Surgical Management of a Giant Inflammatory Hepatocellular Adenoma in a Young Female
Atl Simon Arias Rivera, Anaida Xacur Trabulce, Moises Brener Chaoul, Marco A De La Rosa Abaroa, Rafael Padilla Longoria

TL;DR
A young woman with a large inflammatory liver tumor underwent successful surgery and showed no signs of recurrence.
Contribution
Presents a rare case of giant inflammatory hepatocellular adenoma with successful surgical management and no recurrence.
Findings
Surgical removal via right hepatectomy was effective for the tumor.
The patient had no complications during hospitalization.
No recurrence was observed after eight months of follow-up.
Abstract
Hepatocellular adenomas are rare and benign primary neoplasms of phenotypically mature hepatocytes. Our understanding of this pathology has greatly improved due to advances in molecular and anatomic knowledge. This article provides an in-depth review of hepatic adenomas (HCA) while presenting the case of a 20-year-old patient with a giant inflammatory hepatocellular adenoma with an atypical presentation, in whom surgical intervention was performed via right hepatectomy. In the post-surgical course, the patient had an in-hospital stay of three days with no complications. During outpatient monitoring via laboratory tests and imaging at eight months, the patient did not present any trace of recurrence.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
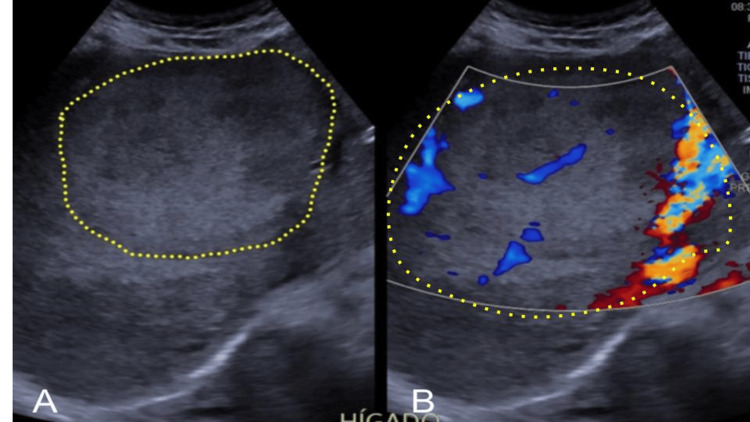 Figure 1
Figure 1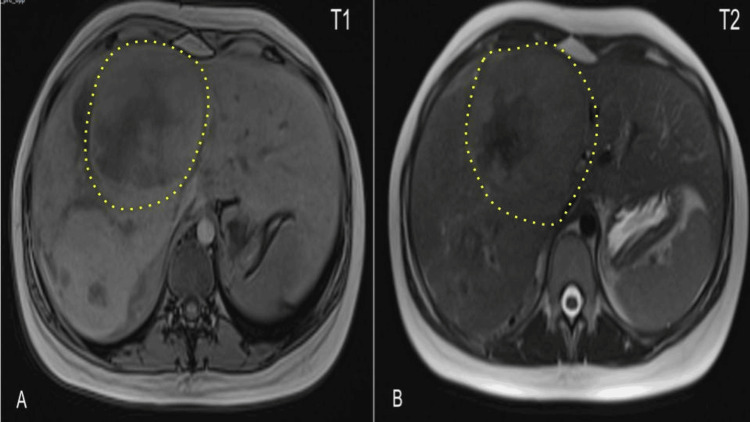 Figure 2
Figure 2 Figure 3
Figure 3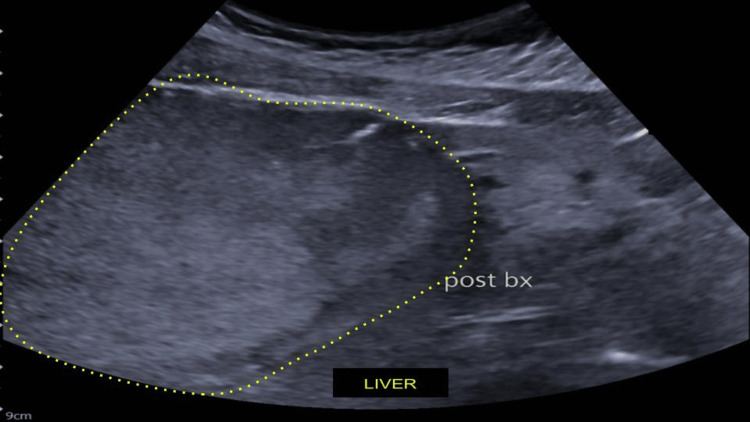 Figure 4
Figure 4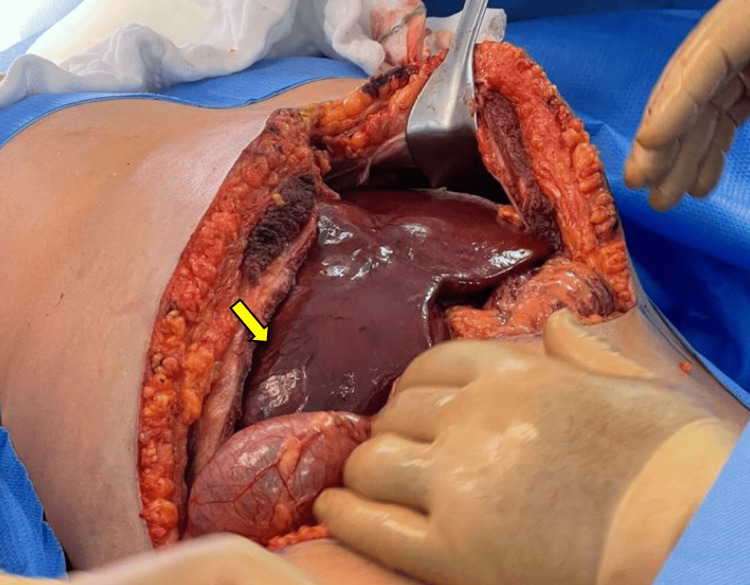 Figure 5
Figure 5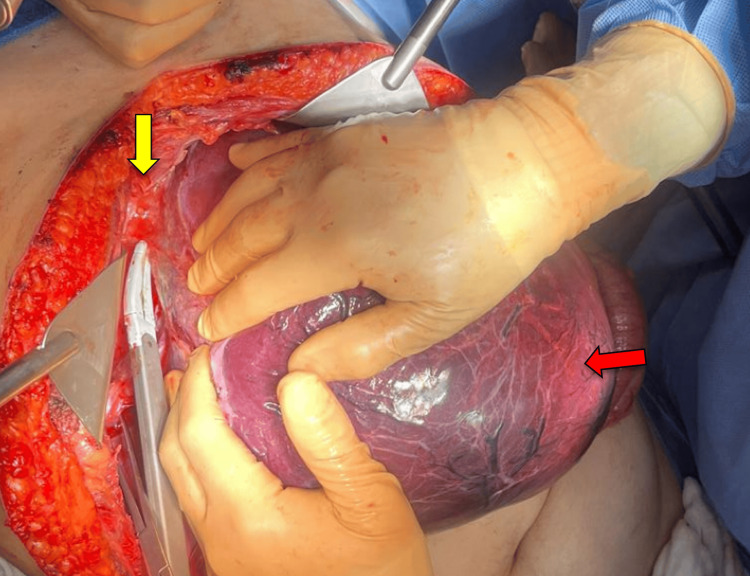 Figure 6
Figure 6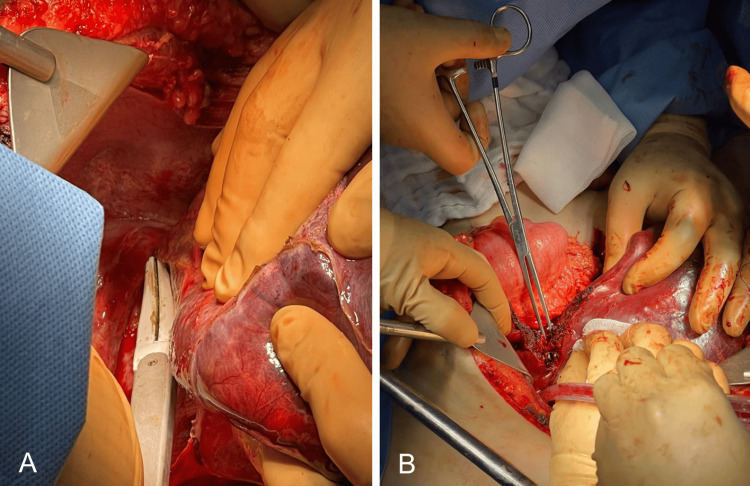 Figure 7
Figure 7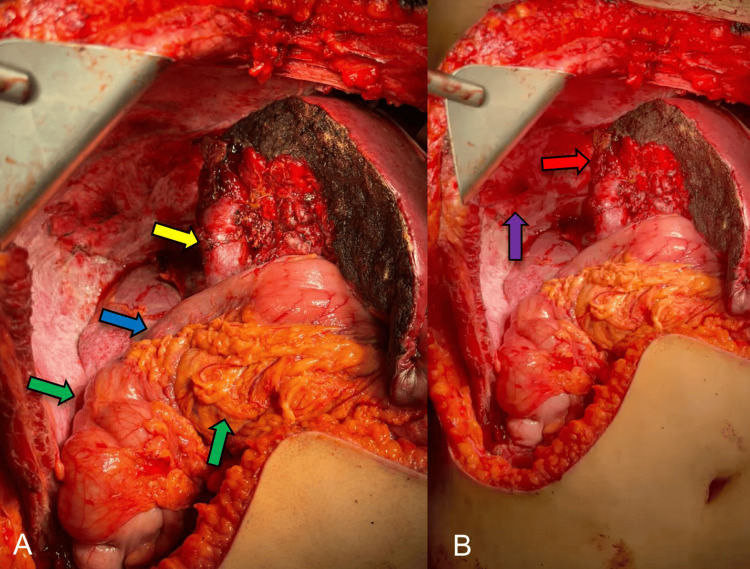 Figure 8
Figure 8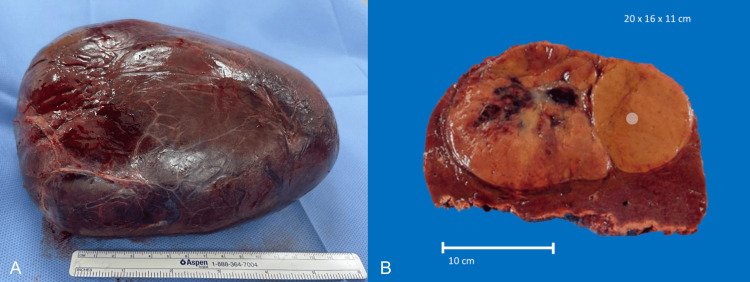 Figure 9
Figure 9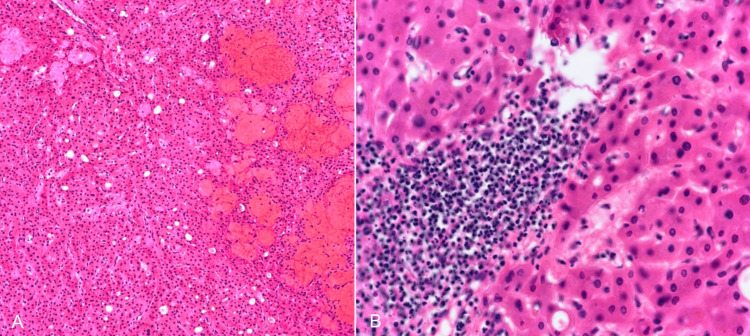 Figure 10
Figure 10| Tumor Marker | Result | Reference Range |
| Alpha-fetoprotein | 1.7 ng/mL | <8.8 |
| Carcinoembryonic antigen | 1.79 ng/mL | 0.00-5.00 |
| CA 19-9 | 17.7 U/mL | 0.0-37.0 |
| Laboratory test | Result | Reference Range |
| Hemoglobin | 11.96 g/dL | 12.00-16.00 |
| Hematocrit | 33.9% | 37.0-48.0 |
| WBC Count | 11,930 103/μL | 3.80-11.20 |
| Lymphocytes | 18% | 20-40 |
| Neutrophils | 65% | 40-70 |
| Stab neutrophils | 10% | 0.0-4.0 |
| Platelets | 262,000 103/μL | 130-450 |
| Glucose | 82.3 mg/dL | 74.0-99.0 |
| Urea | 9.5 mg/dL | 10.7-53.5 |
| Creatinine | 0.75 mg/dL | 0.60-1.60 |
| Uric acid | 2.9 mg/dL | 2.6-6.0 |
| Lactate dehydrogenase | 506.1 U/L | 125.0-243.0 |
| C-reactive protein | 6.42 mg/dL | 0.010-0.744 |
| Creatine phosphokinase | 4540.9 U/L | 29.0-168.0 |
| Alanine Aminotransferase | 317.7 U/L | 0.0-55.0 |
| Aspartate Aminotransferase | 407.3 U/L | 5.0-34.0 |
| Alkaline phosphatase | 237.0 U/L | 40.0-150.0 |
| Gamma-glutamyl transferase | 81.1 U/L | 9.0-36.0 |
| Total bilirubin | 1.09 mg/dL | 0.20-1.20 |
| Direct bilirubin | 0.50 mg/dL | 0.0-0.50 |
| Indirect bilirubin | 0.59 mg/dL | 0.0-1.00 |
| Amylase | 1032.5 U/L | 25.0-125.0 |
| Lipase | 35.7 U/L | 8.0-78.0 |
| International Normalised Ratio | 1.17 sec | 0.80-1.20 |
| Prothrombin time | 14.1 sec | 10.0-13.9 |
| Partial Thromboplastin time | 45 sec | 24.0-40.0 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCholangiocarcinoma and Gallbladder Cancer Studies · Hepatocellular Carcinoma Treatment and Prognosis · Liver Diseases and Immunity
Introduction
Hepatic adenomas (HCA), also known as hepatocellular adenomas, are rare and benign primary neoplasms. Hepatic adenomatosis is defined as the presence of more than 10 adenomas, with multiple lesions reported in 12% to 30% of cases. In the 1970s, after the introduction of oral contraceptives, the prevalence of liver cell adenomas (LCAs) increased since the pathogenesis is associated with steroid and anabolic hormone use. HCA can predominantly be found in young women aged between 20 and 40 years, with a female to male ratio of 11:1. They have an incidence rate of approximately 3 cases per 100,000 individuals [1-3].
The prevalence of symptoms in 50-75% of patients makes upper abdominal pain the most often observed symptom, usually associated with hemorrhage or local compression. Complications of this condition include bleeding, which occurs in 15-20% of cases, and malignant transformation, which occurs in 5% of cases. The 5-7 cm rise in tumor size necessitates the suggestion to surgically remove all HCAs that are greater than 5 cm [3-4].
There are five main subtypes of hepatocellular adenoma: HNF1a-inactivated HCA (HHCA), Inflammatory HCA (IHCA), β-catenin-activated HCA (BHCA), Sonic Hedgehog HCA (shHCA), and less than 5% of HCA will be unclassified because of the absence of molecular abnormalities or immunohistochemistry markers [4].
Major complications of hepatocellular adenoma include rupture, with an estimated risk of 30% to 50%, which mostly occurs in lesions 5 cm or larger. Hemorrhage can be managed with hepatic artery embolization. Malignant transformation is also possible; in the molecular-pathologic classification, the subtype with the highest risk of malignancy is the LCA with β-catenin activation. It is established that CTNNB1 oncologic mutations have the capacity to activate β-catenin at high, moderate, or weak levels, each predisposing to different tumor phenotypes and malignant progression [3-6].
We present a case of a 20-year-old patient with a giant inflammatory hepatocellular adenoma with an atypical presentation.
Case presentation
A 20-year-old female was referred to the surgical oncology department due to a hepatic mass. During the anamnesis, she denied any past utilization of oral contraceptives, alcohol intake, consumption of bee syrup, or history of hepatitis. Previously asymptomatic, after facing difficulties losing weight, she was taken by her mother to perform a routine blood test examination. Pancreatic function tests revealed a significant elevation in amylase (260 U/L) and lipase (566.2 U/L), with liver function tests within normal range.
During the clinical examination, a large palpable abdominal mass was discovered, approximately 15 cm in diameter. Subsequent abdominal ultrasonography revealed a solid, heterogeneous, irregular neoplastic lesion in the liver measuring 150 x 137 x 26 mm. This lesion nearly entirely occupied the right hepatic lobe and showed increased peripheral vascular activity (Figure 1), a finding confirmed by magnetic resonance imaging. Serum biomarkers alpha-fetoprotein, CA 19-9, and carcinoembryonic antigen were within normal range (Table 1). The serum C-reactive protein (CRP) was 6.4 mg/dL (Table 2). There were also elevated values of amylase, lipase, alkaline phosphatase, and gamma-glutamyl transferase (Table 2).
A-B: Solid, heterogeneous, irregular, and giant neoplastic lesion (yellow line) measuring 150 x 137 x 26 mm, almost totally replacing the right hepatic lobe, with increased peripheral vascular activity.
MRI with T1 and T2 sequences reported a liver with a longitudinal axis of 19.9 cm. The right hepatic lobe had an oval, encapsulated, large lesion with dimensions of 13.7 x 14.6 x 19.4 cm and an estimated volume of 2020 cc. The borders of the tumor were well-defined, occupying segments V, VII, and VIII, with a heterogeneous pattern at the expense of cystic and necrotic areas (Figure 2). After IV Gadolinium administration, there was a heterogeneous avid enhancement with peripheral predominance in the arterial phase and moderate lavage in the venous and equilibrium phases (Figure 3). The lesion partially compressed the inferior vena cava, displaced the pancreas to the contralateral side, and pushed the right kidney caudally. It was not associated with free fluid or reactive lymph nodes.
A) In the magnetic susceptibility sequence, irregular hypointense areas with a central distribution suggestive of blood remains are identified. In the diffusion sequence, no restriction areas are identified. B) After the application of intravenous gadolinium, the lesion shows heterogeneous avid enhancement, predominantly peripheral in the arterial phase, with moderate washout in the venous and equilibrium phases.Hepatic tumor is indicated by yellow-dotted line.
Dynamic sequence with hepatospecific gadolinium: A) Pre-contrast 0''; B) Arterial phase 25-30''; C) Venous phase 40-45''; D) Balanced phase 20''; and E) Late phase 30''.Hepatic tumor is indicated by yellow dotted line.
The USG-guided liver biopsy reported a hepatic lesion compatible with hepatocellular adenoma of the inflammatory subtype (telangiectatic). The immunophenotype was glutamine synthetase positive and amyloid A positive, with a proliferation rate of <1% (Figure 4).
Liver appearance post-ultrasound-guided biopsy.No hematoma detected after biopsy.
A surgical intervention was performed via right anatomic hepatectomy using a chevron incision through the abdominal wall (Figure 5). An automatic abdominal retractor was placed for better exposure. The release of the right coronary and triangular ligaments was achieved with bipolar energy (Figure 6). Resection of the right hepatic lobe was completed with monopolar and bipolar energy, aided by intraoperative ultrasound (Figures 7-8). The Pringle maneuver was not necessary during the surgery. The surgery did not have any complications. The right hepatic lobe measured 20 x 16 x 11 cm and was indurated upon palpation, with a heterogeneous superficial pattern and a more vascularized zone (Figure 9). The abdominal drain was placed in the right subdiaphragmatic space. In the post-surgical period, the patient had an in-hospital stay of 3 days without any complications.
Chevron incision in the abdominal wall with adequate exposure of the liver and evidence of a tumor in the right hepatic lobule (indicated by yellow arrow).
Releasing the right coronary and triangular ligaments (yellow arrow) using bipolar energy, with the tumor being retracted (red arrow).
A-B: Separation of the right hepatic lobe using bipolar energy, facilitated by an impact and extraction clamp. Dissection of liver parenchyma with bipolar energy.
Posterior-to-right hepatectomy with adequate hemostasis of the remaining liver. Identifications include the portal vein (yellow arrow), middle suprahepatic vein (red arrow), colon (green arrow), duodenum (blue arrow), and diaphragm (purple arrow).
Macroscopic appearance of the resected specimen showing a non-encapsulated, well-defined, solitary tumor with central hemorrhage on the cut surface. Dimensions: 20 x 26 x 11 cm.
During the outpatient monitoring via laboratory tests and imaging at the first and third months, the patient did not exhibit any disease recurrence. A total of six months of follow-up was conducted with no post-surgical complications.
Pathology examination confirmed the diagnosis of hepatocellular adenoma, telangiectatic inflammatory subtype. The presence of areas exhibiting hemorrhage and necrosis without atypia, unusual mitosis, or invasion into parenchymal regions was noted (Figure 10).
A-B: The slides reveal a tumor displaying a clearly delineated border with the surrounding healthy liver tissue. It consists predominantly of hepatocytes exhibiting no notable cytologic abnormalities. Several areas exhibit hemorrhage and necrosis. There is no presence of cytologic atypia, unusual mitosis, or invasion into parenchymal regions. Ductular reaction is present.Several areas display hemorrhage and necrosis. There are no signs of cytologic atypia, unusual mitoses, or invasion into parenchymal regions. A ductular reaction is present.
Discussion
HCAs are infrequent, noncancerous tumors originating from hepatocytes, manifesting at a rate of approximately 3-4 occurrences per 100,000 individuals [7].
These tumors typically range in size from 8 to 15 centimeters, although reports of giant adenomas exceeding 20 cm are rare [8]. Their growth is closely linked to hormonal levels. Approximately half of hepatic adenomas exhibit regression or cessation of growth upon discontinuation of oral hormonal therapy [8]. The patient denied any history of oral hormonal medication usage.
The primary complications associated with HCAs include potential malignant progression, hemorrhage, and rupture, with their occurrence becoming more likely as the adenoma size increases [9-10]. When dealing with giant adenomas, the optimal treatment modality is surgical removal, performed at a liver surgery center with expertise in such procedures [8].
The classification of HCAs into subtypes relies on histopathological assessment, which considers the unique molecular features of each subtype. Accurate diagnosis is vital because clinical manifestations, such as the likelihood of malignancy, vary according to the subclassification [11].
IHCA is linked to conditions such as excessive alcohol consumption, metabolic syndrome, and obesity, along with heightened levels of inflammation-related proteins like serum amyloid A (SAA) and CRP [12-13]. Despite being overweight, our patient did not meet the criteria for obesity and denied any significant alcohol consumption during questioning.
The distinction between various liver tumors is crucial to clinical practice due to differences in medical management approaches. For instance, focal nodular hyperplasia (FNH) shares similarities with HCA, yet surgical intervention is typically unnecessary for FNH unless the patient experiences persistent pain that does not respond to treatment [11].
For diagnosing HCA through radiological means, multiphase dynamic contrast-enhanced MRI or multiphase CT are commonly employed, with the former being the preferred modality [14-15]. HCAs typically appear hypoattenuating on noncontrast CT scans, exhibit hypervascularity and heterogeneity during the arterial phase, and demonstrate iso/hypoattenuation during the portal venous phase of contrast-enhanced CT scans [15]. Arterial enhancement is a shared feature between HCAs and FNH, and differentiation between the two can be achieved using hepatocyte-specific contrast agents when standard imaging yields inconclusive results [16].
Laumonier H et al. and Ronot M et al. have highlighted MRI’s utility in distinguishing between the two main subtypes of HCA: HNF-1a-inactivated and inflammatory HCA, each displaying distinct features associated with intratumoral steatosis and sinusoidal dilatation, respectively [17-18].
The expected findings on multiphase dynamic contrast-enhanced MRI for inflammatory HCA are as follows in T1/T2-weighted images: presenting with isointensity or slight hyperintensity, and maintaining signal integrity on chemical shift sequences, with diffuse hyperintensity. Notable arterial enhancement continues into the portal venous and delayed phases [16].
In our case, the MRI showed, as previously mentioned, a heterogeneous avid enhancement of peripheral predominance in the arterial phase, with moderate washout in the venous and balance phases being compatible with the frequent findings in inflammatory HCA.
Hemorrhage occurs in 21% to 40% of HCAs, and in most cases, the bleeding is intratumoral. However, it can lead to tumor rupture, resulting in either intraperitoneal or subcapsular hemorrhage. The incidence of hemorrhage is higher in HCAs larger than 5 centimeters, with other contributing factors including the inflammatory subtype, tumor growth, recent hormone usage within the past six months, and pregnancy [19]. Emergency surgery for ruptured HCAs carries a mortality rate of 5% to 10% [20].
The probability of HCA transitioning into malignancy is approximately 5%, influenced by factors such as patient gender, tumor size, and subtype [21]. Mutations in the ß-catenin gene are correlated with an increased likelihood of malignant transformation, with up to 46% of ß-catenin-activated HCAs showing characteristics indicative of hepatocellular carcinoma (HCC) [22]. About 10% of inflammatory HCAs with mutated ß-catenin genes may undergo malignant conversion [23].
For male patients, surgical resection is advised irrespective of tumor size, while for female patients, resection is recommended for tumors measuring 5 cm or larger. However, for multiple tumors smaller than 5 centimeters, surgical resection is not deemed necessary, as most residual HCAs tend to remain stable or even regress spontaneously [21].
Transarterial embolization (TAE) is a recommended intervention for cases of HCA complicated by hemorrhage. Patients experiencing tumoral hemorrhage rarely exhibit hemodynamic instability, allowing for an initial TAE procedure before delayed surgery. TAE is indicated within 2 to 3 days following tumoral hemorrhage, preferably using a selective approach [21-24]. This procedure is minimally invasive, can be safely repeated, and has shown promising outcomes; approximately 80% of tumors may exhibit stability, regression, or complete involution. Importantly, these favorable results are primarily observed in cases involving small tumors. Additionally, TAE may be considered for managing large, multiple, or bilateral tumors, as well as for preoperative reduction in tumor size [24].
The patient presented with a large tumor measuring over 20 cm in diameter, which posed a higher risk of hepatic rupture rather than malignant change. The decision was made to proceed with surgical management, and TAE was not employed.
Conclusions
In conclusion, HCAs are tumors for which the size and subtype dictate the surgical management. Likewise, the treatment of choice for giant HCAs is surgery, which most of the time results in practically no recurrence after surgical resection. Also, the prompt diagnosis of this tumor can diminish the complications that the patient may experience in post-surgical recovery.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Synchronous giant hepatic adenoma in siblings-A case report and brief literature review Cancer Biol Ther Zhang C Shi X Zhao L 7277311720162709639210.1080/15384047.2016.1177682 PMC 4970524 · doi ↗ · pubmed ↗
- 2Hepatic adenomas: classification, controversies, and consensus Surg Pathol Clin Torbenson M 3513661120182975187910.1016/j.path.2018.02.007 · doi ↗ · pubmed ↗
- 3Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice Townsend CM Beauchamp RD Evers BM Mattox KL St. Louis, MO Elsevier Health Sciences 2022 https://books.google.com.mx/books/about/Sabiston_Textbook_of_Surgery_E_Book.html?id=nvz_m It Qy M 4C&redir_esc=y
- 4Focal benign liver lesions and their diagnostic pitfalls Radiol Clin North Am Reizine E MuléS Luciani A 7557736020223598904310.1016/j.rcl.2022.05.005 · doi ↗ · pubmed ↗
- 5Somatic mutations activating STAT 3 in human inflammatory hepatocellular adenomas J Exp Med Pilati C Amessou M Bihl MP 1359136620820112169025310.1084/jem.20110283 PMC 3135371 · doi ↗ · pubmed ↗
- 6Integrated analysis of somatic mutations and focal copy-number changes identifies key genes and pathways in hepatocellular carcinoma Nat Genet Guichard C Amaddeo G Imbeaud S 6946984420122256151710.1038/ng.2256 PMC 3819251 · doi ↗ · pubmed ↗
- 7Epidemiology of hepatocellular adenoma. The role of oral contraceptive use JAMA Rooks JB Ory HW Ishak KG Strauss LT Greenspan JR Hill AP Tyler CW Jr 6446482421979221698 · pubmed ↗
- 8Liver cell adenomas. A 12-year surgical experience from a specialist hepato-biliary unit Annals Surg Leese T Farges O Bismuth H 5585642081988 http://dx.doi.org/10.1097/00000658198811000-0000310.1097/00000658-198811000-00003 PMC 14937953190282 · doi ↗ · pubmed ↗