Malignant character of an ossified posterior longitudinal ligament in a hyperflexion injury: A case report
George Fotakopoulos, Vasiliki Epameinondas Georgakopoulou, Nikolaos Trakas, Pagona Sklapani, Alexandros G. Brotis

TL;DR
A 50-year-old man with cervical spine ossification suffered severe neurological issues after minor trauma, highlighting the potential severity of this condition.
Contribution
This is the first reported case of a lethal outcome following trauma in a patient with extensive cervical osteophyte due to OPLL.
Findings
The patient developed quadriparesis and respiratory insufficiency after minor head trauma.
This case highlights the potential for syncope and lethal outcomes in OPLL patients with significant canal stenosis.
Management of OPLL with canal stenosis should not be delayed unnecessarily.
Abstract
The present study reports the case of a 50-year-old obese male with ankylosing spondylitis, Scheuermann's kyphosis. The patient was asymptomatic concerning the ectopic ossification of the posterior longitudinal ligament (OPLL) at the cervical spine; he developed quadriparesis and respiratory insufficiency following minor head trauma. Even though trauma to the cervical spine in patients with OPLL is common, to the best of our knowledge, this is the first reported case of an extensive osteophyte with a lethal outcome after syncope. In rare occasions, it may be present with syncope and potentially lethal outcomes, particularly when precipitated by trauma. Therefore, the management of OPLL with significant canal stenosis should not be unnecessarily delayed.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
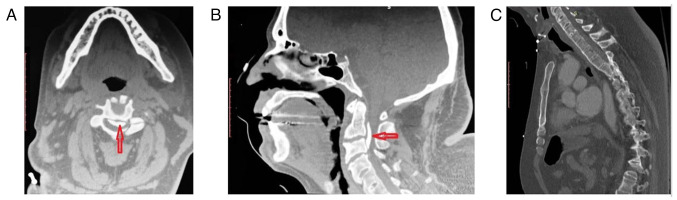 Figure 1
Figure 1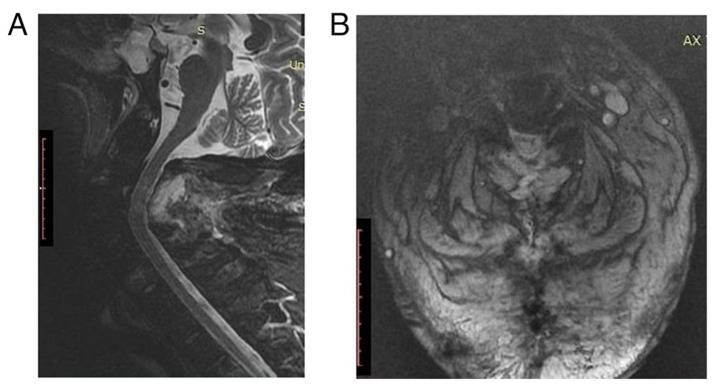 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCervical and Thoracic Myelopathy · Heterotopic Ossification and Related Conditions · Spinal Fractures and Fixation Techniques
Introduction
The ectopic ossification of the posterior longitudinal ligament (OPLL) represents a localized form of skeletal hyperostosis. Its annual incidence is as high as 3 and 1.3% for Asian and non-Asian populations, respectively (1). It frequently involves the cervical and thoracic spine to a lesser extent.
The nature of this chronic disease is generally benign. OPLL is commonly associated with significant stenosis of the spinal canal. The majority of patients present with myelopathy in the fifth and sixth decades of life. During the disease, up to 17% of the cases require some form of assistance in the activities of daily living. Patients are at an increased risk of developing quadriparesis following cervical spine trauma, reaching as high as 15% (1).
The present study describes the case of an asymptomatic patient with OPLL who developed quadriparesis and respiratory insufficiency following minor head trauma. The patient succumbed shortly afterwards due to a respiratory infection.
Case report
During hospitalization for a urinary tract infection, a 50-year-old obese male with ankylosing spondylitis (AS), Scheuermann's kyphosis (KS) and a body mass index of 42.4, lost consciousness and suffered a minor head injury at the occipital region. The immediate clinical examination revealed that the patient was hemodynamically stable (85 bpm and 123/85 mmHg) and febrile (39˚C) (from a urinary tract infection with pyospheres; a urine culture was positive for Escherichia. coli); he had sufficient respiration (SAO_2_, 97%). After 1-2 min, the patient regained consciousness but exhibit no contraction (0/5) in all key muscle groups and sensory paralysis during the neurological examination (ASIA A). A head computed tomography (CT) scan revealed no evidence of intracranial hemorrhage or other intracranial pathology and his Glasgow Coma Scale (GCS) score was 15/15. However, the CT scan of the cervical spine revealed an OPLL associated with severe spinal canal stenosis (canal diameter, 4.18 mm) and extensive anterior ankylosis (Fig. 1). After 30 min, the patient developed respiratory distress and was intubated using fiberoptic technology.
At that time, the patient was transferred to the University Hospital of Larissa (Larissa, Greece) with a cervical rigid collar. In the operating room, he underwent posterior cervical spine decompression with a laminectomy extending from C2 to C4. Following surgery, the patient was awakened and transferred to the intensive care unit for further cardiopulmonary support. The patient remained quadriplegic, with a minor improvement in the deltoid muscles (1/5). The post-operative magnetic resonance imaging scan documented the adequacy of decompression (Fig. 2). Additionally, it revealed a spinal cord with an increased signal intensity, compatible with edema. On the 6th day, the patient suffered a cardiac arrest, which he survived following half an hour of cardiopulmonary resuscitation. Moreover, a cardiac pacemaker was inserted to avoid future episodes. On the 11th day, the patient developed an acute abdomen following gastrostomy tube placement, for which he underwent an exploratory laparotomy. On the following day, the patient suffered a massive pulmonary embolism despite adequate anticoagulation and finally succumbed.
Discussion
Even though trauma to the cervical spine in patients with OPLL is common, to the best of our knowledge, this is the first reported case of an extensive osteophyte with a lethal outcome after a syncope (1,2). The most common presentation of OPLL is cervical myelopathy from the chronic narrowing of the spinal canal, followed by quadriparesis precipitated by trauma (1-4).
The association between the OPLL and syncope is not clear. Several pathogenetic mechanisms could be implicated. A vasogenic origin cannot be excluded following the compression of the anterior spinal arteries and blood stagnation in the vertebrobasilar system. It is unclear whether vertigo caused by vascular changes at the vertebrobasilar circulation causes syncope (5). Moreover, a neurogenic mechanism could be considered after an acute compression of the vagal and glossopharyngeal nuclei in the higher cervical region with parasympathetic over-discharge (5). Finally, the patient may have simply lost consciousness due to a hypotensive episode during an acute urinary tract infection or a latent arrhythmia.
In the present study, pre-operative imaging revealed an OPLL at the C1, C2, and C3 vertebral levels, corresponding to a continuous ossification based on the relevant classification pattern (1). Of note, two additional findings are worth noting, including a marked canal narrowing at the levels corresponding to the canal compromise and ankylosis of the subaxial spine compatible with AS (1,3). The co-existence of AS, KS and OPLL is infrequent, but both have been associated with human leukocyte antigen variants (1,3).
Symptomatic cases are usually treated surgically (1-3). Anterior procedures aim to remove the ossified ligament and directly decompress the spinal canal, but with a high risk of unintended durotomy (1-3). On the other hand, posterior approaches decompress the spinal canal indirectly (1,2). In the case presented herein, the posterior approach was preferred based on the level of the lesion and the curvature of the cervical spine. The K-line, a virtual line between the midpoints of the anteroposterior canal diameter at C2 and C7, fell behind the osteophyte, necessitating a posterior approach (6).
Studies have reported the association between obesity and hyperostosis situations resembling OPLL and diffuse idiopathic skeletal hyperostosis, where the mechanism of enormous cumulatively formed osteophytes remains unclear (7,8). However, the underlying mechanism may be connected with insulin-resistant states, and the surplus adipose tissue via mechanical, hormonal, and cytokine factors leads to bone upregulation (9,10).
In conclusion, OPLL is a rare disease that usually manifests with cervical myelopathy. In rare occasions, it may present with syncope and potentially lethal outcomes, particularly when precipitated by trauma. Therefore, the management of OPLL with marked canal stenosis should not be unnecessarily delayed. Further studies are required for the validation of the findings presented herein.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Matsunaga S Sakou T Ossification of the posterior longitudinal ligament of the cervical spine: Etiology and natural history Spine (Phila Pa 1976)37E 309E 314201210.1097/BRS.0b 013e 318241 ad 3322146284 · doi ↗ · pubmed ↗
- 2Head J Rymarczuk G Stricsek G Velagapudi L Maulucci C Hoelscher C Harrop J Ossification of the posterior longitudinal ligament: Surgical approaches and associated complications Neurospine 16517529201910.14245/ns.1938222.11131607083 PMC 6790740 · doi ↗ · pubmed ↗
- 3Abiola R Rubery P Mesfin A Ossification of the posterior longitudinal ligament: Etiology, diagnosis, and outcomes of nonoperative and operative management Global Spine J 6195204201610.1055/s-0035-155658026933622 PMC 4771496 · doi ↗ · pubmed ↗
- 4Hirai T Yoshii T Ushio S Mori K Maki S Katsumi K Nagoshi N Takeuchi K Furuya T Watanabe K Clinical characteristics in patients with ossification of the posterior longitudinal ligament: A prospective multi-institutional cross-sectional study Sci Rep 105532202010.1038/s 41598-020-62278-332218490 PMC 7099083 · doi ↗ · pubmed ↗
- 5Verma SK Yaseen M Bharadwaj V Pasha A Syncope: A rare presentation of Cervical spondylosis IOSR J Dent Med Sci 1390922014
- 6Ijima Y Furuya T Ota M Maki S Saito J Kitamura M Miyamoto T Ohtori S Orita S Inage K The K-line in the cervical ossification of the posterior longitudinal ligament is different on plain radiographs and CT images J Spine Surg 4403407201810.21037/jss.2018.05.2330069535 PMC 6046332 · doi ↗ · pubmed ↗
- 7Wu JC Liu L Chen YC Huang WC Chen TJ Cheng H Ossification of the posterior longitudinal ligament in the cervical spine: An 11-year comprehensive national epidemiology study Neurosurg Focus 30E 5201110.3171/2010.12.FOCUS 1026821434821 · doi ↗ · pubmed ↗
- 8Wang PN Chen SS Liu HC Fuh JL Kuo BI Wang SJ Ossification of the posterior longitudinal ligament of the spine. A case-control risk factor study Spine (Phila Pa 1976)24142144199910.1097/00007632-199901150-000109926384 · doi ↗ · pubmed ↗