The association between heparin sensitivity index and postoperative blood loss in Chinese patients undergoing elective off-pump coronary artery bypass grafting: a single center retrospective study
Bin Jia, Chenying Ding, Jinhe Deng, Wenhui Qi, Yuntai Yao

TL;DR
This study found that the heparin sensitivity index does not affect postoperative blood loss in Chinese patients undergoing heart surgery, but high preoperative platelet counts are linked to lower heparin sensitivity.
Contribution
The study provides new evidence on the relationship between heparin sensitivity and postoperative outcomes in Chinese OPCAB patients.
Findings
Intraoperative heparin sensitivity index was not associated with postoperative blood loss.
Preoperative high platelet count was an independent predictor of low heparin sensitivity index.
No significant differences in transfusion requirements or complications were found between HSI groups.
Abstract
The heparin sensitivity index (HSI) is closely associated with perioperative ischemic events and increased blood loss in cardiac surgery. Previous studies have produced conflicting results. Therefore, this study aimed to investigate the relationship between HSI and postoperative blood loss specifically in Chinese patients undergoing elective off-pump coronary artery bypass grafting (OPCAB). Patients underwent OPCAB between March 2021 and July 2022 were retrospectively included. Enrolled patients were classified into Low-HSI (HSILOW; HSI < 1.3) and Normal-HSI (HSINORM; HSI ≥ 1.3) groups. HSI = [(activated clotting time (ACT) after heparin) – (baseline ACT)] / [loading dose of heparin (IU/kg)]. Primary outcome included postoperative blood loss at 24 h. Secondary outcomes were total postoperative blood loss, transfusion requirement of red blood cell (RBC), fresh frozen plasma (FFP),…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
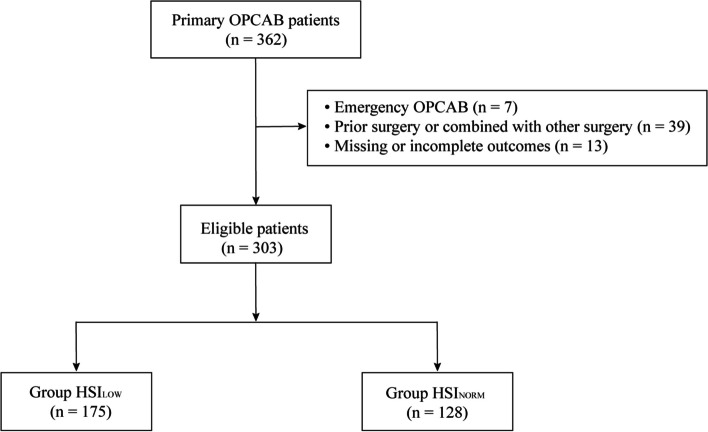 Figure 1
Figure 1- —The Youth Teacher Training Program of Peking Union Medical College
- —The Chinese Academy of Medical Sciences (CAMS) Initiative for Innovative Medicine
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac and Coronary Surgery Techniques · Venous Thromboembolism Diagnosis and Management · Acute Myocardial Infarction Research
Introduction
Unfractionated heparin (UFH) is widely used as an anticoagulant to prevent thromboembolic complications in cardiac surgery. However, the complex pharmacological properties of UFH may result in significant inter-patient variability in terms of responsiveness [1]. Various criteria are available for assessing heparin responsiveness: the general definition is whether UFH loading dose ranging from 150 IU/kg to 600 IU/kg can achieve a target activated clotting time (ACT) value of at least 300 s–600 s [2, 3]. To accommodate different UFH administration practices, some scholars have proposed using heparin sensitivity index (HSI) value to indicate differences in heparin responsiveness [4–6]. HSI is calculated using the following equation [5, 7].
\documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\text{HSI}=\frac{\text{postheparin ACT }\left(\text{s}\right)-\text{ baseline ACT}(\text{s})}{\text{loading dose of heparin }(\text{IU}/\text{kg})}$$\end{document}Previous studies have shown that low HSI value are associated with increased postoperative blood loss in cardiac surgery [8, 9]. However, these studies only enrolled patients undergoing on-pump cardiac surgery. The relationship between interoperative HSI and postoperative blood loss in patients undergoing off-pump coronary artery bypass grafting (OPCAB) remains unknown.
Therefore, this study aimed to investigate the relationship between interoperative HSI and postoperative blood loss in patients undergoing OPCAB to provide a basis for individualized anticoagulation.
Methods
Ethics approval
This study was approved by the ethics committee of Fuwai Hospital (20211636). The need for obtaining informed patient consent was waived due to the retrospective nature of this study.
Study population and design
Consecutive patients who underwent elective OPCAB at Fuwai Hospital between March 2021 and July 2022 were retrospectively enrolled. The inclusion criteria were as follows: (1) adult patients (> 18 years of age) and (2) patients undergoing OPCAB. Exclusion criteria were as follows: (1) emergency surgery, (2) previous cardiac surgery, (3) OPCAB combined with other surgery, (4) use of an intra-aortic balloon pump (IABP) prior to surgery, (5) a history of heparin-induced thrombocytopenia, (6) abnormal preoperative coagulation, thrombotic, or hematological diseases, (7) renal failure (serum creatinine > 200 mmol/L or urine output < 10 mL/h), (8) liver dysfunction (alanine aminotransferase, aspartate aminotransferase, alkaline phosphatase, or total bilirubin levels two times higher than the upper limit of normal), and (9) infectious endocarditis.
Anesthetic and surgical protocols
General anesthesia was induced with midazolam 0.1 mg/kg, etomidate 2 mg/kg, sufentanil 2 μg/kg–3 μg/kg, and cis-atracurium 0.15 mg/kg–0.2 mg/kg. Propofol 100 mg/h–200 mg/h, dexmedetomidine 30 μg/h–50 μg/h, cis-atracurium 8 mg/h–15 mg/h, and sevoflurane 0.5%–1.5% were administered for anesthesia maintenance. Median sternotomy was performed on all patients. Bispectral index (BIS) was maintained between 40 and 60 during surgery. All patients received intraoperative autologous blood salvage using cell-saver systems. No patient received tranexamic acid. The patients were transferred to the intensive care unit (ICU) for postoperative care, and aspirin and clopidogrel were administered on the first postoperative day.
Heparin sensitivity index
Patients underwent radial artery catheterization under local anesthesia prior to general anesthesia, and a 0.5 mL blood sample was collected from each patient's radial artery to determine baseline ACT. The Hemochron Signature Elite Response Whole Blood Coagulation System (International Technidyne Corporation (ITC), San Diego and Edison, USA) was used to monitor ACT using a Hemochron ACT^+^ cartridge (kaolin and silica activators). With a UFH loading dose of 200 IU/kg was used to achieve an activated ACT value of at least 300 s. Five minutes after UFH administration, a blood sample (0.5 mL) was collected from the radial artery to determine the post-heparin ACT. UFH 100 IU/kg was administered hourly following the initial dose, with the maintenance of an intraoperative ACT value ≥ 300 s [10]. UFH was neutralized with 2 mg/kg protamine after the conclusion of revascularization. ACT was subsequently measured 10 min after protamine neutralization. The criterion used to indicate reduced heparin responsiveness was HSI value < 1.3 [7]. HSI value ≥ 1.3 was considered to indicate normal heparin responsiveness. Enrolled patients were classified into two groups, namely Low-HSI (HSI_LOW_; HSI < 1.3) and Normal-HSI (HSI_NORM_; HSI ≥ 1.3) groups.
Primary and secondary outcomes
The primary outcome was postoperative blood loss at 24 h. The secondary outcomes included total postoperative blood loss, transfusion requirement of red blood cell (RBC), fresh frozen plasma (FFP), and platelet concentrates (PC), postoperative mechanical ventilation duration, chest drainage duration, length of stay (LOS) in the ICU and hospital, incidences of reoperation for blood loss, cardiac arrest, myocardial infarction (MI), use of IABP, atrial fibrillation (AF), pacemaker implantation, neurological events (stroke and transient ischemic attack), delirium, renal replacement therapy, and mortality.
Criteria for allogeneic transfusions and outcomes measures
Blood products were transfused according to the following protocols: the transfusion threshold for RBC was hemoglobin < 8.0 g/L. The indication for FFP transfusion was diffuse blood loss with a prothrombin time value 1.5 times longer than the baseline value. The triggers for PC transfusion were a platelet (PLT) count of < 50 × 10^9^/L or PLT dysfunction. Postoperative blood loss was defined based on the chest drainage volume. The patient underwent reoperation if the postoperative chest drainage volume exceeded 300 mL/h within the first 2 h or remained above 200 mL/h for 4 h. Removal of the chest drainage tubes was only considered when discharge fell below 20 mL for a period of at least 5 h–6 h [10]. Antiplatelet therapy (aspirin and/or clopidogrel) was discontinued on admission. Antithrombotic prophylaxis consisted of subcutaneous administration of low-molecular-weight heparin (LMWH) from admission until 12 h prior to surgery. Preoperative use of clopidogrel was defined as cessation within five days, whereas preoperative use of aspirin was defined as cessation within six days [11]. The protamine/UFH dose ratio was determined using the following formula: 1 mg of protamine per 100 IU of UFH. Clinical diagnostic criteria for MI were defined as the occurrence of an increase in cardiac enzyme levels five times higher than the upper limit of normal, at the same time, it must satisfy at least one of the following conditions: newly developed ischemic electrocardiographic changes, new Q-waves formation on electrocardiogram, imaging evidence of new myocardial infarction or new localized abnormal ventricular wall motion. Cerebral stroke was defined as a novel focal or global cerebral dysfunction that persisted for more than 24 h.
Statistical analysis
The previous study [8] showed that the weighted mean difference in postoperative blood loss at 24 h between patients with Low-HSI and Normal-HSI undergoing cardiac surgery was 95 ml, with a standard deviation of 218.5 ml. Based on an independent t-test, we calculated that a sample size of 226 patients would be required to achieve a power of 90% at a two-sided significance level of 0.05. Considering a potential dropout rate of 20%, the minimum sample size was 272 patients. Our final sample size was increased to include 303 patients.
Categorical variables were used the χ^2^ test and expressed as numbers and percentage. Continuous variables were used the Wilcoxon rank-sum test and expressed as median and interquartile range. Repeated measurements of data were analyzed using two-way repeated measures analysis of variance, with data presented as mean ± standard deviation. A multivariate logistic regression model was used to examine the clinical and laboratory predictors of HSI. Baseline variables that were considered clinically relevant or variables with P < 0.20 in the univariate analysis were entered into the multivariable logistic regression model. The variables for inclusion were carefully chosen, given the number of events available, to ensure parsimony in the final model. P < 0.05 was considered to indicate statistical significance. All statistical analyses were performed using SPSS software (SPSS version 23.0; IBM Corp., Armonk, USA).
Results
Study population
From March 2021 to July 2022, 362 patients underwent elective OPCAB, and this retrospective analysis ultimately included 303 cases (Fig. 1). Among them, 175 (57.76%) patients were classified into HSI_LOW_ group, whereas the remaining 128 (42.24%) patients were assigned to HSI_NORM_ group.Fig. 1. Flowchart of the study. OPCAB, off-pump coronary artery bypass grafting; HSI_LOW_, HSI value < 1.3; HSI_NORM_, HSI value ≥ 1.3
Characteristics of the patients and preoperative parameters
Table 1 showed the characteristics of the enrolled patients. HSI_LOW_ group had higher preoperative PLT count (221 × 10^9^/L vs. 202 × 10^9^/L; P = 0.041) and platelet crit (PCT) value (0.23% vs. 0.22%; P = 0.040) compared to HSI_NORM_ group. Table 1. Characteristics of enrolled patients [median (IQR) or cases (%)]VariablesHSI_LOW_ (n = 175)HSI_NORM_ (n = 128)P valueAge (years)63.00 (55.50, 68.00)62.50 (56.00, 67.25)0.930Male (%)141 (80.6)96 (75.0)0.308BMI (kg/m^2^)25.80 (22.49, 29.01)26.87 (23.02, 30.81)0.107Smoker (%)86 (49.1)69 (53.9)0.413Hypertension (%)112 (64.0)85 (66.4)0.755Diabetes mellitus (%)72 (41.1)53 (41.4)1.000Hyperlipidemia (%)147 (84.0)116 (90.6)0.131COPD (%)3 (1.7)0 (0.0)0.367Neurological events (%)31 (17.7)23 (18.0)1.000LVEF (%)61.00 (57.00, 65.00)62.00 (58.00, 65.00)0.229AF (%)5 (2.9)3 (2.3)1.000Prior MI (%)0 (0.0)0 (0.0)NAPrior PH (%)2 (1.1)0 (0.0)0.620Statins (%)165 (94.3)122 (95.3)0.693β-blockers (%)137 (78.3)104 (81.2)0.626ARB (%)46 (26.3)38 (29.7)0.513ACEI (%)14 (8.0)10 (7.9)0.968Nitrates (%)159 (90.9)118 (92.2)0.841Preoperative use of clopidogrel (%)3 (1.7)6 (4.7)0.515Preoperative use of aspirin (%)12 (6.9)13 (10.2)0.781Preoperative use of LMWH (days)4.00 (2.00, 5.00)4.00 (2.00, 6.00)0.245Blood type A (%)54(30.9)35(27.3)0.507Blood type B (%)64(36.6)47(36.7)0.979Blood type AB (%)13(7.4)17(13.3)0.092Blood type O (%)44(25.1)29(22.7)0.617Hemoglobin (g/L)138.00 (126.00, 147.00)135.00 (125.00, 147.00)0.375PLT count (10^9^/L)221.00 (179.50, 258.50)202.00 (169.25, 253.00)0.041Platelet distribution width (fL)12.20 (11.10, 13.15)12.00 (11.30, 13.40)0.466Mean platelet volume (fL)10.60 (10.00, 11.10)10.50 (9.88, 11.13)0.437Platelet-large cell rate (%)29.00 (24.30, 33.00)29.20 (25.00, 34.00)0.435PCT (%)0.23 (0.20, 0.27)0.22 (0.18, 0.26)0.040PT (seconds)13.00 (12.55, 13.40)12.95 (12.58, 13.50)0.935INR (ratio)0.97 (0.94, 1.02)0.98 (0.94, 1.01)0.913APTT (seconds)35.70 (33.45, 38.45)35.30 (32.50, 37.60)0.201Fibrinogen (g/L)3.35 (2.91, 3.87)3.35 (3.04, 3.82)0.599D-dimer assay (mg/L)0.25 (0.21, 0.39)0.27 (0.21, 0.39)0.543FDP (mg/L)2.50 (2.50, 2.50)2.50 (2.50, 2.50)0.459PAg-AA (%)15.97 (7.00, 77.58)27.18 (7.86, 76.21)0.823PAg-ADP (%)59.30 (40.02, 72.98)56.25 (39.10, 70.97)0.322PAg-ADR (%)73.59 (26.76, 84.92)55.56 (41.78, 72.92)0.643PAg-COL (%)77.04 (41.34, 85.00)69.27 (61.08, 74.85)0.440Protein C (%)109.00 (94.50, 118.50)102.00 (89.25, 121.00)0.633Protein S (%)98.10 (82.70, 119.15)98.60 (76.03, 127.50)0.861Antithrombin III (%)98.00 (86.50, 109.00)99.50 (87.50, 107.00)0.611vWF: Ag (%)181.75 (134.58, 214.22)148.00 (124.58, 195.87)0.278Hypersensitive troponin (ng/mL)0.007 (0.003, 0.022)0.007 (0.004, 0.012)0.813Myoglobin (ng/mL)33.68 (25.75, 44.04)35.79 (23.95, 41.72)0.760CK (ng/mL)57.00 (43.25, 83.75)61.00 (43.00, 83.00)0.843CK-MB (ng/mL)0.92 (0.63, 1.32)0.88 (0.66, 1.19)0.293NTpro-BNP (pg/mL)219.00 (74.00, 517.00)209.00 (80.18, 481.00)0.855Albumin (g/L)39.80 (37.35, 42.15)40.10 (38.00, 43.00)0.059ALT (U/L)20.00 (13.50, 28.50)23.50 (15.75, 34.25)0.730AST (U/L)25.00 (20.00, 29.50)26.00 (22.00, 33.00)0.445Creatinine (μmol/L)82.46 (71.50, 97.08)84.36 (74.23, 95.72)0.588Cystatin C (mg/L)0.94 (0.77, 1.06)0.93 (0.81, 1.07)0.193hs-CRP (mg/L)0.87 (0.52, 2.57)1.02 (0.44, 1.84)0.388CRP (mg/L)2.36 (1.74, 4.31)2.38 (1.63, 3.54)0.183ACEI Angiotensin-converting enzyme inhibitors, AF Atrial fibrillation, ALT Alanine transaminase, ARB Angiotensin receptor inhibitors, APTT Activated partial thromboplastin time, AST Aspartate aminotransferase, BMI Body mass index, CK Creatine kinase, CK-MB Creatine kinase isoenzyme, COPD Chronic obstructive pulmonary disease, CRP C-reactive protein, FDP Fibrinogen degradation products, hs-CRP Hypersensitive C-reactive protein, INR International normalized ratio, IQR Interquartile range, LMWH Low-molecular-weight heparin, LVEF Left ventricular ejection fraction, MI Myocardial infarction, NA Not applicable, Neurological events Cerebral stroke or transient ischemic attack, NT pro-BNP Amino-terminal pro-brain natriuretic peptide, PAg-AA Platelet aggregation test-arachidonic acid, PAg-ADP Platelet aggregation test-adenosine diphosphate, PAg-ADR Platelet aggregation test-adrenalin, PAg-COL Platelet aggregation test-adrenalin, PCT Platelet crit, PH Pulmonary hypertension, PLT Platelet, PT Prothrombin time, vWF von Willebrand factor
Intraoperative parameters
Intraoperative parameters were summarized in Table 2. The difference in baseline ACT value (111.95 ± 10.88 s vs. 110.43 ± 10.19 s; P = 0.233) and ACT value after protamine neutralization (121.29 ± 11.95 s vs. 122.14 ± 13.34 s; P = 0.624) between HSI_LOW_ group and HSI_NORM_ group were not statistically significant. However, ACT value after initial UFH administration in HSI_NORM_ group was higher than that in HSI_LOW_ group [73.64 s, 95% confidence interval (CI): -79.28, -68.01; P < 0.001). The dose of protamine in HSI_LOW_ patients was less than that in HSI_NORM_ group (150 mg vs. 160 mg; P = 0.005), but the two groups showed no significant differences in dose of UFH (21,300 IU vs. 22,200 IU; P = 0.158) and protamine/UFH dose ratio (0.67 vs. 0.68; P = 0.287). Table 2. Intraoperative parameters [median (IQR), cases (%), or x̄ ± s]VariablesHSI_LOW_ (n = 175)HSI_NORM_ (n = 128)P valueACT value baseline ACT111.95 ± 10.88110.43 ± 10.190.233 ACT after initial UFH administration326.84 ± 39.80400.48 ± 34.380.000 ACT after protamine neutralization121.29 ± 11.95122.14 ± 13.340.624Surgery duration (minutes)207 (178, 230)205.00 (179, 231)0.780Infused fluid volume (mL)1,900 (1,500, 2,200)2,000 (1,700, 2,500)0.730Pulmonary artery catheter insertion (%)100 (57.1)77 (60.6)0.625UFH (IU)21,300 (17,700, 24,600)22,200 (18,000, 25,800)0.158Protamine (mg)150 (130, 170)160 (140, 180)0.005Protamine/UFH dose0.67 (0.65, 0.77)0.68 (0.65, 0.82)0.287ACT Activated clotting time, IQR Interquartile range, UFH Unfractionated heparin
Postoperative parameters and complications
Postoperative parameters were shown in Table 3. The two groups showed no significant differences in terms of postoperative blood loss at 24 h (460 mL vs. 470 mL; P = 0.252), total blood loss (920 mL vs. 980 mL; P = 0.063), and transfusion requirement of RBC (3.4% vs. 3.1%; P = 1.000) and FFP (3.4% vs. 6.2%; P = 0.380). In addition, HSI_LOW_ and HSI_NORM_ groups showed no significant differences in terms of postoperative mechanical ventilation duration (MVD) (16 h vs. 16 h; P = 0.776), chest drainage duration (4 days vs. 4 days; P = 0.757), ICU LOS (46 h vs. 45 h; P = 0.114), hospital stay (7 days vs. 7 days; P = 0.329), and other complications. No patient in either group required PC transfusion or died during the postoperative hospitalization period. In thrombelastography, HSI_LOW_ group showed a shorter kinetics time (2.20 min vs. 2.50 min; P = 0.010) and a larger alpha angle (58.50° vs. 54.10°, P = 0.003) than HSI_NORM_ group. Table 3. Postoperative parameters [median (IQR) or cases (%)]VariablesHSI_LOW_ (n = 175)HSI_NORM_ (n = 128)P valuePostoperative blood loss at 24 h (mL)460 (350, 600)470 (380, 640)0.252Total postoperative blood loss (mL)920 (685, 1235)980 (817, 1250)0.063RBC transfusion rate (%)6 (3.4)4 (3.1)1.000FFP transfusion rate (%)6 (3.4)8 (6.2)0.380PC transfusion rate (%)0 (0.0)0 (0.0)NARBC transfusion volume (unit)2 (2, 2)2 (2, 2)0.841FFP transfusion volume (mL)400 (0, 400)400 (400, 400)0.143PC transfusion volume (mL)0 (0, 0)0 (0, 0)NAMVD (hours)16.00 (13.00, 18.00)16.00 (13.00, 18.00)0.776Chest drainage duration (days)4.00 (4.00, 5.00)4.00 (4.00, 5.00)0.757LOS in the ICU (hours)46.00 (23.00, 93.00)45.00 (22.00, 71.00)0.086LOS in the hospital (days)7.00 (6.00, 8.00)7.00 (6.00, 8.00)0.329Mortality (%)0 (0.0)0 (0.0)NAReoperation (%)3 (1.7)4 (3.1)0.674Cardiac arrest (%)0 (0.0)0 (0.0)NAMI (%)0 (0.0)0 (0.0)NAIABP (%)2 (1.1)0 (0.0)0.225AF (%)2 (1.1)2 (1.6)1.000New pacemaker (%)0 (0.0)0 (0.0)NANeurological events (%)0 (0.0)1 (0.8)0.875Delirium (%)2 (1.1)1 (0.8)1.000Renal replacement therapy (%)0 (0.0)0 (0.0)NADopamine (%)157 (89.7)115 (89.8)1.000Nitroglycerin (%)118 (67.4)81 (63.3)0.530Norepinephrine (%)64 (36.6)52 (40.6)0.550Thromboelastographyreaction time (minutes)7.10 (6.10, 8.40)7.55 (6.38, 8.35)0.134kinetics time (minutes)2.20 (1.80, 2.60)2.50 (1.90, 2.92)0.010Alpha angle (degrees)58.50 (53.35, 63.25)54.10 (48.88, 60.20)0.003maximum amplitude (millimeters)55.60 (50.60, 61.20)53.85 (48.97, 60.20)0.195lysis at 30 min (%)0.10 (0.10, 0.20)0.10 (0.10, 0.30)0.195Blood coagulation factorsII (%)82.90 (78.10, 88.10)93.10 (76.90, 100.45)0.249V (%)106.00 (96.15, 121.80)108.70 (105.95, 116.00)0.311VII (%)71.80 (60.85, 83.57)71.80 (65.55, 85.50)0.639X (%)82.35 (67.85, 90.33)82.10 (75.80, 95.70)0.888VIII (%)122.20 (100.38, 149.15)121.10 (102.80, 145.00)0.961IX (%)114.10 (107.53, 138.67)107.60 (97.55, 129.50)0.336XI (%)105.20 (85.00, 119.40)90.20 (85.80, 100.50)0.269XII (%)74.30 (62.23, 92.17)60.40 (53.00, 85.50)0.183Big-endothelin (pmol/L)0.42 (0.31, 0.56)0.46 (0.37, 0.61)0.379IL-1β (pg/mL)1.69 (1.12, 2.24)1.59 (0.99, 2.33)0.589IL-2 (pg/mL)1.54 (1.31, 1.96)1.56 (1.31, 2.08)0.588IL-4 (pg/mL)1.54 (1.00, 2.04)1.50 (1.05, 2.12)0.831IL-5 (pg/mL)1.38 (1.14, 1.86)1.27 (1.09, 1.65)0.261IL-6 (pg/mL)134.87 (82.65, 202.58)135.43 (84.20, 234.44)0.445IL-8 (pg/mL)40.00 (24.90, 58.00)44.29 (31.69, 62.92)0.167IL-10 (pg/mL)9.75 (5.88, 16.08)10.93 (6.62, 19.39)0.160IL-12 (pg/mL)1.86 (1.10, 2.71)1.92 (1.00, 2.83)0.724IL-17 (pg/mL)2.73 (0.01, 6.04)3.24 (0.37, 5.68)0.750TNF-a (pg/mL)1.78 (1.18, 2.99)1.66 (1.01, 2.66)0.233IFN-a (pg/mL)1.67 (1.16, 2.26)1.67 (1.19, 2.22)0.724IFN-γ (pg/mL)1.44 (1.07, 1.93)1.48 (1.04, 1.93)0.954AF Atrial fibrillation, FFP Fresh frozen plasma, IABP Intra-aortic balloon pump, ICU Intensive care unit, IFN Interferon, IL Interleukin, IQR Interquartile range, LOS Length of stay, MI myocardial infarction, MVD Mechanical ventilation duration, NA Not applicable, Neurological events Cerebral stroke or transient ischemic attack, PC Platelet concentrates, RBC Red blood cell, TNF Tumor necrosis factor
Multivariable logistic regression analysis
Ten variables were included in multivariate logistic regression analysis (Table 4). Age, sex, and duration of preoperative LMWH use were considered clinically relevant variables [12–15]. The other seven variables showed P < 0.20 in the univariate analysis. Although the proportion of blood type AB among preoperative patients showed P < 0.20 in the univariate analysis, owing to the limited number of available events, this factor was not included in the multivariate logistic regression analysis. High preoperative PLT count (odds ratio: 1.006; 95% CI: 1.002, 1.011; P = 0.008) was significantly associated with low intraoperative HSI value. Table 4. Multivariate logistic regression analysis for heparin sensitivity indexPredictorsBOR (95% CI)P valueAge0.0161.015 (0.702, 2.547)0.296Male0.2741.337 (0.702, 2.547)0.377BMI– 0.0420.959 (0.916, 1.005)0.080Hyperlipidemia– 0.5090.601 (0.277, 1.302)0.197PLT count0.0061.006 (1.002, 1.011)0.008PCT–0.1960.820 (0.393, 1.713)0.598Albumin– 0.0260.973 (0.926, 1.022)0.271Cystatin C– 0.2040.809 (0.419, 1.562)0.528CRP0.0691.069 (0.992, 1.152)0.790LMWH– 0.0390.967 (0.877, 1.066)0.497B Regression coefficient, BMI Body mass index, CI Confidence interval, CRP C-reactive protein, LMWH Low-molecular-weight heparin, OR Odds ratio, PCT Platelet crit, PLT platelet
Discussion
This study showed no increase in postoperative blood loss at 24 h in Chinese patients with a low HSI undergoing elective OPCAB. In the assessment of risk factors for low intraoperative HSI value, preoperative high PLT count was identified as an independent predictor.
The low intraoperative HSI value is associated with concerns regarding potential overactivation of the clotting system due to inadequate anticoagulation, necessitating the administration of additional UFH. However, this exposes surgical patients to the risk of excessive UFH use [8]. Furthermore, repeated administration of UFH at doses exceeding the predicted range may necessitate increased protamine administration to counteract the effects of UFH, thereby exposing patients to the risk of protamine overdose [9]. An excess of protamine can attenuate thrombin-induced PLT aggregation and reduce the responsiveness of PLT to thrombin receptor agonist peptides. Additionally, excessive protamine administration weakens clot strength and shortens the time for clot lysis while promoting fibrinolysis mediated by tissue-type plasminogen activators, thereby facilitating clot breakdown [16]. These factors may contribute to increased postoperative blood loss. In this study, although the ACT value after initial UFH administration in HSI_LOW_ group was lower than that in HSI_NORM_ group, there was no increase in blood loss at 24 h or transfusion requirement was observed after OPCAB in HSI_LOW_ group. The plausible reasons for these findings are as follows: the use of UFH in HSI_LOW_ group was not greater than that in HSI_NORM_ group. Similarly, the protamine/UFH dose ratio in both groups ranged from 0.6 to 0.7 and did not differ significantly between the two groups. The reaction time of the TEG after surgery in both groups, which indicated the onset of measurable clot strength, showed no residual effect of UFH. Some studies have demonstrated a half-dose of protamine can safely reverse UFH without increasing postoperative blood loss [17, 18]. In this regard, a protamine/UFH dose ratio ranging from 0.6 to 0.7 is considered an appropriate neutralization ratio.
Another crucial factor that cannot be overlooked is the perioperative coagulation profile of OPCAB, which exhibits a lower degree of coagulation-fibrinolysis activation and PLT dysfunction [19, 20]. Moreover, in comparison with on-pump cardiac surgery, OPCAB circumvents the impact of hemodilution and hypothermia on the coagulation system [8]. The aforementioned factors collectively contribute to the development of a procoagulant state following OPCAB. Postoperative TEG revealed coagulation characteristics, indicating accelerated blood clot formation, as evidenced by the K value in both groups falling below the lower limit of normal (4 min–9 min). The K value was shorter and the alpha angle was larger in HSI_LOW_ group than in HSI_NORM_ group, indicating higher procoagulant activity reflective of increased fibrinogen function. Previous studies have highlighted potential thromboembolic risks associated with reduced heparin responsiveness [7]. Inadequate response to UFH may result in intraoperative and postoperative coagulation within the peripheral vascular system [20], thereby increasing the risk of endangering coronary anastomosis patency [21]. Despite the strong theoretical possibility of a close relationship between reduced heparin responsiveness and postoperative MI in patients undergoing OPCAB [9], no association between low intraoperative HSI value and adverse ischemic outcomes was observed in this study. The etiology of postoperative MI is multifactorial. In addition to the hypercoagulable state, surgical techniques are also considered significant contributing factors. The present study involved ten experienced faculty surgeons who had completed at least 100 OPCAB procedures as part of their institutional requirement before being qualified to perform the procedure [22]. Therefore, the quality of surgery in this study was deemed reliable.
The present study also confirmed the correlation between preoperative high PLT count and low intraoperative HSI value [12, 13, 23]. The reduced responsiveness to UFH was attributed to excessive production of platelet factor 4 (PF4), an anti-heparin agent, resulting from the accelerated rate of PLT destruction. The strong binding affinity of PF4 for UFH leads to the displacement of PF4 from vascular binding sites with lower affinity, resulting in the formation of circulating complexes with UFH that neutralize its effect. Therefore, one possible explanation for low intraoperative HSI value in patients with preoperative high PLT count may be their greater capacity to produce PF4 after PLT activation [12]. Additionally, PLT count was associated with ACT value [13, 23], which are currently regarded as the standard parameter for monitoring the anticoagulant effect of UFH. The measurement of ACT is a test of whole-blood coagulation that involves the interaction between plasma coagulation components and PLT phospholipids in the hemostatic process. Therefore, a high PLT count may shorten the ACT response time.
In this study, preoperative LMWH treatment was not associated with the incidence of low intraoperative HSI value. Some studies have demonstrated improved outcomes with LMWH use in patients with unstable angina [6]. Therefore, all patients presenting for OPCAB received LMWH before surgery. The dose of enoxaparin was 6000 IU, administered subcutaneously every 12 h. Preoperative heparin exposure was equivalent between the two groups.
Preoperative administration of antiplatelet agents, such as aspirin and clopidogrel, has been linked to an increased risk of blood loss after cardiac surgery [11, 24]. According to the European guidelines [25], for clopidogrel, from the perspective of reducing the blood loss risk, elective cardiac surgery should be performed five days after stopping clopidogrel. The European guidelines also recommend that patients at low risk of perioperative blood loss should continue taking aspirin and do not need to stop taking aspirin before surgery. However, one study indicated that the preoperative use of aspirin significantly increases the risk of postoperative blood loss and blood transfusion in patients undergoing OPCAB [11], and recommended discontinuing aspirin intake six days prior to surgery. In this study, preoperative use of clopidogrel or aspirin was not included in the multivariate logistic regression model because of the limited number of available events. Further research is necessary to investigate whether clopidogrel or aspirin increases the risk of postoperative blood loss during OPCAB.
Limitations of the study include the following. First, this study had a retrospective design. The results of the current study rely heavily on the comprehensiveness and accuracy of the original documentation. We endeavored to minimize potential inaccuracies by meticulously reviewing patients’ medical records. Secondly, HSI was used as a criterion to indicate heparin responsiveness, with some studies using a threshold value of 1.3 and others using 1.0. A stringent criterion for low intraoperative HSI value was defined as an HSI value less than 1.0, which showed an incidence rate between 15.5% [26] and 20.8% [2]. Despite the low incidence of low intraoperative HSI value as measured by this stringent criteria, future studies involving large samples should pay greater attention to this issue.
Conclusions
The present study demonstrated that intraoperative HSI was not associated with postoperative blood loss in Chinese patients undergoing elective OPCAB. Preoperative high PLT count was an independent predictor of low intraoperative HSI value.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bull MH Huse WM Bull BS Evaluation of tests used to monitor heparin therapy during extracorporeal circulation Anesthesiology 197543334635310.1097/00000542-197509000-000121163834 · doi ↗ · pubmed ↗
- 2Chun DH Baik SW Kim SY Shim JK Kim JC Kwak YL Heparin responsiveness during off-pump coronary artery bypass graft surgery: predictors and clinical implications Acta Pharmacol Sin 201132113313810.1038/aps.2010.18021131997 PMC 4003313 · doi ↗ · pubmed ↗
- 3Finley A Greenberg C Review article: heparin sensitivity and resistance: management during cardiopulmonary bypass Anesth Analg 201311661210122210.1213/ANE.0b 013e 31827 e 4e 6223408671 · doi ↗ · pubmed ↗
- 4Knapik P Cieśla D Przybylski R Knapik T The influence of heparin resistance on postoperative complications in patients undergoing coronary surgery Med Sci Monit.2012182 CR 1051110.12659/MSM.88246522293873 PMC 3560574 · doi ↗ · pubmed ↗
- 5Dietrich W Spannagl M Schramm W Vogt W Barankay A Richter JA The influence of preoperative anticoagulation on heparin response during cardiopulmonary bypass J Thorac Cardiovasc Surg 1991102450551410.1016/S 0022-5223(20)31420-31833592 · doi ↗ · pubmed ↗
- 6Bar-Yosef S Cozart HB Phillips-Bute B Mathew JP Grocott HP Preoperative low molecular weight heparin reduces heparin responsiveness during cardiac surgery Can J Anaesth 200754210711310.1007/BF 0302200617272249 · doi ↗ · pubmed ↗
- 7Ranucci M Frigiola A Menicanti L Cazzaniga A Soro G IsgròG Risk factors for fatal myocardial infarction after coronary bypass graft surgery Eur J Anaesthesiol 200118532232910.1097/00003643-200105000-0000711350475 · doi ↗ · pubmed ↗
- 8Ma HP Xu WF Yu J Wang J Zheng H Heparin sensitivity and postoperative blood loss in patients undergoing cardiac surgery with cardiopulmonary bypass Eur J Anaesthesiol 202037316216910.1097/EJA.000000000000114831895135 · doi ↗ · pubmed ↗