Complex Traumatic Jejunal Perforation With Mesenteric Tear and Intussusception: A Case Report
Khushbu Vaidya, Pankaj Gharde, Raju K Shinde, Mihir Patil, Somya Goel

TL;DR
A 52-year-old man suffered complex abdominal injuries from a collision, requiring emergency surgery to repair a perforated intestine and related trauma.
Contribution
This case report presents a rare combination of jejunal perforation, mesenteric tear, and intussusception following blunt trauma.
Findings
Blunt trauma caused jejunal perforation, mesenteric tear, and intussusception.
Emergency surgery with bowel resection was required to treat the injuries.
Histopathology confirmed traumatic perforation with acute inflammation.
Abstract
Blunt abdominal trauma can result in a spectrum of injuries, ranging from superficial contusions to severe hollow viscus perforations. We present the case of a 52-year-old male involved in a bicycle-truck collision, leading to complex intra-abdominal injuries. The patient presented with acute abdominal pain and signs of peritonitis, prompting urgent diagnostic workup and surgical intervention. Imaging studies revealed pneumoperitoneum, free fluid, and multiple rib fractures indicative of significant trauma. Exploratory laparotomy unveiled a perforated jejunal loop with an associated mesenteric tear and intussusception, necessitating segmental bowel resection and repair. Histopathological analysis confirmed acute hemorrhagic inflammation consistent with traumatic perforation. This case highlights the challenges and complexities associated with blunt abdominal trauma, emphasizing the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
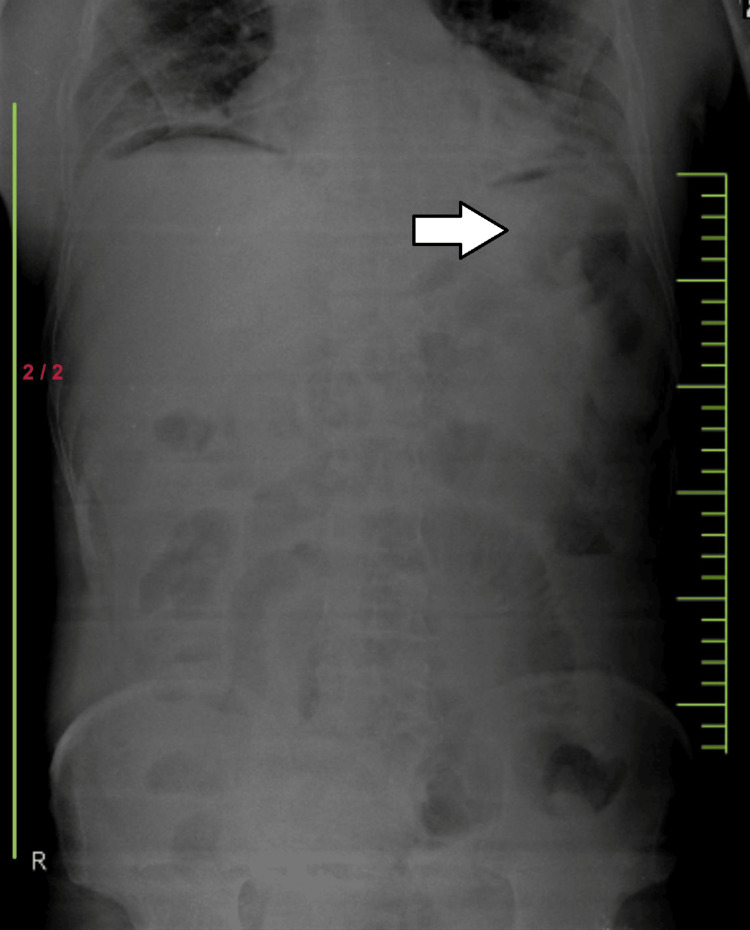 Figure 1
Figure 1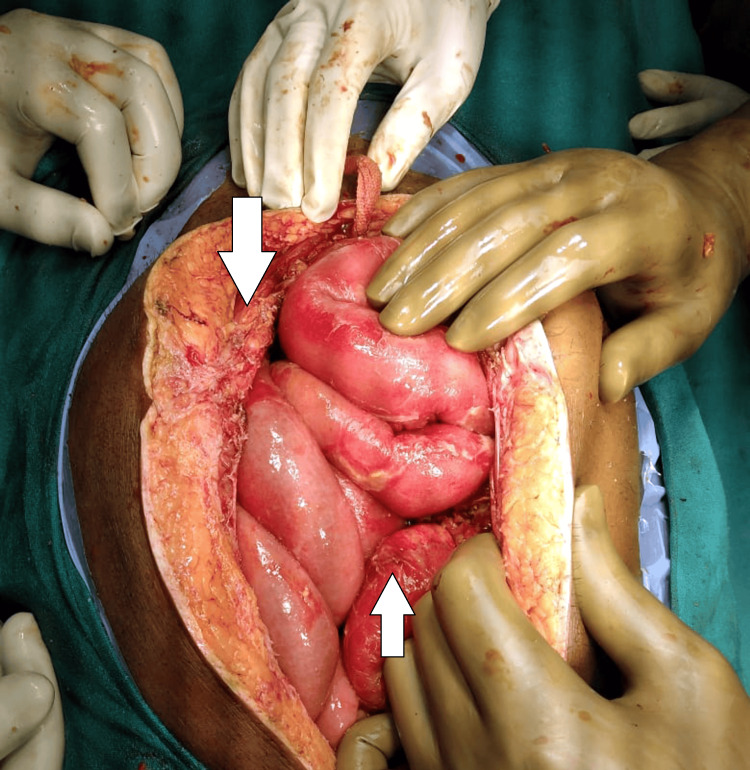 Figure 2
Figure 2 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal disorders and treatments · Esophageal and GI Pathology · Congenital Diaphragmatic Hernia Studies
Introduction
Blunt abdominal trauma is a critical condition that often poses significant diagnostic and management challenges and is frequently encountered in patients involved in traffic accidents, falls, or assaults. The abdomen, being less protected than other body parts, is particularly susceptible to injury from blunt force. Such trauma can lead to various injuries, including solid organ injury (liver, spleen, kidneys), hollow viscus injury (small and large bowel, bladder), and vascular injury [1]. Hollow viscus injuries (HVI) are among the most challenging consequences of blunt abdominal trauma to diagnose, primarily due to their non-specific clinical and imaging findings. They are identified in approximately 1-5% of blunt abdominal traumas [2]. The Centers for Disease Control and Prevention (CDC) states that HIV tests have 99.6% specificity, which means that for every 1,000 people without HIV who take the test, 996 will receive true negative results, and four may receive a false positive [2-3]. The most commonly injured parts of the gastrointestinal tract in blunt trauma are the small intestine, colon, and duodenum [3]. The diagnostic difficulty arises because initial symptoms and signs may be subtle or absent, and delays in diagnosis can lead to significant morbidity and mortality due to sepsis and peritonitis [4].
Perforation of the small intestine, as seen in our case, is particularly concerning as it is associated with high infection rates and requires prompt surgical intervention. Clinical assessment remains crucial, including careful monitoring of vital signs and physical examination findings [5]. Moreover, mesenteric tears, which may accompany small bowel perforations, add another layer of complexity. They can lead to compromised blood supply and result in bowel ischemia or infarction if not promptly addressed [6]. Intussusception in adults, although rare, can occur as a consequence of trauma and may present with similar radiologic features to other types of bowel injury [7].
Case presentation
A 52-year-old male was admitted to the emergency department following a collision between his bicycle and a truck, which resulted in direct impact trauma from the bicycle handle to his chest and abdomen. Upon presentation, the patient complained of severe, diffuse abdominal pain without any prior history of significant medical issues, head injuries, or episodes of unconsciousness. His initial vital signs just after the admission to the emergency department indicated a tachycardic state with a pulse of 130 bpm, hypotension at 104/60 mmHg, and oxygen saturation at 96% on 3 L/min supplemental oxygen. Physical examination revealed abdominal distension, tenderness, and guarding suggestive of an acute abdominal crisis.
Initial diagnostic investigations included an abdominal X-ray, which showed signs consistent with pneumoperitoneum, indicating a possible hollow viscus perforation as shown in Figure 1. An abdomen ultrasound identified free fluid consistent with ascites in perihepatic and perisplenic regions. A CT scan of the abdomen and pelvis was performed to further evaluate the extent of injuries, revealing small pockets of air in the preduodenal and periportal regions and moderate free fluid. These findings highly suggest a hollow viscus injury involving the small bowel. A chest CT scan was also conducted due to the nature of the trauma, which revealed pneumothorax, subcutaneous emphysema, and multiple rib fractures from the right fifth to eighth ribs.
Signs consistent with pneumoperitoneum
Given the clinical and radiological evidence of intra-abdominal injury, the patient was urgently taken to the operating room for an exploratory laparotomy. During surgery, a perforated jejunal loop with a mesenteric tear was discovered as shown in Figure 2.
Perforated jejunal loop with a mesenteric tear
Additionally, a segment of the small bowel was found intussuscepting through the perforation site, complicating the injury pattern. Segmental jejunal resection was performed with primary anastomosis. The colon serosa that had been damaged was repaired via suturing, and a necrotic section of the colon necessitated partial colectomy. Adjacent to the primary lesion in the small bowel mesentery, a benign hematoma was evacuated as shown in Figure 3.
Evacuated hematoma
Histopathological examination of the resected bowel segments confirmed acute hemorrhagic inflammation consistent with traumatic perforation. The complex nature of the patient’s injuries required multidisciplinary management, including surgical intervention, intensive postoperative care, and nutritional support to address the immediate and secondary complications of such severe trauma. This case highlights the critical nature of rapid assessment and intervention in patients presenting with blunt abdominal trauma, the complexity of injuries that can occur, and the importance of a thorough and multidisciplinary approach to management to optimize patient outcomes.
Discussion
The presented case exemplifies the complexity and severity of intra-abdominal injuries resulting from blunt trauma, necessitating prompt recognition and multidisciplinary management. Blunt abdominal trauma encompasses a broad spectrum of injuries, ranging from mild contusions to life-threatening hollow viscus perforations, as seen in this patient [8]. The occurrence of both bowel perforation and mesenteric tear, complicated further by bowel intussusception, represents a rare and challenging scenario in trauma care [9]. A lead point is found in around 80-90% of cases, even though the annual incidence of adult intussusception is very low [9]. While solid organ injuries often dominate discussions on blunt abdominal trauma, hollow viscus injuries, particularly involving the small bowel, present unique diagnostic and therapeutic challenges due to their nonspecific clinical manifestations and subtle radiological findings [9].
Diagnostic modalities such as abdominal X-ray, ultrasound, and computed tomography are crucial in assessing patients with suspected hollow viscus injuries. In this case, the presence of pneumoperitoneum on X-ray and free fluid on ultrasound and CT scan aided in identifying the extent and severity of intra-abdominal injuries, prompting the need for urgent surgical intervention. [10]. Surgical exploration remains the gold standard for definitive diagnosis and management of hollow viscus injuries. The intraoperative findings of a perforated jejunal loop with associated mesenteric tear and bowel intussusception underscore the complexity of the patient's injuries, necessitating segmental bowel resection, serosal repair, and partial colectomy [11].
Histopathological examination of the resected bowel segments confirmed acute hemorrhagic inflammation consistent with traumatic perforation, highlighting the importance of corroborating clinical and radiological findings with histological evidence to guide patient management and prognosis [12]. This case emphasizes the critical role of prompt recognition and multidisciplinary management in optimizing outcomes for patients with blunt abdominal trauma. A comprehensive approach involving trauma surgeons, radiologists, anesthesiologists, and intensive care specialists is essential to address the varied and often life-threatening consequences of intra-abdominal injuries [13].
Conclusions
In conclusion, the presented case underscores the intricate nature of intra-abdominal injuries secondary to blunt trauma, exemplified by the rare occurrence of perforated bowel with mesenteric tear and intussusception. Through prompt recognition, accurate diagnosis, and multidisciplinary management, favorable outcomes were achieved for the patient despite the complexity of his injuries. This case highlights the critical role of surgical intervention guided by advanced imaging modalities and histopathological confirmation in optimizing patient outcomes. Moving forward, continued emphasis on comprehensive trauma care protocols and interdisciplinary collaboration is paramount to effectively address the varied and often life-threatening consequences of blunt abdominal trauma, ensuring timely and appropriate management for patients presenting with similar challenging injuries.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Trends in nonoperative management of traumatic injuries - a synopsis Int J Crit Illn Inj Sci Stawicki SP 3857720172838225810.4103/IJCIIS.IJCIIS_7_17PMC 5364768 · doi ↗ · pubmed ↗
- 2Hollow viscus injury due to blunt trauma: a review J Visc Surg Bège T Brunet C Berdah SV 616815320162720907810.1016/j.jviscsurg.2016.04.007 · doi ↗ · pubmed ↗
- 3Management of bleeding following major trauma: an updated European guideline Crit Care Rossaint R Bouillon B Cerny V 014201010.1186/cc 8943 PMC 288716820370902 · doi ↗ · pubmed ↗
- 4Emergency thoracotomy in trauma: rationale, risks, and realities Scand J Surg Søreide K Petrone P Asensio JA 4109620071746130510.1177/145749690709600102 · doi ↗ · pubmed ↗
- 5WSES guidelines on blunt and penetrating bowel injury: diagnosis, investigations, and treatment World J Emerg Surg Smyth L Bendinelli C Lee N 131720223524619010.1186/s 13017-022-00418-y PMC 8896237 · doi ↗ · pubmed ↗
- 6Acute mesenteric ischemia: a challenge for the acute care surgeon Scand J Surg Kärkkäinen JM 15015811020213386689110.1177/14574969211007590 PMC 8258713 · doi ↗ · pubmed ↗
- 7Adult intussusception Perm J Lu T Chng YM 798119201510.7812/TPP/14-125PMC 431538425663210 · doi ↗ · pubmed ↗
- 8Nonoperative management of blunt hepatic injury: an Eastern Association for the Surgery of Trauma practice management guideline J Trauma Acute Care Surg Stassen NA Bhullar I Cheng JD 09373201210.1097/TA.0b 013e 318270160 d 23114483 · doi ↗ · pubmed ↗