Unilateral arm weakness following retroperitoneal lymph node dissection for testicular germ cell tumour
S. Gaikwad, B. Trivedi, S. Gholap

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
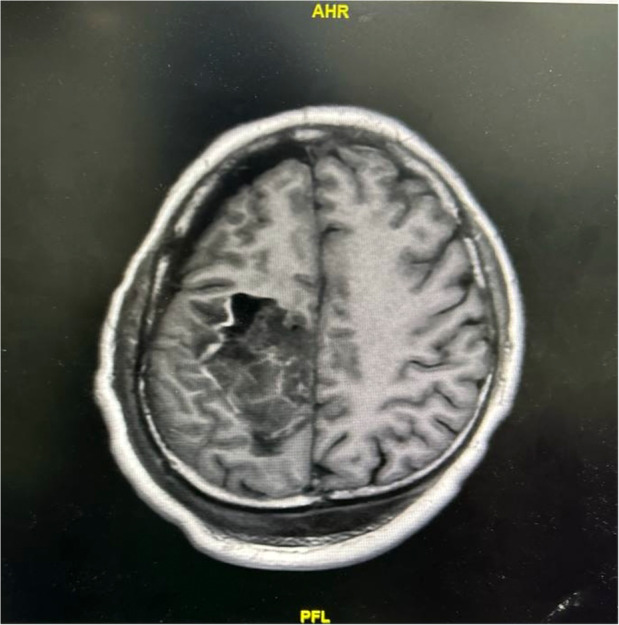 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTesticular diseases and treatments · Glioma Diagnosis and Treatment · Tuberous Sclerosis Complex Research
A 26‐year‐old man underwent retroperitoneal lymph node dissection following diagnosis of non‐seminomatous testicular germ cell tumour. He had previously undergone an inguinal orchidectomy. The surgery was performed under general anaesthesia with thoracic epidural for analgesia. Four hours after the start of surgery, tachycardia and hypotension developed which did not respond to fluid therapy. Therefore, intravenous noradrenaline infusion was started at a rate of 0.01–0.07 μg.kg^−1^.min^−1^ which was discontinued 2 h after surgery. During the operation, both arms were abducted to 90 degrees. At the end of the surgery, the patients' trachea was extubated and he was transferred to the intensive care unit. On the first postoperative day, the patient developed a left upper limb monoparesis without sensory deficit. Magnetic resonance imaging (MRI) of the brain and brachial plexus were undertaken. The MRI brain revealed a haemorrhagic lesion with surrounding oedema, leading to a diagnosis of symptomatic intratumoural bleed with raised intracranial pressure (Fig. 1). This was suspected to be a metastatic lesion as it was well‐defined and solitary. Testicular tumours can metastasise to the brain, although this is rare. The patient was treated with intravenous dexamethasone and received targeted radiotherapy which led to complete recovery of the arm weakness by postoperative day 21.
Brain metastases in non‐seminomatous testicular germ cell tumours are uncommon, but more likely to occur in those over 40, with elevated levels of β‐human chorionic gonadotropin (≥ 5000 IU.l^−1^) and alpha‐fetoprotein (> 10,000 ng.ml^−1^), pulmonary or bone metastases, and neurological symptoms. Due to the absence of these symptoms and low tumour marker levels, pre‐operative brain imaging was not performed in this case [1, 2]. The tumour markers were repeated and were within normal range.
In non‐seminomatous testicular germ cell tumours, spontaneous tumour bleed is rare, and while the patient's coagulation profile and platelets were normal, systemic immune response syndrome and immune suppression may have contributed to the bleeding risk. Systemic immune response syndrome may lead to increased metabolism and vascular complications, possibly influencing the occurrence of intratumoural bleeding [3, 4].
For us, the key point is that brain metastases can mimic anaesthetic complications, such as brachial plexus injury or a cerebrovascular accident. This highlights the need for a comprehensive differential diagnosis in the postoperative period to ensure accurate identification and management of underlying conditions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Le A , Arbab M , Adra N , Miller JC , Watson GA , Shiue K . Literature review of management of brain metastases from germ cell tumors. Chin Clin Oncol 2022; 11: 92687.10.21037/cco-21-12735400165 · doi ↗ · pubmed ↗
- 2Motzer RJ , Agarwal N , Beard C , et al. Clinical practice guidelines in oncology: testicular cancer. J Nat Compr Canc Netw 2009; 7: 672–693.10.6004/jnccn.2009.004719555582 · doi ↗ · pubmed ↗
- 3Boissonneau S , Graillon T , Rolland A , Botella C , Pallud J , Dufour H . Management of patients suffering from hemorrhagic intracranial metastases: propositions to help the neurosurgeon in emergency situations based on a literature review. Neurochirurgie 2021; 67: 369–374.33232711 10.1016/j.neuchi.2020.11.005 · doi ↗ · pubmed ↗
- 4Mihajlovic D , Draskovic B , Brkic S , Mitic G , Lendak D . Endothelial dysfunction and interaction between inflammation and coagulation in sepsis and systemic inflammatory response syndrome (SIRS). Health MED 2012; 6: 1309–1314.