Dual-Arch Prosthesis: Revolutionizing Partial Dentate Rehabilitation
Ekta M Kanojia, Anjali Bhoyar, Surekha A Dubey, Sheetal R Khubchandani, Mahima S Agrawal, Rucha Chiddarwar

TL;DR
A new dental treatment using overdentures and partial dentures improves patient outcomes by restoring function and aesthetics.
Contribution
The paper presents a successful case of dual-arch prosthetic rehabilitation for partially dentate patients.
Findings
Combining maxillary overdentures and mandibular CPDs restored masticatory function and aesthetics.
The treatment modality enhanced patient quality of life and provided cross-arch stabilization.
The approach mitigated residual ridge resorption and improved oral hygiene maintenance.
Abstract
The utilization of natural teeth as denture abutments offers a significant advantage in retarding the residual ridge resorption (RRR). This approach distributes stress concentration between the denture-bearing areas and abutment teeth, thereby mitigating issues such as loss of sensory feedback, compromised mastication, and aesthetic concerns. Overdentures, by providing additional support and stability, play a pivotal role in reducing RRR while enhancing stability and retention. A cast partial denture (CPD) becomes the first choice in cases of long edentulous span where cross-arch stabilization is required. The simplicity of insertion, removal, and maintenance, coupled with effective oral hygiene practices, make CPDs a practical solution. This case presentation illustrates the successful prosthetic rehabilitation of a partially dentate patient through the implementation of a maxillary…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
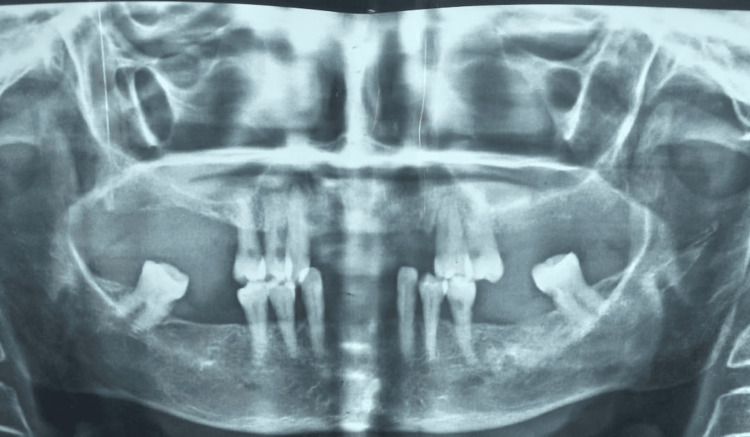 Figure 1
Figure 1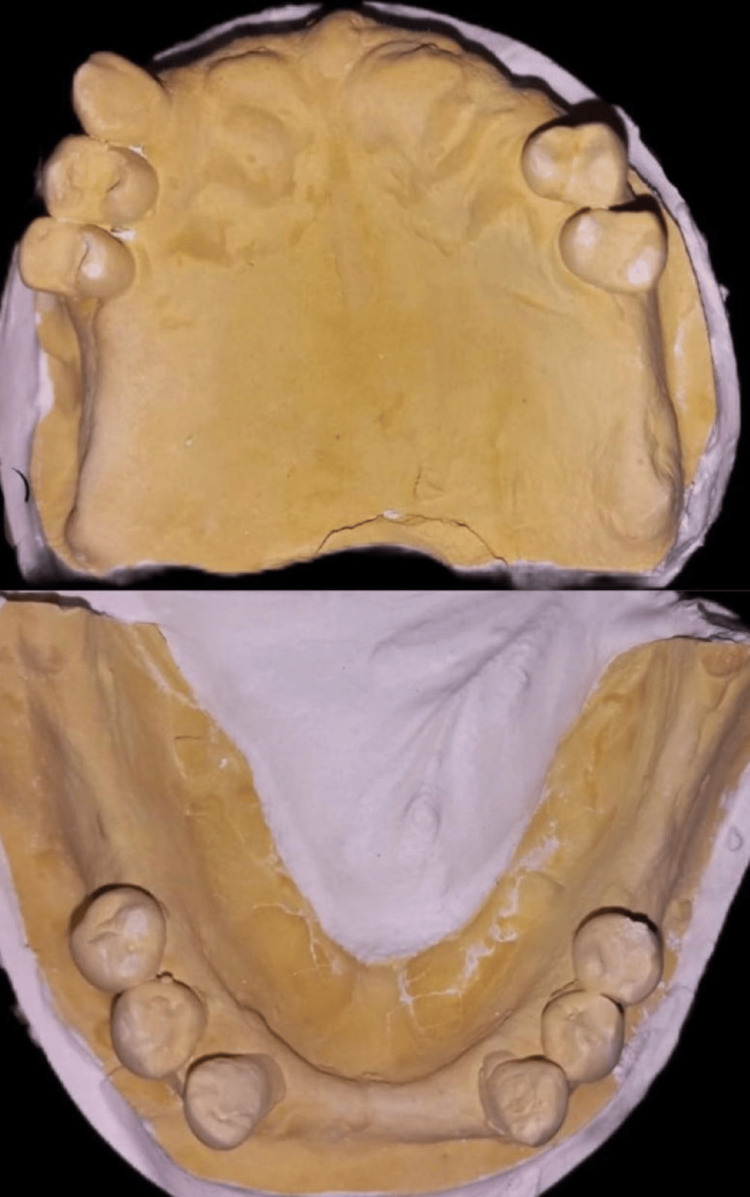 Figure 2
Figure 2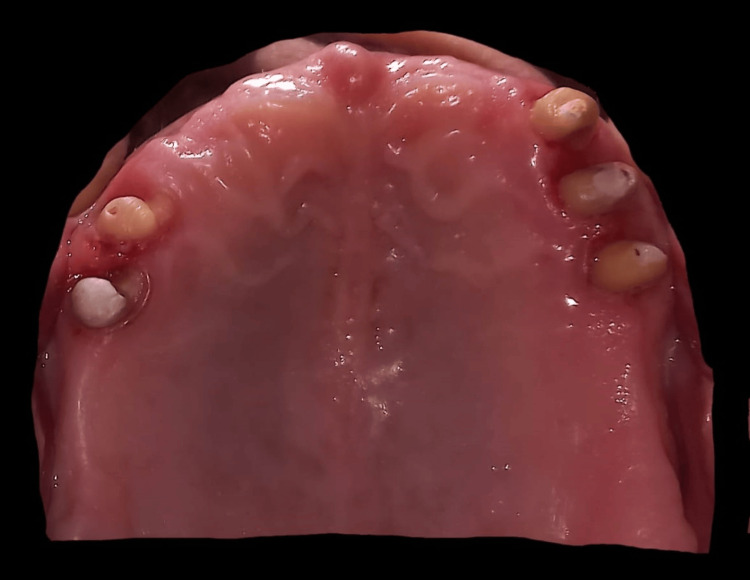 Figure 3
Figure 3 Figure 4
Figure 4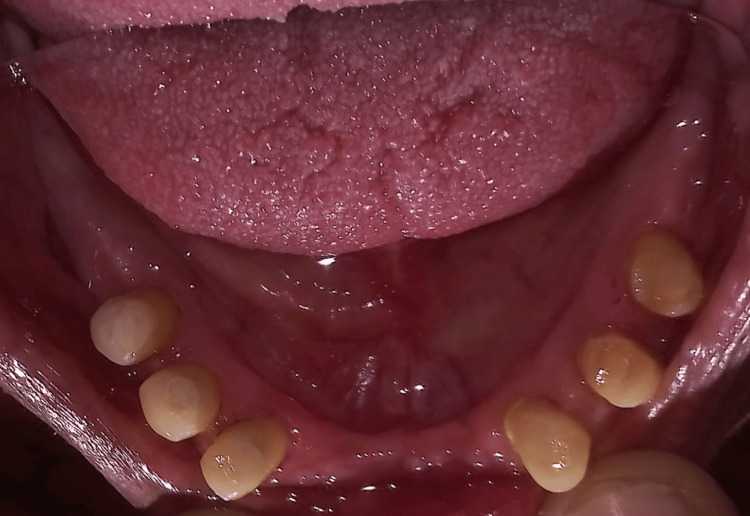 Figure 5
Figure 5 Figure 6
Figure 6 Figure 7
Figure 7 Figure 8
Figure 8 Figure 9
Figure 9 Figure 10
Figure 10 Figure 11
Figure 11 Figure 12
Figure 12Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDental Implant Techniques and Outcomes · Dental Health and Care Utilization · Oral microbiology and periodontitis research
Introduction
A condition called edentulousness is characterized by the loss of a tooth, leading to adverse biomechanical and aesthetic consequences. While there has been a decline in the prevalence of complete denture (CD) wearers, the number of partially edentulous patients has risen, likely influenced by global aging trends and oral health-focused preventive measures. Prosthetic solutions provide a range of choices for restoring missing tooth in partially edentulous individuals, encompassing removable partial dentures (RPDs), which can be supported by natural teeth or dental implants [1].
Achieving aesthetically and functionally successful prosthetic rehabilitation necessitates meticulous treatment planning and attention to detail. The Kennedy classification is a system used in dentistry to categorize partially edentulous arches based on the location and extent of missing teeth, aiding in the design of RPDs. It includes four main classes: class I (bilateral edentulous areas posterior to the remaining natural teeth), class II (a unilateral edentulous area posterior to the remaining natural teeth), class III (a unilateral edentulous area with natural teeth remaining both anterior and posterior to it), and class IV (a single, bilateral edentulous area located anterior to the remaining natural teeth). This classification helps in planning and communication among dental professionals [2]. Rehabilitation of partially edentulous arches presents challenges, particularly in distal extension situations classified under Kennedy's class I and class II categories [3]. In such cases, the fabrication of a fixed partial denture (FPD) is not viable due to the absence of distal abutments. While implant-supported prostheses may be considered, limitations such as inadequate bone volume and economic constraints may render them impractical. Therefore, in such scenarios, acrylic partial dentures or cast partial dentures (CPDs) are often preferred alternatives for achieving satisfactory outcomes [4].
The number and position of missing teeth significantly influence the effectiveness of prosthetic restorations in replicating natural dentition and maintaining oral functions. CPDs have demonstrated superior outcomes when compared to removable acrylic partial dentures, for example, the retention and stability of the denture, comfort of the patient, chewing efficiency, and periodontal condition of abutment teeth [5]. Conversely, conventional CD therapy may lead to suboptimal retention, stability, and patient satisfaction, thereby compromising confidence and comfort. While RPDs like CPDs are gradually becoming less favored as fixed prosthesis options become more accessible, the treatment of choice, particularly for medically compromised patients, is CPD over FPD as illustrated in the present case [6].
Overdentures offer a promising solution to address the shortcomings associated with conventional CD. They effectively mitigate issues such as denture loosening, diminished proprioception, and residual ridge resorption, thereby serving as a preventive measure against complete edentulism [7]. Overdentures prioritize the preservation of natural teeth, aligning with patient preferences and helping to maintain oral function and aesthetics. Despite advancements in dental implants, the conservative approach of preserving roots followed by overdenture placement remains relevant. The selection of treatment modalities is influenced by factors such as the condition of surrounding teeth and tissues, patient preferences, and financial considerations [8]. This case report highlights the successful rehabilitation of a partially dentate patient utilizing a maxillary overdenture and mandibular CPD, emphasizing the effectiveness of this treatment approach in attaining favorable outcomes.
Case presentation
A female patient aged 72 years old presented to the Department of Prosthodontics and Crown and Bridge with a major complaint of edentulism and masticatory dysfunction. She reported undergoing dental extractions for six months. The areas were maxillary (left and right) posterior-most regions. The patient's reluctance to pursue invasive interventions necessitated the formulation of a conservative treatment approach. Given her edentulous state and functional impairment, the treatment plan focused on prosthetic rehabilitation to restore oral function and aesthetics. This involved the fabrication of RPDs for the missing posterior teeth, aiming to optimize masticatory efficiency and improve the patient's overall quality of life.
Clinical examination revealed that the patient has multiple missing teeth in different locations of the oral cavity. In the maxillary arch, the first, second, and third molars were absent bilaterally, along with teeth 11, 12, 21, 22, and 23. Similarly, in the mandibular arch, teeth 31, 32, 36, 37, 41, 42, 46, and 47 were missing. Additionally, tooth 38 exhibited root caries and severe mobility, while tooth 48 remained present. The patient demonstrated adequate oral hygiene. Clinical examination findings were consistent with those from the radiographic examination, particularly evident in the orthopantomography, which indicated a poor prognosis for teeth 38 and 48. Consequently, extractions were planned (Figure 1).
Orthopantomograph image.
Mouth preparation was done. Impressions were made in irreversible hydrocolloid material. Subsequently, dental stone diagnostic models were made (Figure 2).
Maxillary and mandibular diagnostic cast.
The existing occlusion of the patient was recorded using bite registration. The stone models were mounted on an articulator (mean value). The models were meticulously examined for diagnostic purposes, allowing for a comprehensive assessment of the patient's dental condition and aiding in the formulation of an appropriate treatment plan. Rehabilitation was done with a tooth-supported overdenture for the maxillary arch. The mandibular arch was rehabilitated with a CPD - Kennedy Class I Mod 1. Endodontic (root canal) therapy was deemed necessary for all maxillary and mandibular teeth due to proximal caries, periapical infection, and chronic pain experienced by the patient. In the maxillary arch, teeth were prepared in a dome-shaped manner with an approximate height of 3-4 mm, using tapered, round-end diamond points. Chamfer finish lines were incorporated subgingivally (Figure 3) to ensure optimal fit and restoration longevity.
Tooth preparation done for the metal coping for tooth-supported maxillary overdenture.
Following gingival retraction in the maxillary arch, a final impression was obtained using additional silicone material employing the two-step impression technique. This impression served as the basis for creating the master model, which in turn facilitated the fabrication of copings for subsequent restorative procedures (Figure 4).
Metal coping cemented on the maxillary cast for overdenture.
In the mandibular arch, all teeth were prepared for porcelain-fused-to-metal (PFM) crowns, with teeth 33, 34, 35, 43, 44, and 45 designated for restoration (Figure 5).
Tooth preparation done for the PFM crown with teeth 33, 34, 35, 43, 44, and 45.PFM: porcelain-fused-to-metal
Rest seats were incorporated onto the wax pattern of teeth 33, 35, 43, and 45, with guiding planes prepared accordingly. Subsequently, the crowns were cemented in place. Following crown cementation, the final impression was made (Figure 6).
Final impression made for the master cast.
The resulting secondary cast was surveyed to examine and design the cast partial framework. Digital scans were used to finalize the design of the CPD (Figure 7).
Using exocad digital software for designing of the mandibular CPD.CPD: cast partial denture
Addition silicone materials of two consistencies, namely, heavy and light, were used for making the final impression. Then, a master cast was poured. Duplication of the cast was done using a reversible hydrocolloid to obtain a refractory cast made up of investment material. The design of the CPD was formulated, and it was transferred to the refractory cast after which a wax pattern was fabricated. This wax framework was subjected to casting, and Co-Cr alloy was employed. The metal framework after casting was finished and polished (Figure 8 and Figure 9). Framework was then assessed intraorally.
Try-in of the metal framework on the cast.
Try-in of metal framework intraorally.
Jaw relation was recorded using occlusal rims. Mounting of the recorded relation was done using an articulator (semi-adjustable). Try-in was done to ensure proper fit and function (Figure 10).
Try-in procedure image.
Finally, Figure 11 displays the prostheses intraorally, showcasing the completed dental restoration.
Final denture insertion procedure.
Figure 12 shows the preoperative and postoperative images of the patient.
Preoperative and postoperative photograph.
Discussion
For this patient, a maxillary overdenture and a mandibular CPD were selected as treatment modalities owing to their superior stability and retention properties, facilitating optimal distribution of stress and proprioceptive feedback through extant natural dentition. Conversely, alternative therapeutic approaches encompassed the removal of teeth which are present and then a conventional complete set of denture placement [9]. However, such an approach was eschewed due to its potential to diminish proprioceptive input and compromise the structural support conferred by the remaining natural dentition and associated periodontal ligaments. The full-mouth implant-supported prosthesis was precluded as a treatment avenue, given the patient's medical comorbidities and aversion to surgical interventions [10].
Nevertheless, tooth-supported overdentures present certain drawbacks, including the imperative for meticulous oral hygiene to avert periodontal and caries afflictions. These overdentures typically possess larger, more contoured structures, potentially encroaching upon inter-occlusal space [11]. Furthermore, RPDs exhibit limitations, such as patient adaptation challenges and the requisite adjustment period, plaque accumulation on abutment teeth, predisposition to periodontal pathology, and carious lesions. Additionally, inadequately designed RPDs may manifest aesthetic concerns due to visible metal components. The prospect of complete tooth loss is profoundly distressing for patients, precipitating a decline in morale by underscoring dependence and aging [11]. In such instances, the consistent integration of overdentures as a preventive prosthodontic intervention is advocated within dental practices due to their multifarious advantages.
A study has been conducted by Rissin et al. comparing masticatory performance among individuals with natural dentition, CD, and overdentures. Their findings revealed that masticatory efficiency was superior in patients wearing overdentures compared to those with CD [12]. Additionally, Crum and Rooney conducted a five-year study where cephalometric radiographs illustrated vertical bone loss (0.6 mm average) in the region of the anterior mandible of overdenture wearers, contrasting with a 5.2 mm loss observed in CD wearers [13]. Another study found that the existence of RPDs had a substantial impact on nutritional consumption, implying that restoring edentulism might encourage patients towards a healthy plan of diet [14]. Partial tooth loss has been shown to have a negative influence on food acceptance, similar to how edentulism impacts diet quality and nutritional status. Consequently, removable treatment modalities are favored for patients unable to undergo fixed prosthetic procedures despite limitations [15].
Moreover, retaining natural teeth preserves proprioception in overdenture wearers, contributing to enhanced satisfaction and patient acceptability. Thus, this case presentation serves to validate the partially dentate successful rehabilitation through the utilization of a maxillary overdenture and mandibular CPD.
Conclusions
This case presentation demonstrates the successful prosthetic rehabilitation of a partially dentate patient through the implementation of a maxillary overdenture and mandibular CPD. By utilizing these treatment modalities, optimal outcomes in terms of function, aesthetics, and patient satisfaction were achieved. The use of a maxillary overdenture helped preserve natural teeth and mitigate issues associated with complete edentulism, while the mandibular CPD provided stability, retention, and improved masticatory function. Overall, this case underscores the efficacy of combining these prosthetic options in addressing the complex needs of partially dentate individuals, ultimately enhancing their quality of life and oral health.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mc Cracken's Removable Partial Prosthodontics Mc Craken's Removable Partial Prosthodontics. 12th Edition. Mosby Carr AB Brown DT 16232 St. Louis, MO Elsevier Mosby 2011 https://search.worldcat.org/title/698080406
- 2A viable treatment alternative in distal extension cases: a case report J Indian Prosthodont Soc Kukunoor S Savadi RC Venkata Krishnam Raju K Kumar S 1771801420142619951110.1007/s 13191-012-0218-6PMC 4501998 · doi ↗ · pubmed ↗
- 3Genetic mapping in papillon-lefèvre syndrome: a report of two cases Case Rep Dent Thakare KS Bhongade ML Charde P Kale S Jaiswal P Somnath BK Pendor S 404120201320132430321910.1155/2013/404120 PMC 3834890 · doi ↗ · pubmed ↗
- 4Removable partial dentures: the altered-cast technique J Dent Technol Garcia EE Evans JG 2529151998 https://pubmed.ncbi.nlm.nih.gov/10337279/10337279 · pubmed ↗
- 5Prosthetic rehabilitation of a partially dentate patient with a maxillary cast partial denture and mandibular overdenture: a case report Cureus Bansod AV Pisulkar SG Sathe S Beri A Dahihandekar C 014202210.7759/cureus.28652 PMC 952524636196325 · doi ↗ · pubmed ↗
- 6Stability in complete dentures: an overview IOSR J Dent Med Sci Mistry R Pisulkar SK Borle AB Godbole S Mandhane R 3641172018 https://www.researchgate.net/profile/Rohit-Mistry-3/publication/340248153_Stability_in_Complete_Dentures_An_Overview/links/5e 7eed 00458515 efa 0b 11423/Stability-in-Complete-Dentures-An-Overview.pdf
- 7Prosthodontic considerations of speech in complete denture IOSR J Dent Med Sci Godbole S Phakhan AJ Kale S Dahane T 4144152016 https://www.researchgate.net/profile/Sweta-Pisulkar/publication/342410125_Prosthodontic_Considerations_of_Speech_in_Complete_Denture/links/5ef 2eae 692851 cba 7a 46183 a/Prosthodontic-Considerations-of-Speech-in-Complete-Denture.pdf
- 8Host response to two different designs of minor connector J Oral Rehabil Runov J Kroone H Stoltze K Maeda T El Ghamrawy E Brill N 14715371980698735010.1111/j.1365-2842.1980.tb 00431.x · doi ↗ · pubmed ↗