Ventriculo-arterial (VA) coupling and fQRS as new selection criteria for primary prevention ICD placement
Nathan Engstrom, Hayley L. Letson, Kevin Ng, Geoffrey P. Dobson

TL;DR
This paper proposes using ventriculo-arterial coupling and fragmented QRS as better criteria for selecting heart failure patients for ICD implantation.
Contribution
The paper introduces a novel combination of VA coupling and fQRS for improved risk stratification in ICD placement.
Findings
LVEF is an inadequate predictor of sudden cardiac death in heart failure patients.
VA coupling and fQRS may better identify patients who would benefit from ICD therapy.
The proposed method could expand ICD eligibility to include patients with low and high LVEF.
Abstract
For decades, left ventricular ejection fraction (LVEF < 35%) has been a mainstay for identifying heart failure (HF) patients most likely to benefit from an implantable cardioverter defibrillator (ICD). However, LVEF is a poor predictor of sudden cardiac death (SCD) and ignores 50% of HF patients with mildly reduced and preserved LVEF. The current international guidelines for primary prophylaxis ICD therapy are inadequate. Instead of LVEF, which is not a good measure of LV contractility or hemodynamic characterization, we hypothesize ventriculo-arterial (VA) coupling combined with fragmented QRS (fQRS) will improve risk stratification and patient suitability for an ICD. Quantifying cardiac and aortic mechanics, and predicting active arrhythmogenic substrate, from varying fQRS morphologies, may help to stratify ischemic and non-ischemic patients with different functional capacities and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
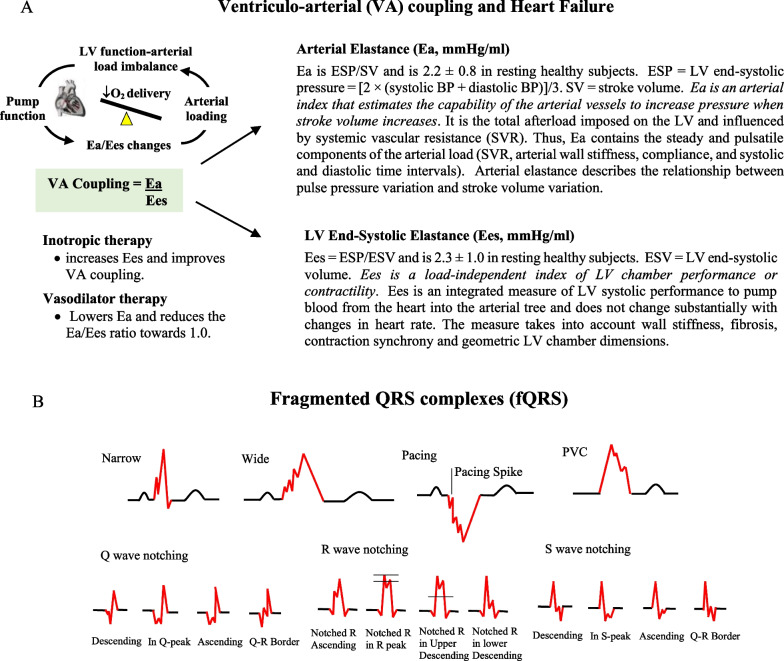 Figure 1
Figure 1- —http://dx.doi.org/10.13039/501100016058Townsville Hospital and Health Service
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac pacing and defibrillation studies · Cardiovascular Function and Risk Factors · Cardiac electrophysiology and arrhythmias
Current guidelines for ICD patient selection are inadequate
Chronic heart failure patients are predisposed to develop ventricular arrhythmias and sudden cardiac death (SCD) [1–4]. Deciding who should receive an implantable cardiac defibrillator (ICD) remains a difficult task. Despite the implantation of over 200,000 ICD devices globally each year, up to 70% of post-implantation deaths are not attributed to arrhythmic SCD [2–4]. The most commonly used prognostic tool for primary prophylaxis ICD is left ventricular fraction (LVEF) < 35% together with other HF symptoms [4, 5]. However, low LVEF alone does not predict lethal arrhythmias [4, 5], and SCD has been reported in nearly 40% of cardiovascular deaths in HF patients who have higher preserved LVEF [6, 7] and would not otherwise qualify for ICD assessment [5]. Clearly, the current international guidelines are inadequate and additional prognostic criteria are urgently required to maximize the benefit of ICD therapy.
LVEF is only part of the answer to ICD selection
LVEF is defined as the LV volume ejected per beat (stroke volume) expressed as a percentage of total ventricular volume (end-diastolic volume) [8, 9]. Although two-dimensional echocardiography or speckle tracking echocardiography remain gold standard measures in the diagnosis, choice of treatment and prognosis of LVEF in HF patients [8], it has a number of shortcomings [9]. First, LVEF is not a measure of intrinsic myocardial contractility [8, 10, 11], and second, it provides little information on the interaction between cardiac performance and the arterial system receiving the blood [1, 9, 12, 13]. Optimal performance requires the heart to pump blood into the vasculature at a rate and volume that matches the capability of the arterial tree to receive it. In short, LVEF fails to provide a “systems approach” to assessing cardiac performance in HF patients and identifying who may benefit from ICD therapy.
ventriculo-arterial coupling as an improved measure of mechanical performance
A fundamental link between central control, cardiovascular hemodynamics and tissue O_2_ supply is VA coupling [1, 12, 13]. VA coupling is the ratio of arterial elastance (Ea) to left-ventricular (LV) end-systolic elastance (Ees) and provides a measure of how efficiently blood is transferred from the heart to tissue mitochondria (Fig. 1A) [12, 14]. Ea incorporates the elements of arterial load, including peripheral vascular resistance, total arterial compliance, characteristic impedance, and systolic and diastolic time intervals, and Ees is a load-independent index of myocardial contractility and systolic stiffness (Fig. 1). When the Ea/Ees ratio is close to unity, the efficiency of material transfer is considered optimal, meaning that the left ventricle is providing sufficient stroke volume (SV) at its lowest possible myocardial energy consumption. If the ratio is excessively low or high, the heart as a pump and the vascular load become uncoupled and tissue perfusion and O_2_ supply is compromised [12, 15]. In HF patients, as arterial load increases to maintain systolic pressure, Ees decreases and cardiac performance declines, and this leads to VA uncoupling and inefficient contraction [16]. VA coupling in elderly patients with systolic dysfunction has been studied after treadmill exercise by Aslanger and colleagues [16], and in heart failure patients by Antohi and colleagues [17].Fig. 1A Ventriculo-Arterial (VA) coupling (Ea/Ees) is a measure of mechanical efficiency of heart performance and vascular load function to deliver sufficient O_2_ to the tissues [1, 12, 13]. The function of the arterial system is determined by the relationship between the stroke volume (SV) and end-systolic arterial pressure, where higher SVs lead to higher arterial end-systolic pressures [1, 12, 13]. The slope of this relationship is termed arterial elastance (Ea). Ees is a measure of cardiac contractility and a load-independent index of left ventricular (LV) chamber performance [1, 12, 13]. The advantage of VA coupling over LVEF or cardiac output (CO) is that it provides additional information on arterial loading and left ventricular function. ESP, end systolic pressure; BP, blood pressure. SVR, systemic vascular resistance; ESV, end systolic volume. B Different morphologies of fragmented QRS complexes (fQRS) in the 12-lead ECG by Das et al. [18] and modified fQRS Q, R and S criteria after Haukilahti et al. [2]. Modified after Engstrom et al. [20]
We hypothesize that VA coupling, and its components, will be a superior diagnostic and prognostic tool than LVEF for high-risk HF patients because: (1) the index provides a measure of both cardiac and vascular function, including LV functional capacity or physiological reserve; (2) it has the potential to capture all HF patients with low and preserved LVEF; (3) it can be measured using the routine, single-beat, non-invasive echocardiography method of Chen and colleagues [12, 17, 19]; and (4) it can be combined with other measures and risk factors to select patients who are more likely to benefit from ICD therapy.
Assessing non-viable myocardium and arrhythmogenic substrate
However, VA coupling alone, like LVEF, is insufficient to predict which patients are more likely to die from SCD. We propose combining VA coupling with fragmented QRS (fQRS) from a 12-lead electrocardiogram (ECG) to predict active arrhythmogenic substrate [17]. In a recent review we showed fQRS was associated with ventricular arrhythmias and all-cause mortality in primary prevention HF patients indicated for ICD implantation [3]. fQRS is the zig-zag notching and slurring of the QRS complex that indicates myocardial scarring and fibrosis [2, 20] (Fig. 1B). The size and location of scar or fibrotic region can further be quantified using late gadolinium enhancement cardiac magnetic resonance imaging (Ga-MRI) [4] or myocardial perfusion-gated scintigraphy (SPECT) [21]. Moreover, the different forms of fQRS in HF patients with ischemic cardiomyopathy (ICM) and non-ischemic cardiomyopathy (NICM) may be useful to predict different left ventricular remodelling, conduction defects and active arrhythmogenic substrate [2, 20], which may also be used for personalization of treatment. In summary, we hypothesize VA coupling and fQRS in high-risk HF patients may provide a superior prognostic measure of (1) cardiovascular function; (2) active arrhythmogenic substrate; and (3) SCD, compared to LVEF and HF symptoms.
Testing the hypothesis
The VA coupling-fQRS hypothesis could be tested in an observational study or prospective, randomized trial using the existing population of ICM and NICM patients with an ICD (LVEF < 35%). The study group should not have experienced a cardiac arrest and already receives routine standard-of-care If suitable, each patient will undergo additional echocardiographic measurements after treadmill exercise tests and stratified into different groups with different functional reserves and scar tissue characteristics [16]. Patient stratification includes using metabolic equivalents (METs), VA coupling, fQRS, Ga-MRI data, New York Heart Association (NYHA) classification and LVEF measurements. We hypothesize that chronic HF patients with low functional capacity (i.e. operating on a more flattened Frank Starling Curve) and minimal scar tissue (i.e. absence of fQRS) will not benefit from ICD therapy. We consider this group at lower risk of triggering severe ventricular arrhythmias [22, 23].
In contrast, we predict that HF patients with higher cardiac reserves (higher scope for activity) and the presence of fQRS (presence of scar tissue) will be more prone to enhanced automaticity, triggered activity and reentry and would benefit from an ICD. Following ICD guidelines, patients recruited in the trial will be monitored every 6 months over a 5-year period, and the study will be powered to include investigating sex-specific differences. Follow-up trials would include patients with low LVEF (< 35%), mid-range LVEF (40–49%) and preserved LVEF (≥ 50%). The latter would be of great interest because ~ 50% of HF patients worldwide have preserved LVEF [24, 25], and ~ 18% of these patients are reported to have fQRS [26]. This trial study has the potential to advance the field of ICD selection. In addition, the study offers an opportunity to include other ECG measures alongside fQRS, such as long QTc [27] or T-peak to T-end (Tpe), which are markers for SCD in the specific patient populations that may benefit from an ICD.
Conclusions
Identifying HF patients at high risk for developing fatal arrhythmias remains a major challenge in cardiology. To date, no measurement or marker has demonstrated utility in distinguishing which patient will derive benefit from ICD therapy. LVEF has a number of clinical shortcomings. We propose VA coupling combined with fQRS has the potential to redefine the risk stratification criteria for selecting which HF patients are best suited for ICD therapy and possibly improve outcomes. The combined approach may provide a more precision-based medical assessment for all HF patients compared to today’s highly restrictive and failed LVEF-based method.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ikonomidis I Aboyans V Blacher J Brodmann M Brutsaert DL Chirinos JA De Carlo M Delgado V Lancellotti P Lekakis J Mohty D Nihoyannopoulos P Parissis J Rizzoni D Ruschitzka F Seferovic P Stabile E Tousoulis D Vinereanu D Vlachopoulos C Vlastos D Xaplanteris P Zimlichman R Metra M The role of ventricular-arterial coupling in cardiac disease and heart failure: assessment, clinical implications and therapeutic interventions. A consensus document of the European Society of Cardiology Working Group on Aorta and Peripheral Vascular Diseases, Europea · doi ↗ · pubmed ↗
- 2Haukilahti MA Eranti A Kentta T Huikuri HVQRS fragmentation patterns representing myocardial scar need to be separated from benign normal variants: hypotheses and proposal for morphology based classification Front Physiol 2016765310.3389/fphys.2016.0065328082919 PMC 5183580 · doi ↗ · pubmed ↗
- 3Engstrom N Dobson GP Ng K Letson H Fragmented QRS is associated with ventricular arrhythmias in heart failure patients: a systematic review and meta-analysis Ann Noninvasive Electrocardiol 202127 e 1291010.1111/anec.1291034766402 PMC 8739614 · doi ↗ · pubmed ↗
- 4Klem I Klein M Khan M Yang EY Nabi F Ivanov A Bhatti L Hayes B Graviss EA Nguyen DT Judd RM Kim RJ Heitner JF Shah DJ Relationship of LVEF and myocardial scar to long-term mortality risk and mode of death in patients with nonischemic cardiomyopathy Circulation 20211431343135810.1161/CIRCULATIONAHA.120.04847733478245 · doi ↗ · pubmed ↗
- 5Shah KS Xu H Matsouaka RA Bhatt DL Heidenreich PA Hernandez AF Devore AD Yancy CW Fonarow GC Heart failure with preserved, borderline, and reduced ejection fraction: 5-year outcomes J Am Coll Cardiol 2017702476248610.1016/j.jacc.2017.08.07429141781 · doi ↗ · pubmed ↗
- 6Adabag S Langsetmo L Sudden cardiac death risk prediction in heart failure with preserved ejection fraction Heart Rhythm 20201735836410.1016/j.hrthm.2019.12.00931838199 · doi ↗ · pubmed ↗
- 7Wu S-J Hsieh Y-C Sudden cardiac death in heart failure with preserved ejection fraction: an updated review Int J Arrhythm.202223710.1186/s 42444-021-00059-3 · doi ↗
- 8Cikes M Solomon SD Beyond ejection fraction: an integrative approach for assessment of cardiac structure and function in heart failure Eur Heart J 2016371642165010.1093/eurheartj/ehv 51026417058 · doi ↗ · pubmed ↗