneity in the data.
Abstract
Purpose: The most common anomaly is an anomalous left coronary artery originating from the pulmonary artery. These variants can be different and depend on the location as well as how they present themselves in their anatomical distribution and their symptomatological relationship. For these reasons, this review aims to identify the variants of the coronary artery and how they are associated with different clinical conditions. Methods: The databases Medline, Scopus, Web of Science, Google Scholar, CINAHL, and LILACS were researched until January 2024. Two authors independently performed the search, study selection, and data extraction. Methodological quality was evaluated using an assurance tool for anatomical studies (AQUA). Pooled prevalence was estimated using a random effects model. Results: A total of 39 studies met the established selection criteria. In this study, 21 articles with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
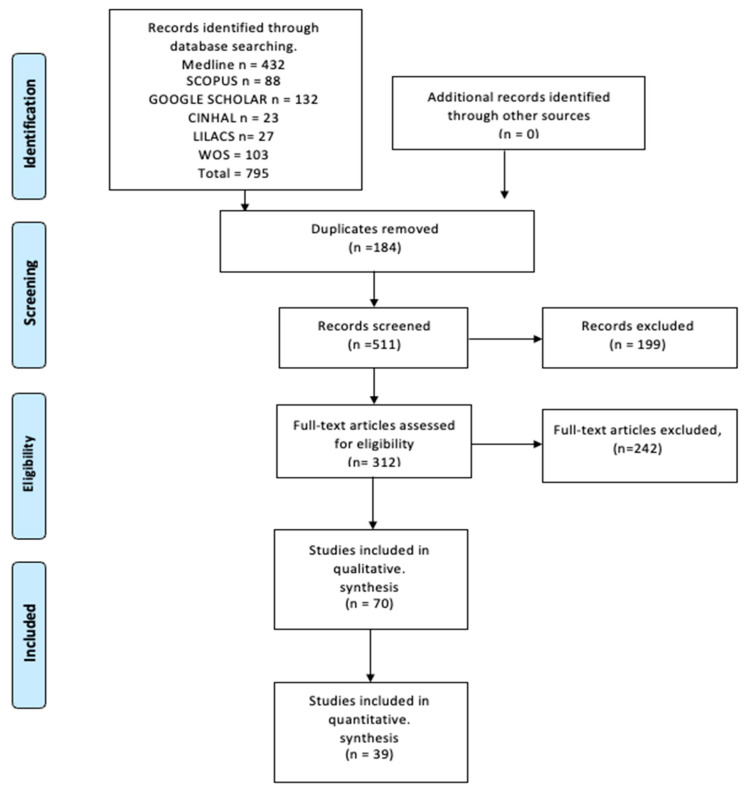 Figure 1
Figure 1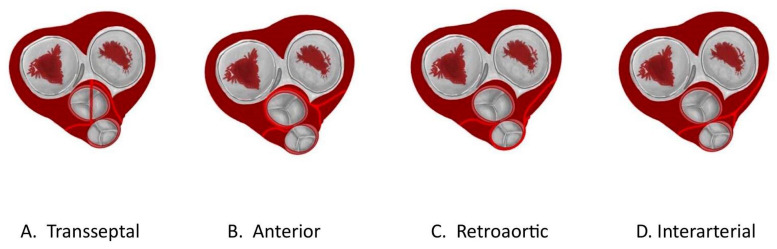 Figure 2
Figure 2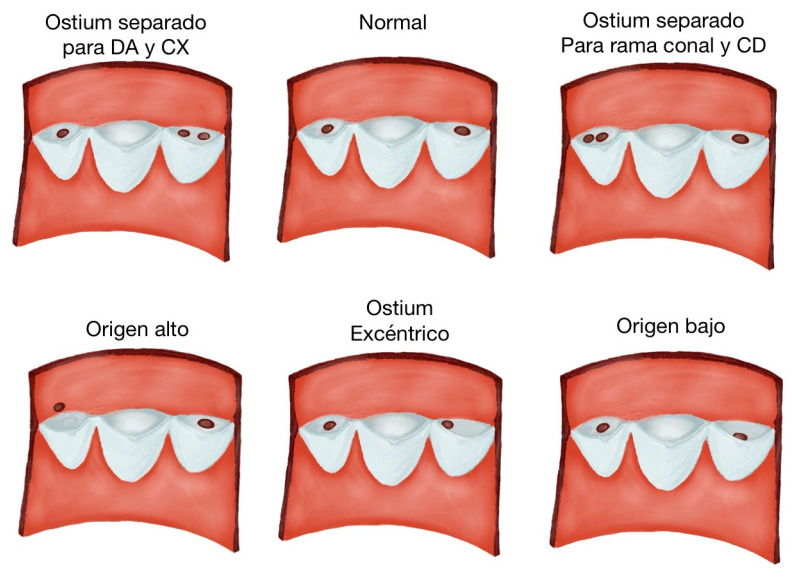 Figure 3
Figure 3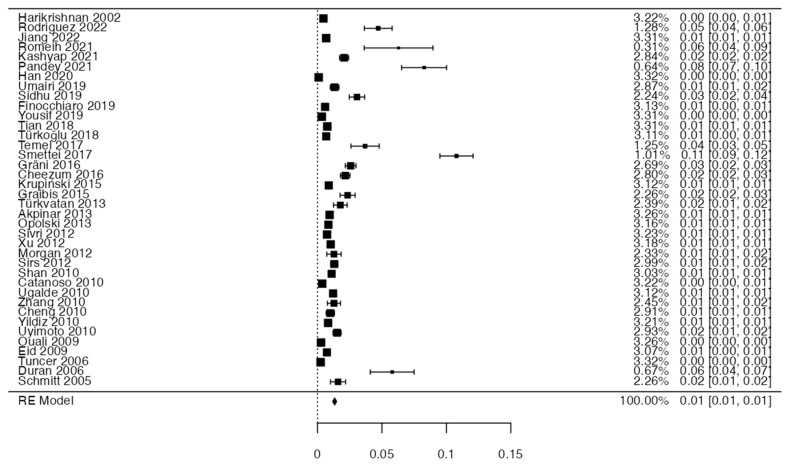 Figure 4
Figure 4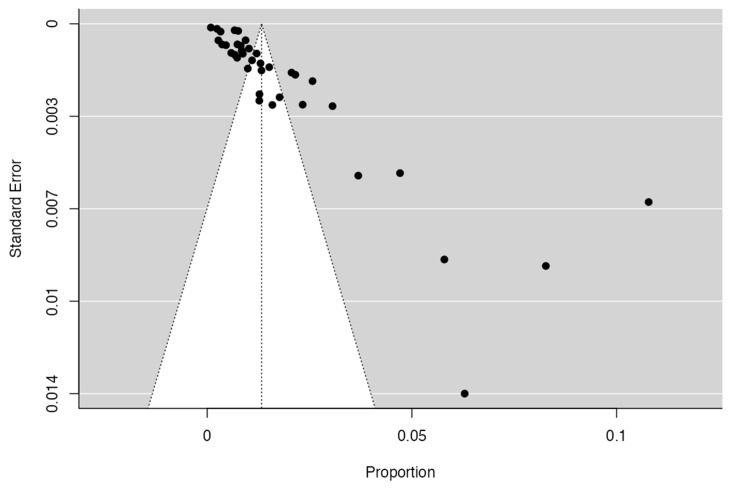 Figure 5
Figure 5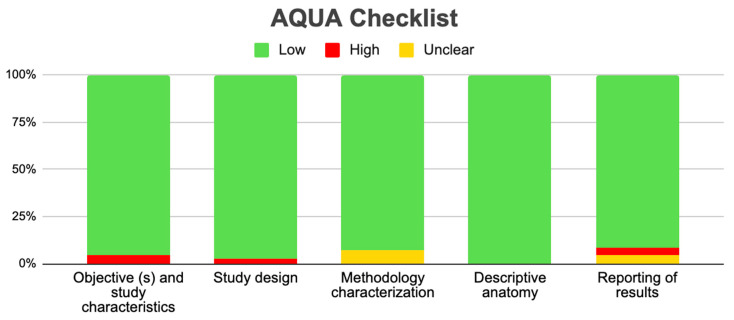 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPolymer crystallization and properties
1. Introduction
The heart is supplied primarily by two branches of the ascending aorta, the left coronary artery (LCA) and the right coronary artery (RCA). As its name suggests, the LCA is responsible for supplying the left side of the heart, starting its journey from the left coronary sinus (LCS) or the left sinus of Valsalva (LSV) and then dividing into the anterior interventricular artery or left anterior descending artery (LAD) and the left circumflex artery (LCx). On the contrary, the RCA begins its journey through the right coronary sulcus (RCS) or the right sinus of Valsalva (RSV), passing to the anterior atrioventricular sulcus to then anastomoses with the LCx, thus supplying the right side of the heart. Although the pathways described are most common for the LCA and RCA, anomalous or different origins can occur, as well as changes in their destination, location, or shape [1,2].
Different types of coronary anomalies can be described and classified according to their origin, course, and termination, or by hemodynamic alterations. However, these anomalies are caused by an alteration at the embryonic level (congenital defect) during the early development of the coronary arteries. In these cases, proper growth of the fetus can be affected or cause sudden death. The most common anomaly is an anomalous LCA originating from the pulmonary artery (PA), which is characterized by the origin of the LCA in the PA instead of the LCS. This syndrome is more common in infants and often presents with accompanying symptoms. At the same time, it is less common in adults and is usually asymptomatic. Other existing variants are abnormalities in the LCx, abnormalities in the RCA, LCA, the left main coronary artery (LMCA), and single coronary artery, among others [1,3,4].
Although there are various diagnostic methods for the detection of coronary anomalies, the use of computed tomography (CT) currently prevails, because this type of imaging indicates the arterial path from its origin to its destination with good resolution and without being invasive for the patient. Another effective but less frequent method is coronary angiography, which gives us a three-dimensional resolution of the arterial pathway, although this is more invasive and has a high economic value, which makes it less accessible [5,6,7]. The literature describes the prevalence of coronary artery anomalies as rare (0.21–5.79%). Due to the greater sensitivity of tomographic studies, these anomalies are more commonly observed using these imaging methods compared to conventional angiography [8,9].
Although the precise reason why the anomaly occurs is unknown, it carries several risks for symptomatic people. If a coronary artery is affected, blood flow in the myocardium can be hindered and can cause myocardial ischemia, and in the worst cases, sudden death. The most frequent symptoms can be fainting during physical activity, respiratory problems, heart problems, and chest pains, which is why people who suffer from this disease and practice intense physical activities are more likely to die from this anomaly [10,11,12,13].
This review aimed to determine the characteristics of coronary artery variants and their relationship with cardiac clinical considerations.
2. Methods
2.1. Protocol and Registration
To carry out this meta-analysis, we were guided by the Prisma statement [14]. The registration number in the Systematic Reviews Registry (PROSPERO) is CRD42024520734.
2.2. Electronic Search
To obtain the best studies that fit our research question, we searched the following databases in January: MEDLINE (via PubMed), Google Scholar, Web of Science (WOS), Cumulative Index to Nursing and Allied Health Literature (CINAHL), Latin American and the Caribbean Literature in Health Sciences (LILACS), and Scopus from their inception until March 2024. Our Search strategy included a combination of the following terms: “coronary artery” (Not Mesh), “left coronary artery” (Not Mesh), “right coronary artery (Not Mesh), “origin anomalous coronary artery” (Not Mesh), “clinical anatomy” (Not Mesh) and “anatomical variation”(Not Mesh), using the Boolean connectors AND, OR, and NOT (Supplementary Table S1).
2.3. Eligibility Criteria
As eligibility criteria, studies that included the presence of origin coronary artery (OCA) variants and their associations with some clinical conditions were included. They were considered eligible for inclusion if the following criteria were met: (1) Sample: dissections or images with the presence of the OCA variation; (2) Results: prevalence of subjects who presented OCA variants and their correlation with pathologies of the cardiac region; (3) Studies: This systematic review included research articles, retrospective and prospective observational types, published in English in peer-reviewed journals and indexed in the reviewed databases.
As exclusion criteria, we used the following to eliminate studies from our selection: (1) sample: studies carried out in animals; (2) studies that analyzed variants of the region or system outside the hepatic region or its drainage area or tract; (3) studies including letters to the editor or comments.
2.4. Study Selection
To make a thorough selection of the studies, we analyzed three authors independently. In the first instance, two authors (Valenzuela JJ and Escalona C) examined the titles and abstracts of the references recovered from the database searches. For the selected studies, the full texts of the references that any of the authors considered potentially relevant were obtained. A third reviewer (Quivira A) was involved if a consensus could not be reached. For this purpose, we also performed the agreement test between authors, the kappa test, to analyze reliability and the risk of bias between observers, which in this case gave 0.80, which is interpreted as good agreement.
2.5. Data Collection Process
Two authors (Nova P and Orellana M) independently extracted data on the outcomes of each study. The following data were extracted from the included studies: (a) authors and year of publication, (b) example total n and age, (c) prevalence, (d) characteristics of variant, (e) region geography, (f) sex of the sample, and (g) clinical considerations.
2.6. Assessment of the Methodological Quality of the Included Studies
To evaluate the bias of the included studies, we used the verification table for anatomical studies (AQUA) proposed by the International Working Group on Evidence-Based Anatomy (IEBA) [15]. Two reviewers (Valenzuela JJ and Nova P) independently analyzed the five domains proposed by the AQUA tool, reached a consensus and constructed the table and bias graph.
2.7. Statistical Methods
The data extracted from the meta-analysis were interpreted by calculating the VAH prevalence using JAMOVI software 2.1212 (https://www.jamovi.org/ accessed on 4 January 2024). The DerSimonian–Laird model with a Freeman–Tukey double arcsine transformation was used to combine the summary data. In addition, a random effects model was used because the VAH prevalence data were highly heterogeneous. The degree of heterogeneity between the included studies was assessed using the chi^2^ test and the heterogeneity (I^2^) statistic. For the chi^2^ test, the p-value proposed by the Cochrane collaboration was considered significant at 0.10. Values of the I^2^ statistic were interpreted with a 95% confidence interval (CI) in the following way: 0–40% might not be important, 30–60% might indicate moderate heterogeneity, 50–90% might represent substantial heterogeneity, and 75–100% could represent a significant amount of heterogeneity.
3. Results
3.1. Selection of Articles
The search process yielded a total of 795 articles from various databases, aligning with the criteria and search terms established by our research team. A filtration process was applied, focusing on the titles and/or abstracts of these articles. Out of the initial pool of 70 articles included, 39 articles were selected for inclusion in the meta-analysis. These articles were chosen based on their comprehensive study of the sample, detailed statistical data for each variant, and their utilization of a clear methodology.
Conversely, eight articles, primarily consisting of clinical case reports, were excluded from the meta-analysis. These reports, while offering valuable clinical and anatomical insights, primarily detailed individual cases and thus lacked the broader statistical foundations required for substantive analysis of the variables. However, these case reports were still considered valuable for the clinical and anatomical aspects of this study.
The total sample size encompassed 54,588 individuals. For the meta-analysis, 51,244 participants, derived from the 39 selected articles, were included. This sample comprised patients, imaging studies, and donor specimens (Figure 1).
3.2. Characteristics of Included Studies
A total of 70 studies that met our inclusion criteria were included in this review; they had a cumulative N of 578,868 subjects. Within these 70 studies, 38 met the criteria for the prevalence meta-analysis [2,5,6,7,10,12,13,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72]. Conversely, according to the variants reported by the studies, three reported variants in the origin of the branches of the RCA, 17 reported variants in the origin of the branches of the LCA, and 43 reported variants directly from the coronary artery. However, only 34 subjects out of 7400 reported anatomical variants in the LCA, while only 28 out of 1750 subjects reported variants in the RCA.
Geographically, 34 of the studies came from Asia, 2 from the African continent, 2 from South America, 14 from North America, and 14 from the European continent. In addition, the average age of the subjects studied was 28 years, with a standard deviation of 24 years. There were 8048 male subjects and 5723 female subjects, while 565,097 subjects had no reported sex (Table 1).
3.3. Description of Variants
When discussing anomalies of origin, the affected segment at the beginning of the coronary artery is examined. It can have a high or low origin, with an incidence of 6%. The coronary ostium, located at the lower end of the coronary sinus, is called the low origin, and the coronary ostium located 5 mm from the valvular attachment point of the aortic annulus is called the coronary commissure ostium. A high-origin ostium refers to an origin more than 10 mm away from the sinotubular junction. It is more common for the right coronary artery to have a high ostium of origin, which can be benign but hemodynamically significant. Likewise, multiple ostia are present in 0.41–0.43% of the population and present as ostia separated from the LCx and the LAD [40]. The single coronary artery, on the other hand, comes from the aortic sinus. It is usually benign, follows the course of the LAD or RCA, and may divide into two or three main branches after its onset. If there is an interarterial pathway between the PA and the aorta, the risk may increase. In coronary artery anomalies of PA origin, the most common form is the left coronary artery anomaly of the PA (ALCAPA), in which the left principal coronary arteries (TCI) arise from the PA. It occurs in 1 in 300,000 live births, and 90% will die within the first year of life if left untreated. Another abnormality is the RCA arising from the PA (ARCAPA); here, the ostium of the RCA arises from the PA. It is rarer and usually asymptomatic. There is also atresia or congenital stenosis of the ostium, which is rare and corresponds to a congenital malformation of the coronary artery, in which there is partial or complete occlusion of the RCA or LCA, which has been associated with hypoplasia of the proximal segment of the corresponding coronary artery (Figure 2).
On the other hand, there are also anomalies regarding the origin of a coronary artery or one of its branches in the opposite sinus or the non-coronary sinus. These anomalies can present in four types. The intra-arterial, which occurs between the pulmonary artery and the aorta, is the most important clinically since it is the most common cause of sudden death in athletes. The other three courses are retroaortic, prepulmonary, and transseptal, all of which are benign. Regarding course abnormalities, we recognize the intramyocardial course (myocardial bridge) in which the coronary artery tunnels into the heart muscle. In most cases, it is a benign and asymptomatic variant. It is described as complete if part of the coronary artery is lined by muscle bundles, or incomplete if only one layer of fibres covers the coronary artery. The different types of bridges are right ventricle, deep septal, and superficial bridges, which can be complete or incomplete (Figure 3).
Another anomaly is the duplication of the LAD and the divided RCA, which is a benign variation, where the RCA arises from two ostia or arises from one ostium and divides into two arteries after its origin. Split LCA is extremely rare, so the incidence of LAD duplication is 1% and has been documented only in sporadic cases. There are four types of duplications depending on the trajectory. There is the long distal anterior descending artery that runs along the left side of the interventricular sulcus, the long distal ADA that runs on the right side of the interventricular sulcus, the long distal ADA that has an intramyocardial course in the septum and appears on the epicardial surface in the distal part of the interventricular sulcus, and the long distal ADA that originates from the coronary artery (CA). Finally, coronary ectasia or aneurysm is defined as an enlargement or dilation of at least 1.5 times its normal diameter. If the entire blood vessel is affected, it is called ectasia, while if it is only partially affected, it is called a coronary aneurysm [20]. Congenital symptoms are very rare and commonly occur as a result of Kawasaki disease or a coronary artery fistula.
Regarding termination anomalies, we found three types: Coronary arterial fistula, which treats the abnormal termination of a coronary artery in the ventricle, the cardiac vein, or the PA [27]. The RCA is affected in 44% of cases, the left main coronary artery (LAB) in an additional 44%, and both TCI and RCA in 12% of cases [61]. Then there is the extracardiac or systemic termination, which is a termination anomaly that must be distinguished from a coronary fistula. This is because, in the fistula, the coronary artery is dilated and tortuous, unlike the systemic endings that do not have this pattern since there is no significant pressure difference between the coronary artery and the systemic artery to which it empties. Finally, the coronary arch is a direct connection between two main coronary arteries without the need for occlusive injury. Anatomical continuity has been reported, especially between the LCx and the RCA.
3.4. Prevalence and Risk of Bias
To calculate the prevalence of OCA variants in the studies included in this review (Table 2), one proportion of forest plots was made. To include the studies in the prevalence forest plot it was taken into account that the studies had to have reported a proportion of at least 10%. A total of 38 studies that met the criteria were included for variants of the OCA [2,4,6,11,12,13,19,20,21,22,26,27,28,33,34,37,45,49,51,55,56,57,62,63,64,65,66,67,68,69,73,74,75,76,77,78,79]. The Forest plot diagram showed that the prevalence was 1%, with a confidence interval of 0.8–1.2% (Figure 4 and Table 2). For this third sample, the funnel plot graph showed an important asymmetry, which had a p-value of 0.162 and is directly associated with this asymmetry (Figure 5).
A total of 70 studies met the criteria to be evaluated using the AQUA Checklist for anatomical studies tool in which bias was analyzed in five domains. In the five domains offered by the AQUA Table, the three included studies presented a low risk of bias and were analyzed across all the domains (Figure 6).
3.5. Clinical Considerations
Several theories attempt to explain the mechanisms that generate cardiac ischemia. In sudden cardiac death, it has been proposed that the mechanism of ischemia is the production of a transient or sustained spasm in the muscular layer of an anomalous coronary artery since sudden cardiac death is the main manifestation of the variation of the coronary arteries or their origin. This has been attributed to the endothelial damage of the blood vessel, which in turn has been directly associated with the abnormal trajectory and OCA. Finally, other authors showed that an intussusception of the proximal part of the CA into the aortic wall occurs. This anomaly only gives symptoms in 20% of patients since in the other patients it can be present without producing any type of damage or symptomatology. If the symptoms are present, they will manifest as dyspnea with associated syncope or some type of angina such as exertional angina. Another theory that explains the signs and symptoms in variants of AC is that they appear when an angulated location is presented by the anomalous AC in their ascending aortic artery exit. The difference with a normal AC is that the AC with variant has a location more perpendicular to the aorta, while the abnormal AC must be adapted so that it “flexes” on itself to reach from the sinus of the contralateral leaflet to its irrigation territory [19,38,46,61,71]. The clinical presentation is variable, ranging from asymptomatic patients to patients with angina, dyspnea, and syncope, either at rest or with exercise, acute myocardial infarction, heart failure, and sudden death. It has been observed that when symptoms are present in patients under 30–35 years of age there is an increased risk of sudden death, and in up to 40% of cases, symptoms that manifest during or immediately after physical activity precede death [16,28,35,39,46,53,62,71,78,79,80,81]. As they are mostly asymptomatic, the diagnostic reference standard is coronary angiography, and more imaging findings are made incidentally when performing imaging studies for other causes [25,46,73,79,81]. Coronary anomalies occur in 1.7% of the general population and cause sudden deaths in 33% of the young population during strenuous effort; the use of imaging techniques to diagnose these variants has grown [64,71,73]. Coronary artery anomalies can be classified according to Greenberg as anomalies of origin, course, and termination. However, one of the factors that most influence the classification is whether it has a hemodynamic impact.
4. Discussion
It was found that most of the subjects under study came from an Asian lineage, so there may be a predominance of certain anomalies based on nationality; however, there are no studies that support this association. If we talk about the age of the subjects in whom coronary anomalies were studied, the average age was 28 years, which means that this condition is detected mostly in adult subjects. In this study, we cannot infer whether these anomalies are related to or are more present in male or female subjects since the subjects’ reports did not place much importance on sex. Regarding the variants most present in this study, it was possible to visualize an abundance of origin-type anomalies, i.e., cases of anomalous origins of the coronary artery are more frequent than anomalies in its route or termination.
Regarding previous studies that have analyzed the variants of the origin of AC, our search only found three studies that met the criteria similar to the objectives set out in this review. The first study, and the one that presents the greatest similarity to ours, is that of Ponzoni et al. 2022 [81], which showed in its results the outcome of surgeries in variants of anomalous aortic origin of coronary arteries in children and young adults (<30 years). Thirteen publications, including a total of 384 patients, were selected. Surgical treatment of the anomalous aortic origin of the coronary arteries can be achieved with excellent results in pediatric patients, but concerns persist about the durability of the surgery, which could be a trigger for future pathologies. In addition, we conducted an exhaustive study of the anatomical considerations of anomalous OCA. Finally, we associated all the above with important clinical considerations that must be taken into account in the presence of this variant. On the other hand, the D’Ascenzi, 2022 [79] study, although it did not show the anatomy of AC, states that deaths from heart attacks could be associated with variants in the origin of AC. Although these characteristics are associated with the clinic, this study does not detail the anatomy or how the variant can produce cardiac pathologies. Finally, the Koppel, 2020 [35] review found the prevalence of coronary anomalies in tetralogy of Fallot to be 4–6%. In patients with an abnormal coronary artery, 72% cross the abnormal outflow tract of the right ventricle. The combined risk of finding an anomalous coronary artery or a large cone artery crossing the right ventricle is 10.3%. The coronary anatomy should be defined before surgery and the surgical approach should be adapted if necessary. Although this review makes a detailed analysis of the anomalous origin of AC in the presence of a tetralogy of Fallot, our study analyzes all the pathologies reported in studies with variants and the number of our studies and subjects is greater, which is why our study is novel.
Both the number of studies and the number of subjects investigated were considerable—more than 550,000 accumulated from all the studies—and shows that this anatomical variant is frequently studied and reported in the literature. If we focus on the data obtained in this study, most came from Asia, which could lead us to think that this variant is associated with races from the Asian continent. However, we have not found any study that supports this theory, so we believe that the greater number of studies in this continent is associated with the availability of samples and studies carried out in that section of the world. Regarding the characteristics of the sex of the sample, we cannot make a direct relationship between this variable and the presence of variation in the origin of the CA. This is because most of the studies included in this review did not indicate the sex of the subjects, with more than 500,000 subjects not reporting the sex of the subjects. The sex of 13,771 subjects was reported, which is equivalent to only 2% of the total sample. Among these subjects, there were 8048 men and 5723 women; therefore, we are categorical that for this study a relationship between sex and the presence of variants in the origin of AC cannot be attributed. On the other hand, according to the variants reported, most of the studies presented direct variants of the OCA. In addition, most of the cases were bilateral, that is, this anomaly occurred in both the LCA and the RCA. Another point is the average age of the subjects studied, which was 28 years, highlighting the early age of recognition of this variant since it causes symptoms in many subjects and great attention must be paid to the presence of variants in the origin of AC.
In the heart, the coronary arteries arise from the aortic wall from a plexus or peritoneal ring that connects to the systemic circulation; however, when this does not occur as it should, an anomaly, which does not have a clear definition, is formed. Despite this, a pattern has been used to classify variants found in the coronary tree; these are based on clinical significance or anatomical and functional characteristics. They are anomalies of origin, which in turn are divided into high and low origin, multiple ostia, single coronary artery, anomalous origin of coronary artery in the pulmonary artery, origin of a coronary artery or one of its branches in the opposite sinus or the non-coronary sinus, with abnormal course, atresia, or congenital stenosis of the ostium; course anomalies that in turn are divided into atresia or congenital stenosis of the ostium, duplication of LAD and divided RCA, ectasia or coronary aneurysm; and termination anomalies that include coronary arterial fistula, extracardiac or systemic termination, and coronary arch.
Anomalies of the coronary arteries are rare in the general population; however, the most frequently found are anomalies of origin and those of the trajectory of the central segments, that is, one is born with one of the coronary arteries from the opposite coronary sinus. The most common variant was the ectopic origin of the RCA from the LSV or the proximal LCA, and the main route was the intra-arterial route (Harikrishnan et al., 2002; Schmitt et al. 2005; Eid et al. 2009; Yildiz et al. 2010 [13,29,53,70]). The prevalence of the variants in the origin of AC was very low; cumulatively, it was less than 1%, indicating that this variant occurs in isolation. In this study, we did not separate the prevalence by different variants since if we had conducted this exclusion, the samples would have been very heterogeneous and limited. Measuring the bias of inclusion in the meta-analysis of the studies using a funnel plot showed symmetry in most of the included studies; thus, it can be said that the statistical analysis was relevant. On the other hand, the bias in the methodology was measured using the AQUA tool.
Because the coronary arteries are responsible for transporting oxygenated blood to the heart muscle, any morpho-functional alteration could cause reduced oxygen and nutrient transport to the heart. We have seen that defects in the origin of the coronary arteries can be multiple, but those closely related to the origin of heart irrigation can cause the most alterations. Therefore, anomalies in the RCA and LCA could potentially cause the most significant alterations. A coronary artery defect can present with a wide spectrum of clinical manifestations. Due to the various types of anomalies that can occur at the origin of the coronary arteries, some patients may be asymptomatic, while others may experience atypical anginal chest pain, syncope, dyspnea, angina, heart failure, acute heart attack, or even sudden death in severe cases. Symptoms have been mostly associated with young adults than the elderly. Additionally, cases of death, although occurring in adults, often happen at an early age, as reported in the literature, and are often associated with syncope at an early age. This could be linked to dietary alterations, lifestyles involving alcohol and drugs, and infrequent medical check-ups. Therefore, early diagnosis suggests periodic follow-up of these patients.
5. Limitations
This review was limited by the publication and authorship bias of the included studies. First, studies with different results that were in non-indexed literature in the selected databases may have been excluded. Second, there could be limitations in the sensitivity and specificity of the searches. Finally, the authors selected articles personally. All of these increase the probability of excluding potential cases from countries outside of Asia and North America that are not reported in the scientific community.
6. Conclusions
An anomalous origin of the variants of AC is a variant that has a low prevalence but has been exhaustively studied in the scientific literature. In this study, we found that the presence of this variant in AC could cause symptoms of high clinical significance, reaching the point of being a cause of death. For this reason, we believe that the knowledge of cardiac surgeons is crucial in avoiding functional and irrigation alterations. It is recommended that patients whose diagnosis was made incidentally and in the absence of symptoms undergo periodic controls to prevent future complications, including death. Finally, we believe that further studies could improve the anatomical, embryological, and physiological understanding of this variant in the heart.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Al-Dairy A. Rezaei Y. Pouraliakbar H. Mahdavi M. Bayati P. Gholampour-Dehaki M. Surgical Repair for Anomalous Origin of the Right Coronary Artery from the Pulmonary Artery Korean Circ. J.20174714414710.4070/kcj.2016.017428154604 PMC 5287178 · doi ↗ · pubmed ↗
- 2Han P.L. Diao K.Y. Huang S. Gao Y. Guo Y.K. Yang Z.G. Yang N. Anatomical characteristics of anomalous left coronary artery from the opposite sinus (left-ACAOS) and its clinical relevance: A serial coronary CT angiography study Int. J. Cardiol. Heart Vasc.20203110064910.1016/j.ijcha.2020.10064933088901 PMC 7558218 · doi ↗ · pubmed ↗
- 3Ismail M. Jijeh A. Alhuwaymil R.M. Alahmari R. Alshahrani R. Almutairi R. Habshan F. Shaath G.A. Long-Term Outcome of the Anomalous Origin of the Left Coronary Artery from the Pulmonary Artery (ALCAPA) in Children after Cardiac Surgery: A Single-Center Experience Cureus 202012 e 1182910.7759/cureus.1182933409071 PMC 7781494 · doi ↗ · pubmed ↗
- 4Jegatheeswaran A. Devlin P.J. Williams W.G. Brothers J.A. Jacobs M.L. De Campli W.M. Fleishman C.E. Kirklin J.K. Mertens L. Mery C.M. Outcomes after anomalous aortic origin of a coronary artery repair: A Congenital Heart Surgeons’ Society Study J. Thorac. Cardiovasc. Surg.2020160757771.e 510.1016/j.jtcvs.2020.01.11432800265 · doi ↗ · pubmed ↗
- 5Krupiński M. Urbańczyk-Zawadzka M. Laskowicz B. Irzyk M. BanyśR. Gruszczyńska K. Baron J. Computed tomography in the evaluation of the anomalous origin of the coronary artery: Coexistence with other congenital heart disease in an adult population Folia Morphol.201574737710.5603/FM.2015.001225792399 · doi ↗ · pubmed ↗
- 6Sidhu N.S. Wander G.S. Monga A. Kaur A. Incidence, Characteristics and Atherosclerotic Involvement of Coronary Artery Anomalies in Adult Population Undergoing Catheter Coronary Angiography Cardiol. Res.20191035836810.14740/cr 94131803334 PMC 6879043 · doi ↗ · pubmed ↗
- 7Sohrabi B. Habibzadeh A. Abbasov E. The incidence and pattern of coronary artery anomalies in the north-west of iran: A coronary arteriographic study Korean Circ. J.20124275376010.4070/kcj.2012.42.11.75323236327 PMC 3518709 · doi ↗ · pubmed ↗
- 8Ramírez F. Bitar P. Paolinelli P. Pérez D. Furnaro F. Congenital anomalies of the Coronary Arteries, study of those with Hemodynamic Importance Chil. J. Radiol.20182414215010.4067/S 0717-93082018000400142 · doi ↗