Justification: gain or game
Mannudeep K. Kalra, Mônica Oliveira Bernardo, Lina Karout, Alair Augusto Sarmet Moreira Damas dos Santos

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
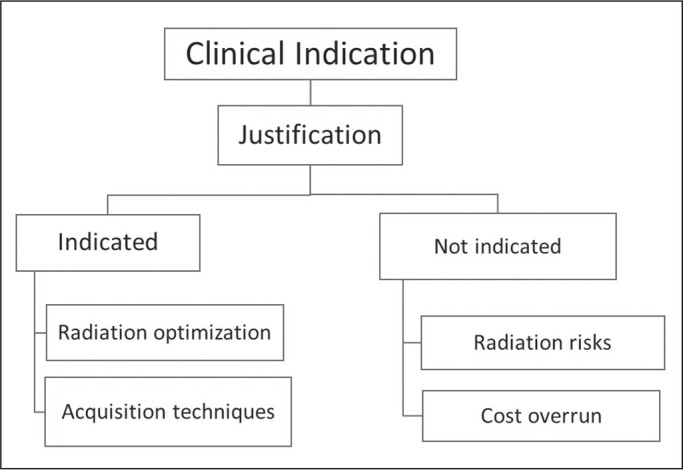 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMedical Malpractice and Liability Issues
INTRODUCTION
Innovations and access to medical imaging have increased its utilization. While some regard imaging as the modern stethoscope to peer within the opaque anatomy and complex physiology, others caution over radiation risks, the workup required when there are incidental findings, and the healthcare costs related to over-testing. Although the justified use of imaging provides invaluable information on the presence and extent of abnormalities, the statistics on unjustified procedures should not be ignored.
Digitalizing justification
Stemming from concerns over spiraling costs, referral guidelines and appropriateness criteria to promote the justification of imaging tests have been proposed by various organizations^(1-3)^. With evidence-based findings and consensus statements by multidisciplinary committees of expert physicians, these guidelines recommend specific imaging pathways or review the risks, benefits, and individual utility of imaging tests for several dozen common clinical indications (Figure 1). The American College of Radiology Appropriateness Criteria, incorporated within the electronic health records (EHRs), help physicians determine the appropriateness of imaging tests based on certain symptoms, signs, and diagnoses^(1)^. The EuroSafe Referral Guidelines for Imaging provide online clinical decision support (CDS) systems for several clinical indications and imaging modalities^(2)^. Those CDS systems provide the utility of different imaging examinations and symbols for the relative radiation levels (a single radiation icon for low-dose radiography versus multiple icons for higher-dose computed tomography). Some provide the relative costs of imaging tests with USD/Euro symbols.
Figure 1. Justification helps determine whether or not an ordered imaging test is truly indicated. Non-indicated tests entail unnecessary radiation risks and cost overruns. The indications that help determine justification can also help optimize acquisition techniques and radiation doses.
At Mass General Brigham, the EHR-embedded CDS system lets the referring physician select a convenient site (hospital versus offsite locations), day, and time for an imaging test^(3)^. In addition to the convenience, the electronic CDS system allows referral practices to be audited and monitored over time.
Limitations
Like legal justice, which is an absolute necessity but not always fair or timely, justification has its limitations. Prior studies have documented a decline in the utilization of imaging tests after the implementation of a CDS system^(4-7)^. Weilburg et al. reported a 28% decline in the use of high-cost imaging tests from 2007 to 2013, after a utilization management program was instituted in an outpatient setting^(6)^. However, some studies have suggested that those initial reductions in imaging utilization are temporary^(8,9)^. Other investigations have raised concerns about the substantial lack of consistency between the clinical indications specified in the CDS system and the symptoms, signs, and diagnoses described in the EHRs^(10)^. Gupta et al. found a 4.2% error rate in CDS system orders for computed tomography pulmonary angiography^(10)^. Such inconsistencies do not necessarily suggest malicious intent and might stem from errors in the EHR, a complex clinical presentation, or patient expectations or demands. The Brazilian College of Radiology and Diagnostic Imaging has initiated efforts to create referral guidelines for imaging in Brazil.
Future
The disconcerting frequency of incorrect and incomplete clinical information in CDS systems offers an opportunity to aid or automate the determination of the best imaging tests based on the text recorded in the EHR^(11,12)^. Gish et al. reported that the proportion of referring physicians who preferred the imaging tests suggested by a new free-text-based artificial intelligence (AI) tool was significantly greater than that of those who preferred the traditional order-entry CDS system (58.9% vs. 41.1%; p < 0.01)^(11)^. In addition, the free-text-based AI tool predicted orders correctly in 91.7% of cases. Another study, conducted by Ramgopal et al., demonstrated that an AI tool can accurately predict the need for clinical and imaging tests in children presenting to the emergency department, with an area under the receiver operating characteristic curve of 0.89-0.99^(13)^. Given the excitement over Chat GPT, could the use of large language models further improve compliance or automated selection of imaging pathways? Only time and further studies will tell us if such a path leads to justice in justification.
CONCLUSION
Implementing and monitoring justification in imaging are complex tasks. There are definite gains to be made from the justified use of imaging tests, including reductions in the associated risks and costs. However, the gamut of clinical presentations, physician practices, and patient preferences makes this a complicated game in search of a satisfactory solution.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Frush DP. Justification and optimization of CT in children: how are we performing?Pediatr Radiol 201141 Suppl 24674712184772410.1007/s 00247-011-2097-0 · doi ↗ · pubmed ↗
- 2Expert Panel on Thoracic Imaging Bang TJ Chung JH Walker CM ACR Appropriateness Criteria® routine chest imaging J Am Coll Radiol 202320 S 224S 2333723674510.1016/j.jacr.2023.02.006 · doi ↗ · pubmed ↗
- 3EUROSAFE Referral guidelinescited 2023 Oct 15Available from: https://www.eurosafeimaging.org/referral-guidelines
- 4Rosenthal DI Weilburg JB Schultz T Radiology order entry with decision support: initial clinical experience J Am Coll Radiol 200637998061741217110.1016/j.jacr.2006.05.006 · doi ↗ · pubmed ↗
- 5Gupta S Klein K Singh AH Analysis of low appropriateness score exam trends in decision support-based radiology order entry system J Am Coll Radiol 2017146156212819070210.1016/j.jacr.2016.12.011 · doi ↗ · pubmed ↗
- 6Weilburg JB Sistrom CL Rosenthal DI Utilization management of high-cost imaging in an outpatient setting in a large stable patient and provider cohort over 7 years Radiology 20172847667762843055710.1148/radiol.2017160968 · doi ↗ · pubmed ↗
- 7Yan Z Ip IK Raja AS Yield of CT pulmonary angiography in the emergency department when providers override evidence-based clinical decision support Radiology 20172827177252768992210.1148/radiol.2016151985 PMC 5330300 · doi ↗ · pubmed ↗
- 8Foley SJ Bly R Brady AP Justification of CT practices across Europe: results of a survey of national competent authorities and radiology societies Insights Imaging 2022131773641701710.1186/s 13244-022-01325-1PMC 9684387 · doi ↗ · pubmed ↗