Myocardial Bridging-Induced Acute Coronary Syndrome: A Bridge Too Far
Priya Ramcharan, Arun R Katwaroo, Reyaz Hosein, Nicole Maharaj, Steven M Swarath, Valmiki Seecheran, Rajeev V Seecheran, Naveen A Seecheran

TL;DR
A 37-year-old man with no risk factors for heart disease had a heart attack linked to a heart condition called myocardial bridging.
Contribution
Highlights myocardial bridging as a potential cause of acute coronary syndrome in young patients without traditional risk factors.
Findings
A young patient with myocardial bridging experienced a heart attack without typical risk factors.
Successful treatment involved medical therapy and intervention without affecting the bridged segment.
Myocardial bridging may contribute to major adverse cardiovascular events.
Abstract
Recent studies suggest a potential association between myocardial bridging (MB) and accelerated atherosclerotic plaque formation. We describe the case report of a 37-year-old South Asian male with no established risk factors for coronary artery disease (CAD) who presented with a non-ST-segment-elevation acute coronary syndrome (NSTE-ACS) with a coincident widowmaker lesion and severe MB. He was successfully managed with comprehensive guideline-directed medical therapy (GDMT) and urgent percutaneous coronary intervention (PCI) of the culprit lesion, sparing the MB segment. The clinician should be cognizant of MB implicating ACS as a major adverse cardiovascular event (MACE) and its key management strategies.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
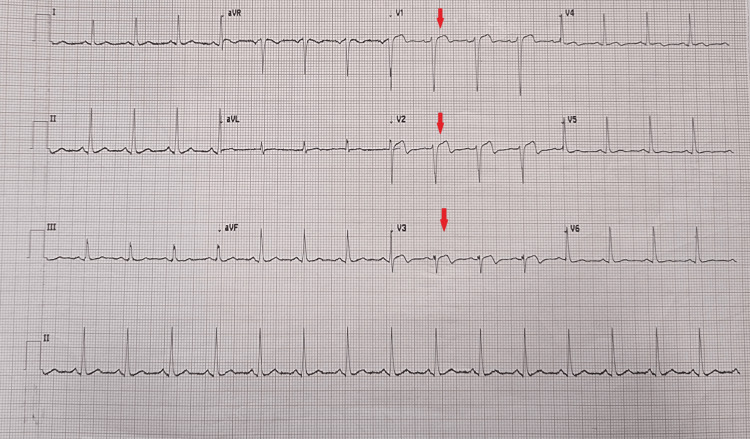 Figure 1
Figure 1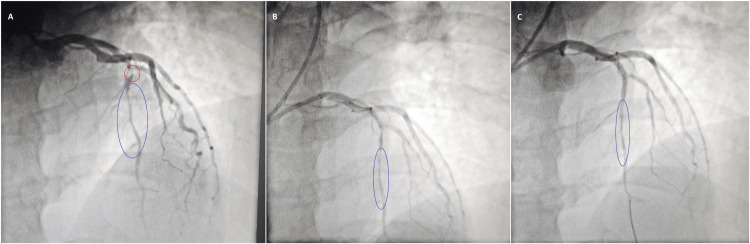 Figure 2
Figure 2| Diagnostic data | |||
| Complete Blood Count | Patient value | Units | Normal range |
| White blood cells (WBC) | 6.4 | 103µL | 4.0 – 10.3 |
| Red blood cells (RBC) | 4.72 | 106µL | 4.38 – 5.77 |
| Hemoglobin (Hb) | 16.1 | g/dL | 13.6 – 17.2 |
| Hematocrit (HCT) | 48.30 | % | 39.5 – 50.30 |
| Mean corpuscular volume (MCV) | 86.1 | fL | 80.70 – 95.50 |
| Mean corpuscular hemoglobin (MCH) | 31.7 | pg | 27.2 – 33.50 |
| Mean corpuscular hemoglobin concentration (MCHC) | 32.9 | g/dL | 32.7 – 35.6 |
| Red cell distribution width (RCW) | 12.8 | % | 11.8 – 14.3 |
| Platelet (PLT) | 310 | 103µL | 159 – 388 |
| Mean platelet volume (MPV) | 9.2 | fL | 6.90 – 10.8 |
| Comprehensive metabolic panel | Patient value | Units | Normal range |
| Sodium (Na) | 140.0 | mmol/L | 135 – 145 |
| Potassium (K) | 4.4 | mmol/L | 3.5 – 5.1 |
| Creatinine (Cr) | 0.8 | mg/dL | 0.7 – 1.2 |
| Urea (BUN) | 193.0 | mg/dL | 6.0 – 23.0 |
| Calcium (Ca) | 9.1 | mg/dL | 8.6 – 10.2 |
| Aspartate transferase (AST) | 32 | IU/L | 5.0 – 40.0 |
| Alanine transaminase (ALT) | 28 | IU/L | 5.0 – 41.0 |
| Alkaline Phosphatase (ALP) | 110 | U/L | 40 – 129 |
| Gamma-glutamyl transferase (GGT) | 34 | U/L | 6.0 – 61.0 |
| Total bilirubin (TBili) | 0.48 | mg/dL | 0.0 – 1.29 |
| Direct bilirubin (DBili) | 0.25 | mg/dL | 0.0 – 0.4 |
| Indirect bilirubin (IBili) | 0.23 | mg/dL | 0.0 – 1.0 |
| Total protein (TP) | 8.1 | g/dL | 6.4 – 8.3 |
| Albumin (ALB) | 4.8 | g/dL | 3.5 – 5.2 |
| Globulin (GLB) | 33.4 | g/dL | 2.3 – 4.5 |
| Magnesium (Mg) | 1.8 | mg/dL | 1.6 – 2.4 |
| Phosphorus (Phos) | 3.5 | mg/dL | 2.5 – 4.5 |
| Cardiac Pack | Patient value | Units | Normal range |
| C-reactive protein (CRP) | 20.10 | mg/dL | 0.100 – 0.500 |
| High-sensitivity cardiac Troponin I (hs-cTnI) 1 | 8.8 | ng/dL | 0.0 – 0.8 |
| High-sensitivity cardiac Troponin I (hs-cTnI) 2 | 3.7 | ng/dL | 0.0 – 0.8 |
| D-dimer | 0.26 | ng/mL | < 0.5 |
| B-type natriuretic peptide (BNP) | 112 | pg/mL | < 100 |
| Total cholesterol | 174 | mg/dL | < 200 |
| Low-density lipoprotein (LDL) | 136 | mg/dL | 60 - 130 |
| High-density lipoprotein (HDL) | 38 | mg/dL | > 40 |
| Triglycerides (TG) | 108 | mg/dL | < 150 |
| Glycosylated hemoglobin (HbA1c) | 5.4 | % | < 6.5% |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCoronary Artery Anomalies · Cardiac Arrhythmias and Treatments · Cardiovascular Issues in Pregnancy
Introduction
Myocardial bridging (MB) is a congenital anomaly characterized by the segmental intramyocardial course of an epicardial coronary artery. This anomaly entails tunneling the affected artery segment beneath a muscular bridge formed by the overlying myocardium [1,2]. MB has been implicated in various clinical presentations, including exertional angina, acute coronary syndromes (ACS), lethal arrhythmias such as ventricular fibrillation (VF), stress-related cardiomyopathy (SRC), and even sudden cardiac death (SCD). However, these complications are infrequent, with the majority of MBs being asymptomatic and posing minimal clinical significance. Notably, previously asymptomatic individuals might develop symptoms due to the emergence of coexisting conditions, such as left ventricular hypertrophy (LVH), diastolic dysfunction, coronary vasospasm, or microvascular dysfunction. Furthermore, exercise and tachycardia can potentially exacerbate symptoms and trigger major adverse cardiovascular events (MACEs) [2].
Recent studies suggest a potential association between MB and accelerated atherosclerotic plaque formation. This phenomenon appears proximal to the bridged segment, with the tunneled portion seemingly spared from plaque accumulation. Endothelial injury within the proximal segment is postulated as a contributing factor, potentially triggered by increased local wall tension and stretch during the cardiac cycle [3]. This case report describes the potential association between MB and a widowmaker lesion (proximal left anterior descending artery (LAD) occlusion) precipitating a non-ST-segment-elevation ACS (NSTE-ACS) in a young South Asian male without any conventional cardiovascular risk factors.
Case presentation
A 37-year-old Caribbean South Asian male with no significant medical history presented to the emergency department with an episode of typical angina, described as dull, substernal, and of 30 minutes duration. His family history revealed a first-degree relative (father, age 62) with coronary artery disease (CAD) status post percutaneous coronary intervention (PCI) for unstable angina. He is a lifelong non-tobacco user; however, he acknowledged occasional social alcohol consumption. He did not report any dyspnea, palpitations, presyncope, or syncope. He did not have any antecedent infection, nor did he have any pets or have traveled recently.
Upon initial evaluation, the patient presented with vital signs, including blood pressure of 133/88 millimeters of mercury (mmHg), heart rate of 93 beats per minute (bpm), respiratory rate of 18 breaths per minute, oxygen saturation of 98% on 2 liters nasal cannula, and body temperature of 36.0 degrees Celsius (°C). Physical examination revealed no acute distress, with normal cardiopulmonary auscultation (regular heart sounds without murmurs and clear breath sounds bilateral). Furthermore, the neurologic and abdominal examinations were normal. The 12-lead electrocardiogram (ECG) demonstrated a sinus rhythm with 2 millimeters (mm) ST-segment-elevation in V1-V3, suggestive of an evolving non-ST-segment-elevation acute coronary syndrome (NSTE-ACS) (Figure 1). A high-sensitivity cardiac troponin I (hs-cTnI) returned as 8.8 ng/dL (normal 0.0-0.8 ng/dL) (Table 1). The patient proceeded directly to the cardiac catheterization laboratory for urgent PCI. During coronary angiography (CAG), there was a “widowmaker” lesion (proximal LAD occlusion) with severe mid-LAD intra-MB, near-complete systolic compression, and a “milking” phenomenon [4]. The culprit lesion was successfully treated with provisional stenting, comprising pre-dilation with a drug-coated balloon (DCB) and subsequently stented with a zotarolimus drug-eluting (ZES) stent, with care to exclude the bridging segment with a good angiographic result and no complications (Figures 2a-2c). No intravascular ultrasonography (IVUS), fractional flow reserve (FFR), or optical coherence tomography (OCT) was performed, as these were not currently available in our setting.
The patient’s 12-lead electrocardiogram. The downward red arrows illustrate the 2-millimeter ST-segment-elevation in leads V1-V3, suggestive of an evolving non-ST-segment-elevation acute coronary syndrome (NSTE-ACS) for which the cardiac catheterization laboratory was activated for urgent percutaneous coronary intervention (PCI).
The patient’s coronary angiogram (CAG) and urgent percutaneous coronary intervention (PCI). (a) Left anterior oblique (LAO) imaging demonstrated the widowmaker lesion (encircled in red) and the severe mid-left anterior descending (LAD) artery myocardial bridging (MB) segment (ellipsed in blue). (b) LAO imaging demonstrated the pre-dilation of the culprit widowmaker lesion with a drug-coated balloon (DCB), with an improved but residual 50% stenosis and unchanged MB segment. (c) LAO imaging demonstration successful drug-eluting stent implantation at target lesion, sparing the MB segment.
The patient was hospitalized post-PCI for 48 hours. He received comprehensive, guideline-directed medical therapy (GDMT), which comprised aspirin, ticagrelor, ramipril, carvedilol, eplerenone, empagliflozin, rosuvastatin, amlodipine, and colchicine in accordance with American College of Cardiology and American Heart Association standard-of-care practice. A chest radiograph (CXR) reported no cardiomegaly or pulmonary edema. A two-dimensional transthoracic echocardiogram (2D-TTE) demonstrated mild anterior hypokinesis with an estimated left ventricular ejection fraction (LVEF) of 45%-50%. The remainder of his ensuing hospitalization was uneventful as he remained angina-free and hemodynamically stable with down-trending cardiac biomarkers. He was discharged with a follow-up appointment at the cardiology clinic in one week.
Discussion
MB is a medical condition first observed by Reyman in 1737 during an autopsy and was later described in 1960 through angiography [5-7]. This condition occurs when a part of the coronary artery runs through the myocardium instead of epicardially, creating a tunnel-like pathway [7,8]. Studies have shown that MB may be highly underdiagnosed, with postmortem examination reports indicating an incidence rate ranging from 15% to 85%, with a mean of 25% [5,7]. Cardiac computer tomography angiography (CCTA) follows closely at 22%, while invasive CAG displays a rate of 1.5%-16% (without provocation), with the majority being discovered incidentally [5,9]. Male patients are affected in 70% of cases [10]. The disparity in diagnostic studies can be attributed to including non-functional myocardial loops in pathological studies, advanced imaging, and hemodynamic modalities such as IVUS, FFR, OCT, and the lack of provocative testing [6,7,10]. MB was historically considered a benign anomaly due to the predominance of diastolic coronary perfusion. Although it is commonly believed to be low-risk, MBs can have severe clinical consequences such as angina, lethal arrhythmias, heart failure (HF), and SCD [6,7]. Accurate diagnosis and management of patients displaying symptomatology are integral to identifying potential risks and mitigating MACE.
However, recent evidence suggests a more complex relationship between anatomical factors and their pathophysiology. A broad spectrum of clinical presentations is contingent on the tunneled segment’s location, length, and depth, which underpin the potential for ischemia and guiding treatment decisions [11]. The LAD is the most common site in 67%-98% of detected myocardial bridges and most at the mid-LAD segment [10,11]. The length varies from 4 to 40mm, and depth ranges from 10 to 30mm [6,7,9,12,13]. Treatment strategies, especially surgical interventions, are also affected by this depth. Additionally, the length of the tunneled segment is pivotal as it can impact the number of branches affected by MB, particularly in the context of LAD MBs and their potential to affect diagonal or septal branches. This aspect holds significant clinical relevance [11]. Based on current classifications, it appears that individuals with isolated MB, which refers to MB without any accompanying CAD, do not demonstrate an increased incidence of high-risk stress test findings, which is diametrically opposite to the concept that MB inevitably results in impaired coronary blood flow (CBF). The intracoronary hemodynamic assessment estimates the functional significance of MB via pressure gradients and can provide valuable insights into inducible ischemia [14].
Almost 70%-95% of CBF in the coronary arteries occurs during the diastole when the myocardium relaxes, and there is no arterial compression [9]. Although an MB during systole theoretically should not affect CBF, studies revealed that arterial compression caused by a myocardial contraction can affect localized vasospasm [5,11]. As a result, there is a reduction of the diameter of the coronary artery by 34%-51%, an increase in blood flow velocities and retrograde flow, and reduced coronary flow reserve (CFR) - particularly in times of stress and exercise. The increased sympathetic tone from these states can induce tachycardia, resulting in decreased diastolic perfusion time and compromised myocardial perfusion [10]. Paradoxically, the vessel segment proximal to the MB demonstrates a significantly increased susceptibility to atherosclerosis, with reported rates approaching 90% attributed to hemodynamic alterations [7]. This accelerated plaque formation may be linked to changes in shear stress, which shifts from low shear stress at the tunnel entrance to high shear within the tunnel [7]. Endothelial cell morphology analysis at the tunneled segment entrance reveals a unique structure described as “flat, polygonal, and polymorphic,” indicating a low shear stress state. In contrast, within the MB, they exhibit a helical orientation, typically associated with laminar flow and high shear stress. The alteration in shear stress, the frictional force to flow, is proatherogenic and pro-inflammatory, leading to endothelial dysfunction and atherosclerosis development [15]. Additionally, there is an intricate milieu of vasoactive compounds such as endothelial nitric oxide synthase (eNOS), endothelin-1, and angiotensin-converting enzyme (ACE) in the proximal segment, which impact smooth muscle cell proliferation and atheroma formation. The presence of cardiovascular risk factors such as hypertension (HTN), diabetes mellitus (DM), and dyslipidemia (HLD) has been shown to amplify CAD proximal to the MB [15]. The MB segment is usually spared from atherosclerotic disease due to a thinner intima absence of smooth muscle cells and foam cells, which are integral in atherogenesis [7,10].
Electrocardiographic changes are frequent, but there are reported cases of pseudo-Wellens’ (biphasic T-waves or deep T-wave inversions in leads V2 and V3), VF, transient STE, and atrioventricular block [9,11,16,17]. Echocardiographic findings have revealed an abnormal left ventricular strain pattern, diastolic dysfunction, myocardial stunning, and SRC. Additionally, MB has been linked to LVH and hypertrophic cardiomyopathy (HCM) as it accentuates the supply-demand mismatch and augments compression of the microvascular vasculature [16,18]. Stress echocardiography may uncover septal bulking (a transient focal septal wall motion with apical sparing) and an abnormal strain pattern [9,19]. The classic angiographic feature is the systolic narrowing of the vessel, commonly called “milking,” which is characteristically described as a “step-down” to “step-up” phenomenon. This occurs when there is a greater than 70% reduction in the systolic luminal diameter, with complete or partial reduction in the luminal diameter persisting during systole. Despite this description, this is only demonstrated in 5% of cases [11].
Currently, management strategies primarily focus on pharmacotherapies such as beta-blockers (βBs) and non-dihydropyridine calcium-channel blockers (CCBs) [7]. Mitigating the hemodynamic consequences and reducing compression of the bridged segment are the mainstays of treatment. Protracting diastole with βBs could enhance CBF by extending the perfusion period. Additionally, reduced heart rates attenuate myocardial contractility, resulting in the lessening of systolic compression on the MB. CCBs offer a potential benefit in cases with suspected vasospasm due to their vasodilatory properties [11]. However, nitrates are generally contraindicated due to their ability to increase systolic compression, enhancing vessel wall compliance and contractility, potentially exacerbating the compression. As there is an emerging link between MB and accelerated atherosclerosis, the use of antiplatelets and statins have also been utilized [20]. In severe, refractory cases with persistent symptoms, surgical interventions like myotomy (resection of overlying muscle fibers), intracoronary stenting, and coronary artery bypass grafting (CABG) may be considered, however, long-term efficacy remains uncertain and requires further investigation [7]. There have been reports of stent fracture, in-stent restenosis (ISR), perforation, coronary artery dissection, and risk of graft occlusion [10].
Our patient displayed several key facets of MB, such as being male gender, the MB site being proximal to mid-LAD, approximately 30 mm in length. The compelling link was the presence of the widowmaker lesion despite his young age and the absence of conventional risk factors such as HTN, DM, HLD, and tobacco use. It must be acknowledged that the patient is of South Asian descent, and there were no lipoprotein(a) levels available in our setting, both of which are linked to increased, premature MACE [21-23]. Additionally, a dedicated CCTA was not performed. Thus, while we cannot definitively exclude that the widowmaker lesion was solely attributed to the severe MB, based on the above, the clinical scenario did not fit the classic de novo plaque rupture picture.
Conclusions
We describe the case report of a 37-year-old South Asian male with no established risk factors for CAD who presented with an NSTE-ACS with a coincident widowmaker lesion and severe MB. He was successfully managed with comprehensive GDMT and urgent PCI of the culprit lesion, sparing the MB segment. The definitive role of MB in atherosclerotic plaque formation within the Caribbean population warrants further investigation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Coronary anomalies: incidence, pathophysiology, and clinical relevance Circulation Angelini P Velasco JA Flamm S 2449245410520021202123510.1161/01.cir.0000016175.49835.57 · doi ↗ · pubmed ↗
- 2Myocardial bridging: contemporary understanding of pathophysiology with implications for diagnostic and therapeutic strategies J Am Coll Cardiol Corban MT Hung OY Eshtehardi P 234623556320142458330410.1016/j.jacc.2014.01.049PMC 4065198 · doi ↗ · pubmed ↗
- 3Myocardial bridging in adults 3 2024 2024 https://www.acc.org/latest-in-cardiology/articles/2020/08/04/08/48/myocardial-bridging-in-adults
- 4Left anterior descending artery stenosis: the widow maker revisited Mayo Clin Proc Holmes DR Jr Bell MR 111311157520001107573910.4065/75.11.1113 · doi ↗ · pubmed ↗
- 5Atherosclerosis and myocardial bridging: not a benign combination. An autopsy case report J Cardiovasc Dis Res Thej MJ Kalyani R Kiran J 176178320122262904410.4103/0975-3583.95380 PMC 3354469 · doi ↗ · pubmed ↗
- 6Myocardial bridges spared from atherosclerosis: overview of the underlying mechanisms Can J Cardiol Chatzizisis YS Giannoglou GD 2192222520091934034510.1016/s 0828-282x(09)70065-0PMC 2706759 · doi ↗ · pubmed ↗
- 7Myocardial bridging: an up-to-date review J Invasive Cardiol Lee MS Chen C-H 521528272015 https://www.hmpgloballearningnetwork.com/site/jic/articles/myocardial-bridging-date-review 25999138 PMC 4818117 · pubmed ↗
- 8Myocardial bridge: diagnosis, treatment, and challenges J Cardiothorac Vasc Anesth Freiling TP Dhawan R Balkhy HH Castillo J Cotter EK Chaney MA 395539633620223587188410.1053/j.jvca.2022.06.024 · doi ↗ · pubmed ↗