Primary Tumor Characteristics as Biomarkers of Immunotherapy Response in Advanced Melanoma: A Retrospective Cohort Study
Rachel S. Goodman, Seungyeon Jung, Kylie Fletcher, Hannah Burnette, Ismail Mohyuddin, Rebecca Irlmeier, Fei Ye, Douglas B. Johnson

TL;DR
This study finds that patients with cutaneous melanoma respond better to immunotherapy than those with acral or unknown primary melanoma.
Contribution
The study identifies cutaneous melanoma subtypes as significant predictors of immunotherapy response and survival in advanced melanoma patients.
Findings
Cutaneous melanoma subtypes are associated with better progression-free and overall survival.
Acral and unknown primary melanomas show inferior response to immunotherapy.
Metastatic stage and BRAFV600E mutation are linked to worse outcomes.
Abstract
Melanoma survival rates have been vastly improved by the use of immune checkpoint inhibitors. However, some patients do not respond to the treatment or experience progression of disease. Because of this variability of response, markers predicting efficacy of these treatments is of interest. This study aimed to clarify the role of primary tumor characteristics in melanoma treatment and survival. The authors demonstrated that cutaneous melanoma and its subtypes were significantly associated with response, progression-free survival, and overall survival compared with acral or unknown primary melanoma. Other primary features did not demonstrate an association on multivariable analyses. Thus, primary features, other than cutaneous primary, should likely not influence metastatic treatment selection. Identifying patients likely to benefit from immune checkpoint inhibitor (ICI) treatment…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
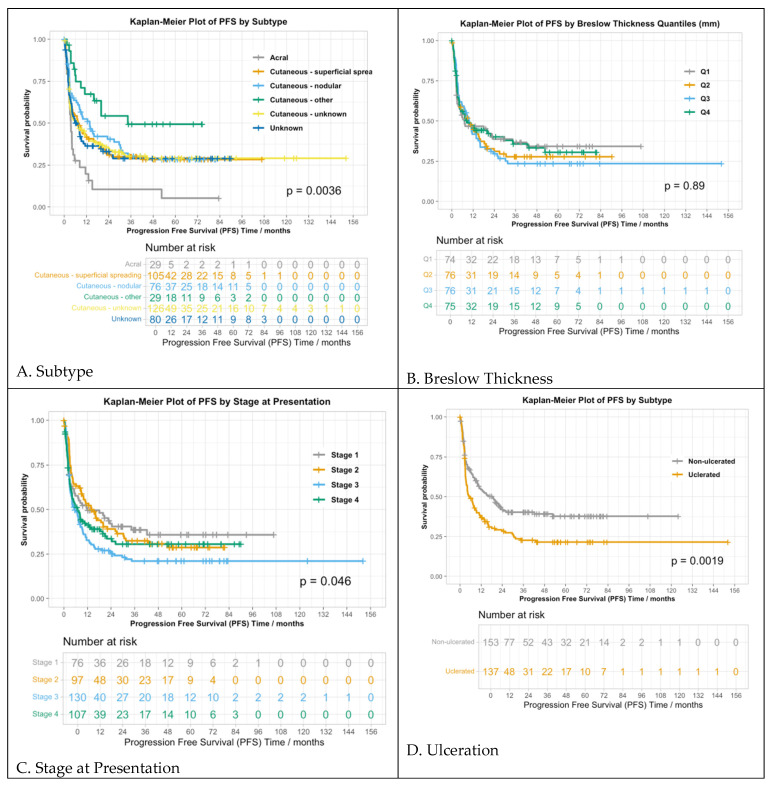 Figure 1
Figure 1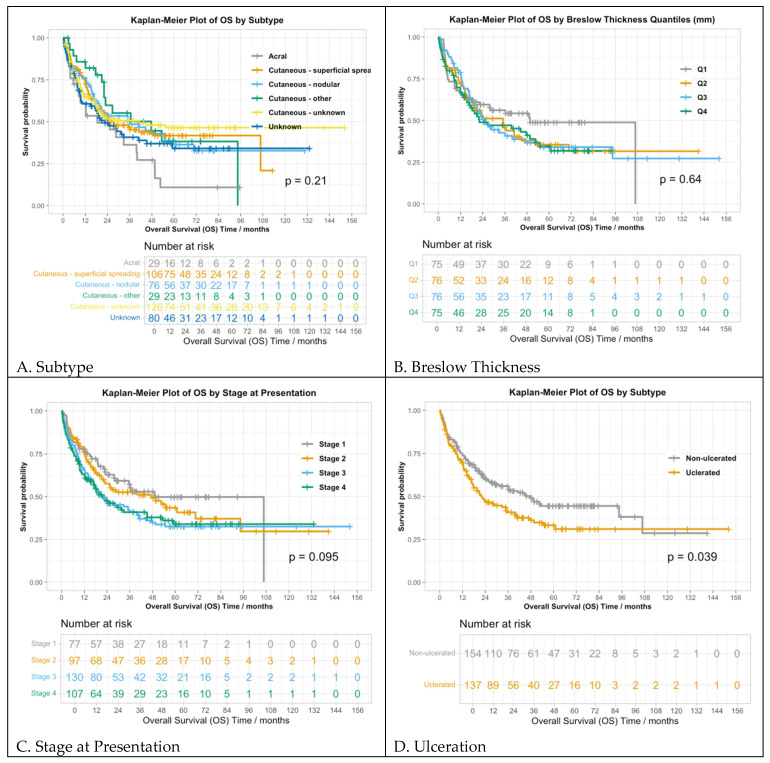 Figure 2
Figure 2| Response to Anti-PD-1 | |||
|---|---|---|---|
| Variable | Odds ratio | 95% CI | |
| SSM subtype | 6.50 | 1.8–23.45 | 0.004 |
| Nodular type | 10.48 | 2.850–38.50 | <0.001 |
| Other cutaneous type | 8.97 | 2.13–37.71 | 0.003 |
| Unknown subtype | 7.36 | 2.06–26.32 | 0.002 |
| Unknown primary | 7.07 | 1.90–26.33 | 0.004 |
| 1–2 positive sentinel nodes | 0.50 | 0.30–0.83 | 0.008 |
| 3+ positive sentinel nodes | 0.68 | 0.32–1.41 | 0.300 |
| BRAF mutation | 0.38 | 0.24–0.61 | 0.001 |
| PFS | |||
| Variable | Odds ratio | 95% CI | |
| SSM subtype | 0.58 | 0.36–0.94 | 0.026 |
| Nodular type | 0.53 | 0.33–0.86 | 0.010 |
| Other cutaneous type | 0.31 | 0.15–0.61 | <0.001 |
| Unknown subtype | 0.55 | 0.34–0.88 | 0.013 |
| Unknown primary | 0.50 | 0.28–0.88 | 0.016 |
| Ulceration | 1.24 | 0.92–1.66 | 0.162 |
| Mitoses | 0.99 | 0.97–1.01 | 0.202 |
| Stage II at presentation | 1.14 | 0.73–1.78 | 0.561 |
| Stage III at presentation | 1.42 | 0.93–2.16 | 0.103 |
| Stage IV M1a/b at presentation | 0.94 | 0.53–1.68 | 0.842 |
| Stage IV M1c/d at presentation | 1.79 | 1.07–3.00 | 0.027 |
| Male gender | 0.75 | 0.58–0.96 | 0.022 |
| Prior treatment | 1.04 | 0.91–1.20 | 0.542 |
| LDH > ULN | 0.92 | 0.79–1.06 | 0.236 |
| BRAF mutation | 1.64 | 1.27–2.11 | <0.001 |
| OS | |||
| Variable | Odds ratio | 95% CI | |
| SSM subtype | 0.58 | 0.35–0.95 | 0.029 |
| Nodular type | 0.65 | 0.39–1.09 | 0.105 |
| Other cutaneous type | 0.46 | 0.24–0.90 | 0.023 |
| Unknown subtype | 0.50 | 0.31–0.83 | 0.008 |
| Unknown primary | 0.71 | 0.42–1.19 | 0.196 |
| Age | 1.01 | 1.00–1.02 | <0.001 |
| Prior treatment | 1.14 | 1.02–1.27 | 0.015 |
| LDH > ULN | 1.04 | 0.93–1.16 | 0.474 |
| BRAF mutation | 1.38 | 1.04–1.84 | 0.028 |
- —SCRIPS Foundation, Burroughs Wellcome Fund
- —Medical Scholars, Vanderbilt University Medical Center
- —NCI
- —Susan and Luke Simons Directorship for Melanoma
- —James C. Bradford Melanoma Fund
- —Van Stephenson Melanoma Fund
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Immunotherapy and Biomarkers · Immunotherapy and Immune Responses · Cutaneous Melanoma Detection and Management
1. Introduction
The advent of immune checkpoint inhibitors (ICI) targeting cytotoxic T-lymphocyte-associated antigen 4 (CTLA-4) and programmed death 1 (PD-1) has transformed the management of advanced melanoma. Five-year survival has increased from 5% historically to >50% with combination immunotherapy [1,2]. While many patients exhibit durable responses, approximately half experience progression of the disease [3,4,5]. The variability in response remains unclear.
Despite the growing use of ICI across tumor types, there is a lack of well-defined prognostic or predictive markers of ICI efficacy and survival. While efforts have been made to identify factors associated with response (and lack thereof), such as tumor factors, immune microenvironment, and host factors [6,7,8,9,10,11,12], the impact of primary tumor characteristics on therapy response is unclear. One study found that primary melanoma thickness, ulceration, and stage were associated with brain metastases [13]. Thus, the primary tumor characteristics could reflect the underlying disease biology (e.g., hypoxia, immune response, aggressiveness) that impacts other aspects of metastatic behavior including the immunotherapy response. Another study demonstrated that primary melanomas located on sun-exposed skin treated with first-line anti-PD1 therapy had improved progression-free survival (PFS) compared to those on intermittently sun-exposed areas or sun-protected areas [14].
In this single-center retrospective cohort study, we assessed clinical features, primary tumor characteristics, response, and survival outcomes in 447 patients with unresectable or metastatic melanoma treated with ICI.
2. Methods
2.1. Overview
We conducted a single-center retrospective cohort study to assess the characteristics of primary melanomas and ICI outcomes. The study was approved by the Vanderbilt University Medical Center institutional review board. Patients receiving one or more doses of anti-PD-1 monotherapy or combination of ipilimumab and nivolumab were included. Patients with melanoma of mucosal or uveal origin were excluded due to their distinct tumor biology and published lower responses to anti-PD-1 [15,16,17].
2.2. Data Collection
Retrospective clinical data were collected, including date of initial diagnosis, anatomic site of primary, subtype (cutaneous, acral, or unknown primary), histologic subtype (superficial spreading [SSM], nodular, other, unknown), Breslow thickness, ulceration status (0/1), number of mitoses, presence of lymphovascular invasion (LVI), and tumor-infiltrating lymphocytes (TILs). The “other” cutaneous histologic subtype category aggregated multiple subtypes including desmoplastic, spindle cell, lentigo maligna, amelanotic, spitzoid, and balloon cell. Pre-immunotherapy treatment details, BRAF and other mutation status, number of positive sentinel nodes (0, 1–2, 3+), M status, and stage (AJCC 8th edition [18]) after the staging workup were collected. LDH level and stage (AJCC) at the time of immunotherapy initiation were collected. Immunotherapy outcomes were evaluated according to the therapeutic response (RECIST criteria), progression details, and date of last follow-up, which was defined as the date of last survival follow-up or death, whichever occurred later.
2.3. Statistical Analyses
Descriptive statistics were used to summarize patient and treatment characteristics. Univariate analyses assessed the association between each primary tumor characteristic and the response to ICI, progression-free survival (PFS), and overall survival (OS). Categorical variables and continuous variables were analyzed using a chi-squared test and a Wilcoxon rank-sum test, respectively. PFS and OS were tested using log-rank tests. Continuous variables were summarized by mean, median, and interquartile range (IQR). To estimate the independent effect of each clinical variable on the outcome, we conducted multivariable analyses using logistic regression for the response and Cox regression for the PFS and OS. In the Cox models, variables that did not meet the proportional hazard assumption were treated as time-dependent covariates, allowing their effect on the outcome to change over time. The multivariate analyses results were reported as odds ratios (ORs) or hazard ratios (HRs) with 95% confidence intervals (CIs). A backwards selection identified the independent variables that were most strongly associated with the outcome to avoid overfitting and improve model interpretation. To assess the impact of treatment, a reduced model without treatment status was compared to the full model using a likelihood ratio test. All of the statistical analyses were conducted using R v4.2.2.
3. Results
3.1. Patient and Primary Tumor Characteristics
A total of 447 patients (137 female [30.6%]; mean [SD] age, 60.9 [14.6] years) were included. Of these, 300 (67.1%) patients received anti-PD-1 monotherapy, and 147 (32.9%) patients received ipilimumab and nivolumab. BRAF^V600E^ mutations were present in 140 (31.3%) of patients, and 177 (39.6%) patients had elevated LDH at the start of treatment.
In total, 338 (75.6%) patients had cutaneous melanoma, 29 (6.5%) had acral melanoma, and 80 (17.9%) had melanoma of unknown primary (Table 1). Among the patients with cutaneous melanoma, 107 (23.9%) had SSM, 76 (17.0%) had nodular, 29 (6.5%) had another subtype, and 126 (28.2%) were unknown (subtype not specified, but cutaneous primary confirmed). “Other” cutaneous subtypes included lentigo maligna (N = 11, 37.9%), desmoplastic (N = 8, 27.6%) and spindle cell (N = 8, 27.6%). At initial presentation, the mean [SD] Breslow thickness was 4.2 mm [5.3], ulceration was present in 137 (30.6%) patients, the mean [SD] mitotic count was 6.5/mm^2^ [6.7], and LVI and TILs were present in 169 (37.8%) patients and 128 (28.6%) patients, respectively. One-hundred ninety (42.5%) patients had localized disease, 125 (27.9%) had regional disease, and 110 (24.5%) had metastatic disease at presentation.
An objective response rate (ORR; complete or partial response) occurred in 128 (42.7%) patients treated with anti-PD-1 and 69 (46.9%) for those who received ipilimumab and nivolumab (Table 2). The mean PFS [SD] was 19.3 months [26.5] for anti-PD-1, and 20.2 months [25] for the combination therapy. The mean OS [SD] was similarly comparable—31.1 months [30.9] for anti-PD-1 versus 28.7 months [25.1] for the combination therapy.
3.2. Univariate Analysis
3.2.1. Response to ICI
The melanoma site of origin, ulceration, number of positive sentinel nodes, and the stage at presentation showed significant associations with the ORR (Table 3). By site of origin, the ORR was 44.7% (151/338) for cutaneous, 10.3% (3/29) for acral, and 36.7% (29/79) for unknown primary (p < 0.01). The ORRs by subtype were as follows: 39.4% for SSM (43/109), 53% for nodular (41/78), and 55% for other types (16/29). The ORR in patients with ulceration was 35.8% (49/137) and 51.0% (79/155) for those without ulceration. The ORR was 53.2% (82/154) for those with 0 positive sentinel nodes, 28% (27/95) for 1–2 positive sentinel nodes, and 39% (12/31) for 3+ positive sentinel nodes (p < 0.01). For the stage, the ORR was 49.1% (86/175) for patients who initially presented with stage I/II melanoma and 35.3% (96/272) for patients presenting with stage III/IV melanoma (p < 0.01). The Breslow thickness (p = 0.3), mitoses (p = 0.5), LVI (p = 0.5), TILs (p = 1), and M status at presentation (p = 0.56) were not associated with the response.
3.2.2. Progression-Free Survival
Among all patients, the median PFS was 8.2 months (95% CI: 5.8–10.4, N = 445), 3.6 months for patients with acral melanoma (95% CI: 2.7–5.6), 7.6 months for SSM (95% CI: 4.3–16.2), 13.8 months for nodular (95% CI: 8.1–30.3), 34.3 months for other cutaneous subtype (95% CI: 16.02–NA), 7.2 months for unknown cutaneous subtype (95% CI: 3.6–13.1), and 7 months for unknown primary (95% CI: 4.1–11.3) (p < 0.01) (Figure 1A). The patients were categorized into four quartiles based on their Breslow thickness: Q1 (<1.4 mm), Q2 (1.4–2.7 mm), Q3 (2.7–5 mm), and Q4 (>5 mm) (Figure 1B). There was no significant difference in the PFS among the quartiles, with PFSs of 7.2, 9.6, 9.7, and 8.9 months for Q1–4, respectively (p = 0.9). The stage at initial disease presentation was associated with the PFS, with median PFSs of 11.8, 14.0, 5.6, and 7 months for stages I, II, III, and IV, respectively (p = 0.05) (Figure 1C). For the M status, the overall difference in the PFS was not statistically significant (p = 0.3), with median PFSs of 8.6, 18.4, 24.4, 5.3, and 5.7 months for M0, M1a, M1b, M1c, and M1d, respectively. The median PFSs were 5.2 months (95% CI: 3.7–9.4) and 18.4 months (95% CI: 10.0–26.2) in those with and without ulceration, respectively (p < 0.01) (Figure 1D). Other factors associated with PFS (or with nearly significant trends) included the number of positive sentinel nodes (p < 0.01), mitoses (p = 0.07), primary presentation (p = 0.06), and BRAF mutation (p < 0.01), whereas LVI (p = 0.1) was not associated with PFS.
3.2.3. Overall Survival
The median OS for all patients was 28 months (95% CI: 21.9–41.1), with 247 out of 446 patients (55%) having died before last follow-up. As with PFS, the OS was different between those with ulceration (21.9 months, 95% CI: 17.0–39.7) and without ulceration (47.7 months, 95% CI: 29.2–NA) (p = 0.02). Similarly, OS varied by M stage, with median OS values of 35.1, 45.3, not reached, 16.9, and 9.6 months for those with M0, M1a, M1b, M1c, and M1d, respectively (p = 0.04) (Figure 2D). The number of positive sentinel nodes was also associated with OS (p < 0.01).
OS analysis by subtype did not reveal statistically significant differences, with median OS values of 18.6, 27.4, 36.1, 47.7, and 41.1 months for acral, superficial spreading, nodular, other cutaneous, unknown cutaneous subtypes, and unknown subtype, respectively (p = 0.21) (Figure 2A). Moreover, the association between the stage at presentation and OS was not statistically significant (p = 0.10): the median OSs were 49.1, 47.2, 21.0, and 21.9 months for stages I-IV (Figure 2C). Other factors not associated with OS included LVI (p = 0.6), TILs (p = 0.1), Breslow thickness (p = 0.64), and BRAF mutation (p = 0.19) (Figure 2B).
3.3. Multivariable Analysis
3.3.1. Response to ICI
The multivariable analyses with backward selection revealed that gender, TILs, treatment, Breslow thickness, stage at presentation, M status, LVI, age, prior therapy, ulceration, mitoses, and elevated LDH were not significantly associated with the response to ICI (p > 0.05). In the reduced logistical regression model, the superficial spreading subtype (OR = 6.5, p < 0.01), nodular subtype (OR = 10.5, p < 0.01), other cutaneous subtype (OR = 9.0, p < 0.01), unknown cutaneous subtype (OR = 7.4, p < 0.01), and unknown subtype (OR = 7.1, p < 0.01) were associated with the response (reference group: acral). The BRAF^V600E^ mutation (OR = 0.4, p < 0.01) and 1–2 positive sentinel nodes (reference group: 0 positive sentinel nodes; OR = 0.50, p < 0.01) were negatively associated with the response. When treatment was added to the model, it was not a significant predictor of the therapeutic response (OR = 1.1, p = 0.7) and did not significantly affect the model likelihood ratio test or discrimination indexes. We also wondered whether the loss of association of ulceration with response was due to a more aggressive metastatic presentation in patients with ulceration. Ulceration was associated with higher metastatic stage at presentation with a marginally significant p-value (p = 0.06) but not with higher LDH (p = 0.45) (Table 4).
3.3.2. Progression-Free Survival
The backwards selection removed the number of positive sentinel nodes, TILs, Breslow thickness, age, LVI, and treatment from the model (p > 0.05). The reduced cox regression model showed that SSM (OR = 0.6, p < 0.05), nodular subtype (OR = 0.5, p < 0.05), other cutaneous subtype (OR = 0.3, p < 0.001), unknown cutaneous subtype (OR = 0.5, p < 0.05), unknown primary (OR = 0.5, p < 0.05), and male gender (OR = 0.7, p < 0.05) were associated with longer PFS. Metastatic stage (M1c, M1d) at presentation (OR = 1.8, p < 0.05) and BRAF^V600E^ mutation status (OR = 1.6, p < 0.001) were associated with shorter PFS. The presence of ulceration, mitoses, initial presentation stage (II, III, M1a, M1b), elevated LDH, and prior therapy were not associated with PFS.
3.3.3. Overall Survival
The number of positive sentinel lymph nodes, TILs, gender, LVI, Breslow thickness, treatment status, ulceration, mitoses, and M status were removed in the model selection for OS (p > 0.05). SSM (OR = 0.6, p = 0.03), other cutaneous subtype (OR = 0.5, p < 0.05), unknown cutaneous subtype (OR = 0.5, p < 0.01) were associated with longer OS while age (OR = 1, p < 0.001), prior therapy (OR = 1.1, p < 0.05), and BRAF^V600E^ mutation status (OR = 1.4, p < 0.05) were associated with shorter OS. The treatment type did not have an independent effect (p = 0.5).
4. Discussion
This is the first study to comprehensively assess whether primary tumor characteristics and initial presentation impacted the subsequent immunotherapy response in the metastatic setting. Though a more advanced stage of initial presentation, ulceration, and histologic subtype were associated with inferior outcomes in the univariate analyses, they were less or not significant in the multivariable analysis. Instead, cutaneous melanoma and each of its subtypes (superficial spreading, nodular, other, unknown) were significantly associated with improved clinical outcomes. Other features of the primary, including Breslow depth, TILs, mitoses, and LVI, did not impact the immunotherapy response after controlling for multiple variables.
There remains a need to identify the markers of response and survival to better select patients likely to benefit from ICI. The melanoma biology influences the immune response by regulating antigen expression and presentation, thereby playing a critical role in determining the likelihood of an immunotherapy response. The increased tumor cell expression of MHC-II and PD-L1, influenced by tumor infiltrating lymphocytes, has shown promise [19,20,21,22,23], although they remain imperfect [7,24,25]. A high tumor mutational burden (TMB) is a potential marker of response, although it has a limited predictive capacity [26,27]. Similarly, an inflamed tumor microenvironment, as expressed by CD8+ T cells and interferon-γ signatures, has also been correlated with a response to ICI therapies [28,29]. Therapeutic resistance has also been associated with transcriptional programs of mesenchymal differentiation, angiogenesis, and hypoxia, as well as JAK-STAT mutations [30,31]. While these biomarkers have promise, it is possible that the clinical and pathologic features of primary tumors could also have predictive value.
The ulceration and stage of presentation were associated with poorer PFS and OS in the univariate analyses, with similar but more modest effects seen with high mitotic rates, though these associations did not persist in the multivariable models. Thus, it is likely that factors like ulceration and a high mitotic rate are not only associated with higher rates of metastatic progression and death in the pre-ICI era [32] but also with other adverse metastatic features, such as visceral organ involvement, bulky disease, and high LDH, which correlate with ICI failure [33,34]. Indeed, ulceration was associated with higher metastatic stage at presentation with a marginally significant p-value, although not with higher LDH.
The lack of an independent association between most of the primary tumor features and outcomes following ICI therapy for metastatic disease suggests that these features may not have a major predictive role in this setting. However, they add valuable prognostic information following initial diagnosis. Since most of these adverse prognostic factors were identified prior to immunotherapy development, it is noteworthy that they presage not only inferior outcomes in an era lacking effective systemic therapies but also poor responses to active modern treatment options.
All of the cutaneous subtypes were more likely to respond compared with the acral melanoma, though “other” cutaneous subtypes (lentigo maligna, desmoplastic, spindle cell, etc.) had the longest PFS. Specifically, the ORR was greatest for the desmoplastic (N = 8, RR: 75%) and amelanotic subtypes (N = 3, RR: 67%), followed by lentigo maligna (N = 11, RR: 45%) and spindle cell (N = 8, RR: 38%). It is well known that the desmoplastic melanoma has a higher response in part due to its high mutation burden [35]. However, larger studies on less common atypical subtypes (such as amelanotic and lentigo maligna) Nare warranted to assess for other unexpected beneficial associations.
Several known prognostic factors were recapitulated. The metastatic stage (M1c, M1d) was associated with shorter PFS, while age and prior therapy correlated with shorter OS [36,37]. The BRAF^V600E^ mutation negatively impacted ICI response, possibly due to prior BRAF/MEK inhibitors in some patients. The optimal first-line regimen for BRAF-mutant melanomas remains contested, although it should consist of immunotherapy for most patients [38]. Ongoing studies aim to determine combination and sequence strategies (NCT02908672, NCT02967692, NCT02631447).
One prior study assessed primary tumor characteristics as potential biomarkers of immunotherapy response. LVI was significantly associated with an immunotherapy response and prolonged PFS and OS in advanced melanoma patients [39]. Our findings are somewhat in line with this, as LVI was associated with prolonged OS. Notably, our study has a significantly larger cohort and assessed multiple other clinical variables.
The limitations of this study included its retrospective and single-center nature, and relatively small sample size. Prospective, multi-center studies with a larger and more diverse sample size should be conducted to enhance generalizability.
These findings suggest that the clinical and pathological variables of primary tumors are associated with immunotherapy response, PFS, and OS in melanoma, though these do not appear to be independent of the adverse prognostic features of the metastatic presentation. Thus, primary features, other than cutaneous primary, should likely not be integrated in predictive models [40] for metastatic treatment, but may provide additional prognostic data surrounding initial presentation. Future research should aim to replicate and validate these results to help stratify patients by likelihood of response to ICI therapy.
5. Conclusions
Features of the primary tumor were associated with clinical outcomes when assessing as univariate analyses (primarily ulceration and initial stage of presentation). However, these associations were largely not significant after adjusting for known prognostic variables, with the exception of cutaneous histology vs. acral and mucosal primaries. This suggests that adverse prognostic features of initial presentation may correlate with later inferior outcomes with modern therapies, although these variables are captured with known prognostic features at the time of metastatic disease.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mangin M.-A. Boespflug A. Maucort Boulch D. Vacheron C.-H. Carpentier I. Thomas L. Dalle S. Decreased Survival in Patients Treated by Chemotherapy after Targeted Therapy Compared to Immunotherapy in Metastatic Melanoma Cancer Med.2021103155316410.1002/cam 4.376033932099 PMC 8124115 · doi ↗ · pubmed ↗
- 2Ernst M. Giubellino A. The Current State of Treatment and Future Directions in Cutaneous Malignant Melanoma Biomedicines 20221082210.3390/biomedicines 1004082235453572 PMC 9029866 · doi ↗ · pubmed ↗
- 3Wolchok J.D. Chiarion-Sileni V. Gonzalez R. Grob J.-J. Rutkowski P. Lao C.D. Cowey C.L. Schadendorf D. Wagstaff J. Dummer R. Long-Term Outcomes with Nivolumab Plus Ipilimumab or Nivolumab Alone Versus Ipilimumab in Patients with Advanced Melanoma J. Clin. Oncol.20224012713710.1200/JCO.21.0222934818112 PMC 8718224 · doi ↗ · pubmed ↗
- 4Patrinely J.R. Baker L.X. Davis E.J. Song H. Ye F. Johnson D.B. Outcomes after Progression of Disease with Anti-PD-1/PD-L 1 Therapy for Patients with Advanced Melanoma Cancer 20201263448345510.1002/cncr.3298432463489 PMC 7695037 · doi ↗ · pubmed ↗
- 5Wang D.Y. Eroglu Z. Ozgun A. Leger P.D. Zhao S. Ye F. Luke J.J. Joseph R.W. Haq R. Ott P.A. Clinical Features of Acquired Resistance to Anti-PD-1 Therapy in Advanced Melanoma Cancer Immunol. Res.2017535736210.1158/2326-6066.CIR-16-028728396509 PMC 5502536 · doi ↗ · pubmed ↗
- 6Bai R. Lv Z. Xu D. Cui J. Predictive Biomarkers for Cancer Immunotherapy with Immune Checkpoint Inhibitors Biomark. Res.202083410.1186/s 40364-020-00209-032864131 PMC 7450548 · doi ↗ · pubmed ↗
- 7Huang A.C. Zappasodi R. A Decade of Checkpoint Blockade Immunotherapy in Melanoma: Understanding the Molecular Basis for Immune Sensitivity and Resistance Nat. Immunol.20222366067010.1038/s 41590-022-01141-135241833 PMC 9106900 · doi ↗ · pubmed ↗
- 8Augustin R.C. Luke J.J. Rapidly Evolving Pre- and Post-Surgical Systemic Treatment of Melanoma Am. J. Clin. Dermatol.20242542143410.1007/s 40257-024-00852-538409643 PMC 11552441 · doi ↗ · pubmed ↗