Long-Lasting Insecticidal Net Coverage and Utilization in Burla Town of Sambalpur District: A Cross-Sectional Study
Sanjeeb K Mishra, Gourahari Pradhan, Soumya R Patra, Ashok K Panigrahi, Subrat K Pradhan

TL;DR
This study assesses the coverage and use of insecticidal nets in Burla town, finding high availability but room for improvement in regular usage.
Contribution
The study provides new insights into LLIN coverage and utilization patterns in a specific Indian town and identifies factors influencing net usage.
Findings
Household-level LLIN coverage was 94.2%, but regular utilization was only 45.74%.
Skin reactions were the most common reason for not using LLINs, followed by low mosquito density.
Factors like number of bed nets, knowledge of malaria, and other mosquito control measures significantly predicted LLIN usage.
Abstract
Background Vector-borne diseases continue to significantly contribute to mortality and morbidity, especially in developing nations. Vector management is a key pillar in combating these diseases, and long-lasting insecticidal nets (LLINs) are cost-effective tools. The Government of India, under the National Vector Borne Disease Control Programme (NVBDCP), has distributed LLINs for free to increase coverage and utilization. This study aims to estimate the coverage and utilization of LLINs in Burla town. Method This cross-sectional study was conducted from October to December 2022 in Burla town of Sambalpur in Odisha, India. The estimated sample size was 510 households, assuming 50% coverage. Multi-stage cluster sampling was adopted to select the Anganwadi centers and households. A pretested questionnaire was utilized for data collection by trained personnel through Epicollect5 (Centre…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
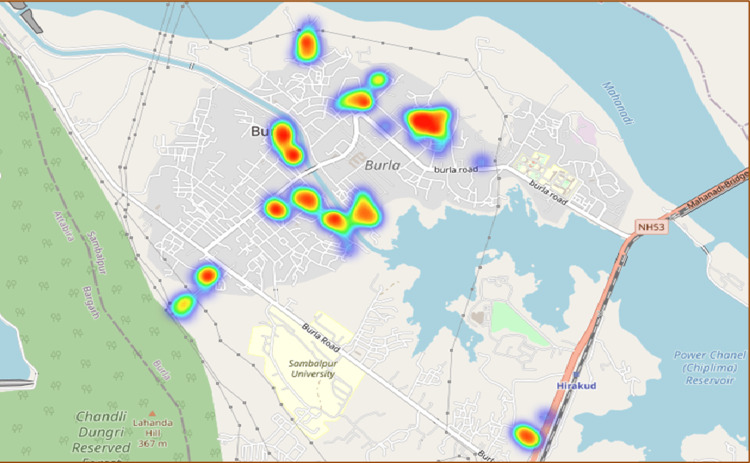 Figure 1
Figure 1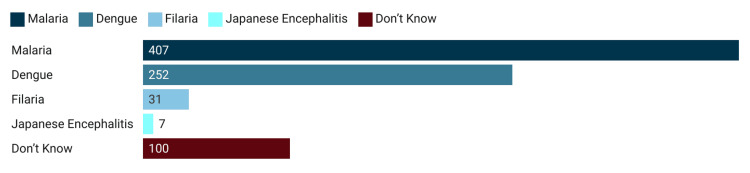 Figure 2
Figure 2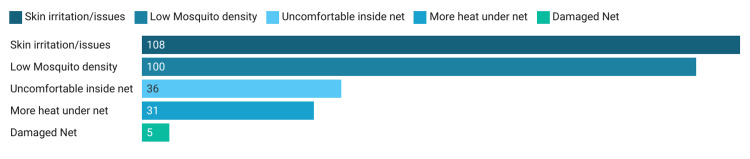 Figure 3
Figure 3| Variables | Categories | n | % |
| Age (in years) | ≤20 | 27 | 5.2 |
| 21-40 | 236 | 45.7 | |
| 41-60 | 212 | 41.1 | |
| ≥61 | 41 | 7.9 | |
| Gender | Female | 364 | 70.5 |
| Male | 152 | 29.5 | |
| Socio-economic status | Lower | 319 | 61.8 |
| Upper lower | 31 | 6.0 | |
| Lower middle | 125 | 24.2 | |
| Upper middle | 31 | 6.0 | |
| Upper | 10 | 1.9 | |
| Education | No education | 71 | 13.8 |
| Primary | 91 | 17.6 | |
| Secondary | 128 | 24.8 | |
| Matriculate | 148 | 28.7 | |
| 12th and above | 78 | 15.1 | |
| Number of family members | Four or less | 275 | 53.3 |
| Five or more | 241 | 46.7 | |
| Number of rooms | ≤ Two | 239 | 46.3 |
| Three to four | 225 | 43.6 | |
| ≥ Five | 52 | 10.1 | |
| Person per room | ≤ One | 121 | 23.4 |
| More than one to two | 234 | 45.3 | |
| ≥ Two | 161 | 31.3 | |
| Received long-lasting insecticidal nets | Yes | 466 | 90.3 |
| No | 50 | 9.7 | |
| Number of mosquito nets | Zero | 30 | 5.8 |
| One to two | 311 | 60.3 | |
| Three or more | 175 | 33.9 | |
| Washed the supplied net (466) | Yes | 421 | 90.3 |
| No | 45 | 9.7 | |
| Has any family member suffered from malaria, dengue, filariasis, or Japanese encephalitis | Yes | 29 | 5.6 |
| No | 487 | 94.4 | |
| Currently using mosquito net during sleeping | Yes | 236 | 45.7 |
| No | 280 | 54.3 |
| Variables | Categories | User, n (%) | Non-user, n (%) | P-value |
| Age | ≤20 | 7 (25.9) | 20 (71.1) | 0.138 |
| 21-40 | 108 (45.8) | 128 (54.2) | ||
| 41-60 | 104 (49.1) | 108 (50.9) | ||
| ≥61 | 17 (41.5) | 24 (58.5) | ||
| Gender | Female | 174 (47.8) | 190 (52.2) | 0.145 |
| Male | 62 (40.8) | 90 (59.2) | ||
| Socio-economic status | Lower | 149 (46.7) | 170 (53.3) | 0.455 |
| Upper lower | 17 (54.8) | 14 (45.2) | ||
| Lower middle | 55 (44%) | 70 (56.0) | ||
| Upper middle | 10 (32.3) | 21 (67.7) | ||
| Upper | 5 (50.0) | 5 (50.0) | ||
| Education | No education | 39 (54.9) | 32 (45.1) | 0.282 |
| Primary | 41 (45.1) | 50 (54.9) | ||
| Secondary | 50 (39.1) | 78 (60.9) | ||
| Matriculate | 71 (48.0) | 77 (52.0) | ||
| 12th and above | 35 (44.9) | 43 (55.1) | ||
| Number of family members | Four or less | 131 (47.6) | 144 (52.4) | 0.355 |
| Five or more | 105 (43.6) | 136 (56.4) | ||
| Received long-lasting insecticidal nets | Yes | 221 (47.4) | 245 (52.6) | 0.019 |
| No | 15 (30.0) | 35 (70.0) | ||
| Number of rooms | ≤ Two | 124 (51.9) | 115 (48.1) | 0.024 |
| Three to four | 89 (39.6) | 136 (60.4) | ||
| ≥ Five | 10 (40.0) | 15 (60.0) | ||
| Number of mosquito nets | Zero | 0 (0) | 30 (100) | 0.000 |
| One to two | 141 (45.3) | 170 (54.7) | ||
| Three or more | 95 (54.3) | 80 (45.7) | ||
| Adopt other measures to keep mosquitoes away | Yes | 165 (40.2) | 245 (59.8) | 0.000 |
| No | 71 (67.0) | 35 (33.0) | ||
| Washed the supplied net | Yes | 210 (49.9) | 211 (50.1) | 0.000 |
| No | 26 (27.4) | 69 (72.6) | ||
| Any family member suffered from malaria, dengue, filariasis, or Japanese encephalitis | Yes | 10 (34.5) | 19 (65.5) | 0.211 |
| No | 226 (46.4) | 261 (53.6) |
| Variables | B | SE | AOR-Exp B (95% CI) | P-value |
| Received LLIN | 0.21 | 0.40 | 1.234 (0.569, 2.780) | 0.600 |
| Number of rooms | -0.457 | 0.17 | 0.663 (0.450, 0.891) | 0.012 |
| Number of mosquito nets | 0.72 | 0.20 | 2.757 (1.389, 3.039) | 0.000 |
| Adopt other measures to keep mosquitoes away | -1.18 | 0.25 | 0.295 (0.189, 0.505) | 0.000 |
| Washed the supplied net | 0.58 | 0.30 | 1.920 (0.994, 3.205) | 0.028 |
| LLIN helps prevent malaria | 0.80 | 0.25 | 2.920 (1.368, 3.623) | 0.004 |
| Any family member suffered from malaria, dengue, filariasis, or Japanese encephalitis | 0.402 | 0.44 | 1.494 (0.628, 3.558) | 0.364 |
| Constant | 0.742 | 0.53 | 2.099 | 0.160 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInsect Pest Control Strategies · Mosquito-borne diseases and control · Agricultural pest management studies
Introduction
About one-fifth of all infections are vector-related diseases accounting for more than 700,000 deaths across the globe each year [1]. Mosquitoes are responsible for the majority of these cases [2]. Malaria is a parasitic infection caused by plasmodium species transmitted by female anopheline mosquitoes [1]. Dengue, a remerging disease, is a viral infection caused by the dengue virus (Flavivirus) transmitted by Aedes mosquitoes. Nearly four billion people in over a hundred countries are at risk of being affected by dengue, with nearly 100 million cases and an estimated 40,000 deaths every year [3]. Many vector-borne diseases are preventable, through protective measures, and community mobilization [1,2].
Integrated vector management is a key strategy that includes indoor residual spraying (IRS) in selected high-risk areas, insecticidal nets (ITNs) in high malaria endemic areas, use of larvivorous fish, anti-larval measures in urban areas, including bio-larvicides and minor environmental engineering, and source reduction for prevention of breeding. The WHO recommends widespread implementation of ITNs. Data from cluster randomized trials support the current policy recommendation for ITNs carried out between 1988 and 2013 that demonstrate the value of ITNs for public health [4].
Long-lasting insecticidal net (LLIN) is an advanced ITN that demonstrates sufficient entomological efficacy even after 20 washes conducted in a laboratory setting. In India, the government procured more than 47 million LLINs that were distributed during 2019-2020 to high-burden areas [5]. The use of LLINs is stated to be highly accepted by the community at large and has contributed to the drastic decline of malaria cases in the country [6].
With financial support from the World Bank and the governments of India and Odisha, anti-malaria activities have been accelerated to improve the delivery of services, especially in remote and inaccessible pockets [7]. The state has made significant progress in controlling malaria with a 90% reduction in the number of cases over the last five years due to targeted interventions [8]. The rate of reduction of vector-borne disease between 2018 and 2019 was 40% against the national average of 17% during the same period [8]. With active interventions, the annual parasite index (API) decreased to less than one per 1,000 population in 23 districts in 2020 compared to eight districts in 2016. Due to the rapid reduction in the positivity rate, the WHO has recorded the Odisha model as a best practice in its World Malaria Report of 2020 [9]. This was made possible due to integrated interventions like the state-led program called Durgama Anchlare Malaria Nirakarana (DAMaN). Around 2.8 crore people were protected from malaria with a distribution of 1.57 crore LLINs under DAMaN. Around 48,455 Accredited Social Health Activist (ASHA) workers were trained and engaged in the diagnosis and management of cases [10].
Studies on LLIN coverage and its ownership in Odisha are scarce. With this background, our study aims to estimate the LLIN coverage and its utilization in the Burla town of Sambalpur district in Odisha, India.
Materials and methods
This cross-sectional study was conducted in Burla town of Sambalpur district in Odisha state of India. Burla comprises more than 46,000 inhabitants, most of whom live in slums.
Sample size and sampling
Assuming that 50% of households owned at least one LLIN and using a precision of 5%, a confidence level of 95%, a non-response rate of 10%, and a design effect of 1.2, the estimated sample was 506 households. Multi-stage cluster sampling was followed. Anganwadi centers (AWCs) were the initial sampling units that were selected by arranging the 53 AWCs in alphabetical order and selecting 10 of them by random sampling with the help of a random number table. In each AWC area, 51 households were selected by random walk method.
Study design and procedures
A cross-sectional household survey study to estimate the coverage and assess the knowledge, attitude, and practice (KAP) was conducted just after the monsoon (rainy) season, between 1 October 2022 and 3 December 2022. In Sambalpur, two mass distributions of LLINs have taken place since its inception: first in 2016-2017 and second in 2020. The data collection was done by trained data collectors with the help of Epicollect5 (Centre for Genomic Pathogen Surveillance, Oxford, UK). Data collection and management interviews were conducted using structured questionnaires with household heads or, in their absence, with the partner or an adult permanently living in the house. The respondent was explained about the research project in detail and verbal consent was obtained before administering the questionnaire. Households were excluded from the study if the head of the household was not willing to participate or if no adults were available to answer the questionnaire after two separate visits. Interviews included questions on household characteristics, demographic information of all household members like education, occupation, income, number of family members (residents and long-term visitors sleeping in the same house), LLIN ownership, use of LLINs, alternative mosquito control measures, knowledge about diseases caused by mosquito and behavioral questions related to prevention from mosquito-borne diseases. The tool was tested for internal consistency and Cronbach's alpha was 0.67. The questionnaire also enquired about reasons for the non-usage of bed nets by the non-users.
The data collection tool recorded the location of the households, which is shown in Figure 1. The tool also has a provision for pictures of the net in the household with the additional consent of the respondent. Data collected through Epicollect5 was cleaned and analyzed using Epi Info (Centers for Disease Control and Prevention, Atlanta, GA). Categorical variables were expressed in frequency and percentages. Continuous variables were expressed in mean ± standard deviation. The association of variables with the usage of LLIN was tested using the chi-square test after the categorization of continuous variables. To identify the predictors for the usage of bed nets, binary logistic regression analysis was carried out. Analysis results are presented as odds ratios (ORs) with 95% confidence intervals. Approval was obtained before data collection from the Institutional Ethics Committee of Veer Surendra Sai Institute of Medical Sciences and Research.
Heat map of the area showing the surveyed clusters in Burla, Sambalpur, Odisha, 2022 (n = 516).
Results
The survey covered 516 households with 2,541 individuals and 1,165 nets. Among the surveyed households, 94.2% owned at least one bed net. About 1,107 (95%) of the nets in the households were LLIN supplied under the government scheme. Among the respondents, 364 (70.5%) were females. The age of the respondents ranged from 18 to 90 years, with a mean age of 41.89 (±14.6). The monthly family income of the respondents ranged from 3,000 to 500,000 with a mean of 16.99 thousand. Family size ranged from one to 26, with a mean of 4.92 and a standard deviation of 2.42. Person per room ranged from 0.25 to 11, with a mean of 2.04 ± 1.31. The mean number of nets (treated and untreated) owned per household was 2.26 with a standard deviation of 1.19. As far as the educational status of the head of the family is concerned, nearly 13.76% had no formal education, with a further 42.45% educated below 10th standard. As per the modified Kuppuswamy socioeconomic status scale, 236 households belonged to the lower class, 114 to the upper lower class, 125 to the lower middle class, 31 to the upper middle class, and 10 belonged to the upper class. About 90.3% of the surveyed households obtained nets during the free mass distribution campaign by the Ministry of Health and Family Welfare under the National Vector Borne Disease Control Programme. However, 364 (70.54%) of the households reported that the nets were not supplied to their houses rather they had to collect them from the health center. More than three-fourths of the households had two or more bed nets, six being the highest number of LLINs per family. More than 81% of the households washed the supplied bed nets before use. As far as knowledge about the benefits of mosquito nets is concerned, about 407 (78.88%) correctly identified protection from malaria, followed by dengue (n = 252, 48.84%), filaria (n = 31, 6.01%), and Japanese encephalitis (n = 7, 1.36%) (Figure 2).
Knowledge of participants on diseases prevented by the mosquito net in Burla, Sambalpur, Odisha, 2022 (n = 516).
Interestingly, only five (0.96%) of the respondents correctly answered all four diseases, and 28 (5.4%) identified three diseases. One hundred (19.4%) of the respondents failed to identify even a single mosquito-borne disease from the list (Figure 2). Only about 29 (5.62%) of the respondents could recall any of their family members suffering from the above-mentioned diseases in their lifetime. The socio-demographics are detailed in Table 1.
Usage of the LLIN was the main outcome of interest and about 236 (45.74%) of the respondents said they were using the nets regularly and slept under it on the previous night also. Nearly four-fifths (n = 429, 83.63%) of the respondents reported having used the supplied bed net at least once. Among the total households, 492 had children aged less than five years and about 104 (21.14%) of the households were using LLIN for their children as a regular practice. Among the non-users (n = 280), the reasons were skin reaction (n = 108, 38.57%), low mosquito density (n = 100, 35.71%), sleeping issues under the net (n = 36, 12.86%), increased heat inside the net (n = 31, 11.07%), and damaged net (n = 5, 1.78%) (Figure 3).
Reasons for non-usage of mosquito nets in Burla, Sambalpur, Odisha, 2022 (n = 280).
Additional/other measures were utilized by 411 (79.65%) of the households to keep mosquitoes away. These include vaporizer or Kachua Agarbati (231), closing doors and windows in the evening (127), burning egg cartons/cow dung (60), and using the net in the door and windows (34).
On the test for association with the chi-square test (on cross-tabulation), the number of rooms (p = 0.024), receiving mosquito nets (p = 0.019), number of bed nets per household (p = 0.000), washing the net (p = 0.000), and adopting other measures to keep mosquito away (p = 0.000) were found to be significantly associated with LLIN usage at an α of 0.05 (Table 2).
Multivariate logistic regression was used to identify predictors of net usage. The variables with p-values less than 0.1 were included in the regression analysis. The enter method was utilized for analysis. The omnibus test showed that the model was significant with an R2 of 0.192 and a correct prediction of 65% of cases. On logistic regression, the number of rooms (adjusted odds ratio (AOR) = 0.663, p = 0.012), number of bed nets (AOR = 2.757, p < 0.001), knowledge of malaria (AOR = 2.920, p = 0.04), adopting other measures for mosquito control (AOR = 0.295, p < 0.001), and washing the net (AOR = 1.920, p = 0.028) significantly predicted sleeping under the mosquito net (Table 3).
Discussion
The findings of this study highlight a high level of mosquito net ownership in the surveyed households, with 94.2% of households owning at least one net. A significant proportion of these nets, approximately 95%, were supplied under the government scheme, reflecting the success of government-led initiatives to increase LLIN distribution. These results are in line with previous research on LLIN ownership in regions with active government interventions in northeastern states and other parts of the world [11,12]. The high ownership rates can be attributed to nationwide programs aimed at combatting vector-borne diseases such as malaria and dengue [7].
A study from the high-burden region in Chhattisgarh reported 86% coverage, whereas Bihar reported 81% coverage in another study [13,14]. A study from West Bengal reported 100% coverage of LLIN whereas another from Purulia reported 96% coverage [15,16]. All these studies demonstrate the relatively high coverage of LLIN and demonstrate the efficacy of the government initiatives. However, a significant portion (70.54%) noted that they had to collect the nets from a health center, highlighting potential logistical challenges in the distribution process. The fact that over 81% of households washed the supplied bed nets before use indicates the transmission of government messages before LLIN use. Similar findings were reported by Prakash et al. in North India [11].
The usage of LLINs emerged as a significant area of interest. While approximately 45.74% of respondents reported regular LLIN usage and stated that they slept under the nets on the previous night and similar results were obtained by Millat-Martínez et al. [17]. However, higher usage from Chhattisgarh and West Bengal, and lower usage from Bihar were reported by other studies [13-15]. About 84% reported using the supplied bed nets at least once similar to the results reported by Millat-Martínez et al. [17]. Among households with children under five years old, about 21.14% practiced regular LLIN usage for their children similar to the findings by Millat-Martínez et al. at 19.9% [17].
The awareness of the benefits of mosquito nets was also evaluated. While approximately 78.88% correctly identified protection from malaria as a key benefit, awareness of other mosquito-borne diseases such as dengue, filaria, and Japanese encephalitis varied. These findings are similar to the study by Shrivathsa et al. in Mangaluru who reported 88% knowledge regarding malaria protection and Dey et al. in West Bengal [15,18]. Only a small fraction of respondents correctly identified all four diseases. This highlights the need for more comprehensive health education programs.
Skin reactions, low mosquito density, sleeping issues, heat inside the net, and damaged nets were identified to be common reasons for non-usage. Similar issues were also highlighted by other studies from this region [14,18]. Additional measures to repel mosquitoes were also employed by a substantial portion of the households, with vaporizers, closing doors and windows, burning egg cartons/cow dung, and using nets on doors and windows being popular choices.
The analysis of factors associated with LLIN usage revealed some interesting insights. Several persons per room, receiving a mosquito net, the number of bed nets per household, and washing the nets were all significantly associated with LLIN usage. These results suggest that household characteristics, availability of nets, and maintenance practices play a vital role in determining LLIN usage. Other studies also depicted similar associations [4,13,17].
Strength and limitations
The study is one of the few to provide these estimates and also provides an evaluation of the national program on vector-borne diseases in Odisha. The adopted questionnaire had a Cronbach's alpha of 0.67, which is of moderate to low internal consistency and may well have resulted from a limited number of items. The small geographical region may also be a limitation for the generalizability of the results.
Conclusions
To summarize, our study provides a comprehensive picture of LLIN coverage and ownership in the surveyed households. The high ownership rates and government interventions have contributed to widespread access to LLINs. The reasons for non-usage, such as skin reactions and discomfort, call for improved LLIN design and health education programs. Understanding the factors associated with LLIN usage is crucial for targeting interventions and ensuring the effectiveness of LLIN distribution programs. Further research, particularly through qualitative methods, can shed more light on the predictors of LLIN usage, facilitating evidence-based interventions to combat vector-borne diseases.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1WHO. Vector-borne diseases 5 2024 2020 https://www.who.int/news-room/fact-sheets/detail/vector-borne-diseases
- 2CDC. Climate and health: vector-borne diseases 5 2024 2020 https://www.cdc.gov/climate-health/php/effects/vectors.html?CDC_A Aref_Val=https://www.cdc.gov/climateandhealth/effects/vectors.htm
- 3WHO. Dengue and severe dengue 3 2024 2023 https://www.who.int/news-room/fact-sheets/detail/dengue-and-severe-dengue
- 4WHO. Achieving and maintaining universal coverage with long-lasting insecticidal nets for malaria control 3 2024 2017 https://www.who.int/publications/i/item/WHO-HTM-GMP-2017.20
- 5Ministry of Health & Family Welfare. Annual report: 2020-2021 4 2023 2021 https://main.mohfw.gov.in/sites/default/files/Annual%20Report%202020-21%20English.pdf
- 6Impact of long-lasting insecticidal nets on prevalence of subclinical malaria among children in the presence of pyrethroid resistance in Anopheles culicifacies in Central India Int J Infect Dis Chourasia MK Kamaraju R Kleinschmidt I Bhatt RM Swain DK Knox TB Valecha N 1231295720172826809610.1016/j.ijid.2017.02.001PMC 5384434 · doi ↗ · pubmed ↗
- 7Department of Health & Family Welfare. National Vector Borne Disease Control Programme (NVBDCP) 1 2024 2020 https://health.odisha.gov.in/healthnationaldiseasecontrol/national-vector-borne-disease-control-programme-nvbdcp
- 8New Indian Express. Odisha leads in malaria control with 90% reduction in cases 3 2022 2021 https://www.newindianexpress.com/states/odisha/2021/jun/26/odisha-leads-in-malaria-control-with-90-pc-reduction-in-cases-2321694.html