Segmentectomy for ground glass-dominant invasive lung cancer with tumour diameter of 2–3 cm: protocol for a single-arm, multicentre, phase III trial (ECTOP1012)
Shiqi Chen, Qingyuan Huang, Fangqiu Fu, Zezhou Wang, Yang Zhang, Haiquan Chen

TL;DR
This study tests if segmentectomy is a safe and effective treatment for a specific type of lung cancer with tumors measuring 2–3 cm.
Contribution
The trial introduces a new clinical investigation into the optimal surgical approach for ground glass-dominant lung cancer of a specific size range.
Findings
The trial aims to determine if segmentectomy is suitable for ground glass-dominant invasive LUAD with tumor size of 2–3 cm.
It will evaluate 5-year disease-free survival and other clinical outcomes in 307 patients across multiple hospitals.
Abstract
Previous studies demonstrated that wedge resection is sufficient for ground glass-dominant lung adenocarcinoma (LUAD) with tumour diameter ≤2 cm, however, the optimal surgical type for ground glass-dominant LUAD with tumour diameter of 2–3 cm remains unclear. The purpose of this trial is to investigate the safety and efficacy of segmentectomy for ground glass-dominant invasive LUAD with tumour size of 2–3 cm. We initiated a phase III trial to investigate whether segmentectomy is suitable for ground glass-dominant invasive LUAD with tumour size of 2–3 cm. This trial plans to enrol 307 patients from multiple institutions including four general hospitals and two specialty cancer hospitals over a period of 5 years. The primary endpoint is 5 year disease-free survival. Secondary endpoints are lung function, 5 year overall survival, the site of tumour recurrence and metastasis, segmentectomy…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
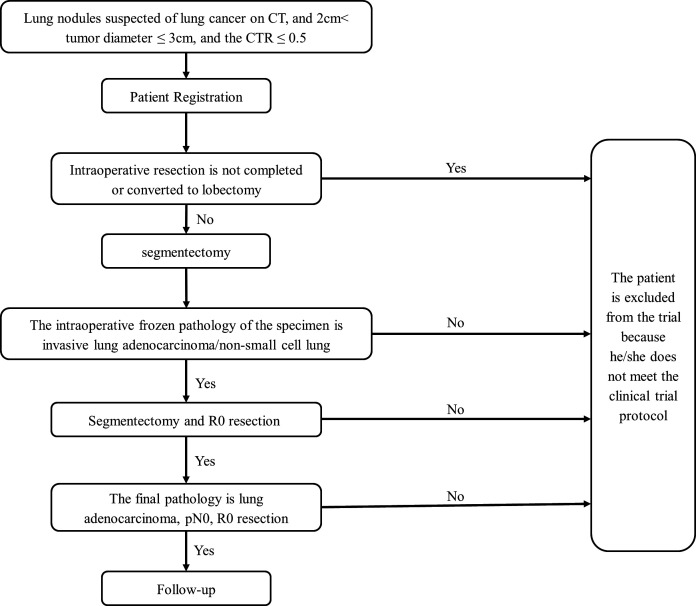 Figure 1
Figure 1- —Cooperation Project of Conquering Major Diseases in Xuhui District
- —National Key R&D Program of China
- —Shanghai Technology Innovation Action Project
- —http://dx.doi.org/10.13039/501100001809National Natural Science Foundation of China
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Diagnosis and Treatment · Lung Cancer Treatments and Mutations · Radiomics and Machine Learning in Medical Imaging
Introduction
Lung cancer is the most commonly diagnosed malignancy in men and the leading cause of cancer-associated mortality in both men and women.1 Since the national lung screening trial demonstrated that screening with low-dose CT (LDCT) could increase the detection of lung cancer, and reduce the risk of mortality from lung cancer, LDCT is widely used in the screening for lung cancer.2 LDCT screening leads to a dramatic increase in the detection of small-sized lung nodules, especially ground-glass opacity (GGO).3 The shift of the spectrum of radiological characteristics challenges lobectomy as the ‘gold standard’ of surgical treatment for early-stage lung cancer, which was established in the 1990s by the Lung Cancer Study Group trial.4
From 2002 to 2004, the JCOG0201 trial included patients with clinical T1N0M0 (≤3 cm in tumour diameter) peripheral lung cancer, and defined radiological non-invasive lung adenocarcinoma (LUAD) as tumour size ≤2 cm with consolidation-to-tumour ratio (CTR) ≤0.25.5 Afterward, the JCOG1211 trial found that the 5 year recurrence-free survival (RFS) of patients undergoing segmentectomy for the ‘radiologically invasive’ tumours (tumour diameter ≤2 cm with CTR between 0.25 and 0.50, or tumour diameter between 2 cm and 3 cm with CTR≤0.50) is 98.0%, exceeding the 87% of the preset threshold.6 However, this trial was criticised on the basis that about half of the included patients were pathologically confirmed as adenocarcinoma in situ (AIS) and microinvasive adenocarcinoma (MIA). For these patients (AIS/MIA), wedge resection is sufficient, and segmentectomy may be unnecessary. Additionally, this also limits the statistical power to demonstrate the efficacy of pathologically invasive LUAD. Recently, our team performed a retrospective study and found that wedge resection for peripheral invasive LUAD with tumour diameter ≤2 cm and CTR≤0.5 could lead to excellent long-term survival.7
This single-arm, multicentre, phase III trial (ECTOP1012) aims to investigate whether segmentectomy is suitable for ground glass-dominant invasive lung cancer with tumour size of 2–3 cm.
Methods and analysis
Study design
ECTOP1012 is a single-arm, multicentre, confirmatory phase III trial to evaluate the safety and efficacy of segmentectomy for ground glass-dominant invasive lung cancer with size of 2–3 cm. Four general hospitals and two specialty cancer hospitals will participate in this trial. As the prognosis of these patients is fairly excellent, a large sample size would be required if a randomised controlled trial (RCT) is to be performed, so this study is designed as a single-arm confirmatory trial. The tumour size should be between 2 and 3 cm, and the CTR should not be greater than 0.5 on preoperative high-resolution CT. The surgical procedure for included patients is segmentectomy, which includes single-segment resection, combined segment resection, trisegmentectomy and basal segment resection. Tumours located in the right middle lobe are excluded in this trial (figure 1).
Study flowchart. CTR, consolidation-to-tumour ratio.
The trial started in February 2023; the estimated primary completion date is December 2028 and the estimated study completion date is December 2029. We used the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) checklist when preparing this report.8
Objectives
The primary objective of ECTOP1012 is to assess the efficacy of segmentectomy for ground glass-dominant invasive lung cancer with size of 2–3 cm.
The secondary objectives include:
Surgical safety of segmentectomy for ground glass-dominant invasive lung cancer with size of 2–3 cm.Loss of lung function after segmentectomy.Tumour recurrence rate after segmentectomy.
Endpoints
The primary endpoint is 5 year disease-free survival (5 year DFS). DFS events are defined as tumour recurrence due to lung cancer or death from any cause. Alive patients without recurrence at the last follow-up are defined as censored.
The secondary endpoints are lung function, 5 year overall survival, the site of tumour recurrence and metastasis, segmentectomy completion rate, radical segmentectomy (R0 resection) completion rate and surgery-related complications.
Eligibility criteria
Inclusion criteria
All enrolled patients should meet the following criteria:
Written informed consent.18–80 years old (including cut-off value) at the time of signing the informed consent.Eastern Cooperative Oncology Group (ECOG) score of 0 or 1.No prior lung cancer surgery.Invasive LUAD confirmed by intraoperative or postoperative pathological evaluation.A single pulmonary nodule with a predominantly ground-glass component or pure ground-glass on CT, or multiple pulmonary nodules but the main lesion is the above-mentioned nodule.The CTR of the nodule ranges from 0 to 0.5, and the total size is between 2 and 3 cm.No evidence of nodal or distant metastasis.The tumour is evaluated to be completely removed via segmentectomy by thoracic surgeon.No prior radiotherapy or chemotherapy.
Exclusion criteria
Exclusion criteria
Patients are excluded if they meet any of the following criteria:
1.CTR is not between 0 and 0.5 or the total nodule size is not between 2 and 3 cm.
2.The lesion cannot be completely surgically removed by segmentectomy.3.Lung malignancies other than lung adenocarcinoma confirmed by cytological or histopathological evaluation.4.Prior lung cancer surgery.5.Non-treatment-naïve patients.
Withdrawal or termination criteria
All data in this trial are obtained based on existing examinations and procedures and the trial does not cause any additional harm to patients. The specifics of the patient’s withdrawal from this study are as follows:
The patient’s data shall not be used for the clinical study.Patient enrolment error (eg, patient does not meet enrolment criteria).Patients voluntarily propose to withdraw from the trial.
Treatment
Segmentectomy and lymph node dissection
Pulmonary GGOs that are evaluated to be removed via segmentectomy by thoracic surgeons could be included in the study. Anatomical segmentectomy could be single segmentectomy (eg, S3 resection), combined segmentectomy (eg, S7+S8 resection), basal segmentectomy (eg, S7–S10 resection) and trisegmentectomy (eg, left S1–S3 resection). In addition, the use of wedge resection to manage the patient’s other non-major lesions is allowed in this study.
Based on the results of previous studies, there was no lymph node metastasis in lung cancer with a CTR<0.5,9 so there is no further provision for mediastinal lymph node dissection in this study, and the surgeon could choose the extent of mediastinal lymph node dissection according to personal experience. The lymph nodes exposed during the operation need to be removed and sent for pathological examination.
Procedures
Preoperative CT imaging evaluation and clinical staging
All patients are required to undergo a thin-slice (1 mm) contrast-enhanced CT scan of the chest before enrolment. According to the CT scan results, the long diameter of the tumour is the maximum diameter of the tumour (solid component+ground-glass component) on the CT cross-section. The size of the solid component is the maximum diameter of the solid component on the CT cross-section. CTR is defined as the ratio of solid component size to tumour diameter. For pure ground-glass nodules in which there are no solid components, the CTR is 0. cN0 is diagnosed when the short axis of lymph nodes of intrapulmonary, interlobar, hilar and mediastinal are shorter than 10 mm on contrast-enhanced CT or no uptake of lymph nodes on PET/CT.10 The staging in this study is performed using the 8th edition of the TNM lung cancer staging system.11 Patients will be admitted to the hospital for surgery after the CT or PET-CT is evaluated by the radiologist, and the interval is 1 month.
Intraoperative frozen pathological evaluation criteria
All primary tumours are sent to the pathology room for frozen section diagnosis immediately after resection. Frozen pathology is taken from the maximum diameter of the tumour. Diagnosis is based on the 2015 WHO classification criteria.12 Lesions diagnosed as invasive lung adenocarcinoma/non-small cell lung cancer by intraoperative frozen are included in this study.
Postoperative pathological evaluation criteria
The postoperative pathological diagnosis of the tumour using paraffin sections is based on the 2015 version of the WHO classification criteria, and patients with lung adenocarcinoma are included in this study. All pathology reports are evaluated by two experienced pathologists.
Statistical analysis
Analysis sets
Full analysis set (FAS): determined according to the intention-to-treat principle, including all enrolled cases who have undergone segmentectomy.
Per-protocol set (PPS): subset of the FAS population, including all cases that meet the protocol and have completed case report form.
In this trial, FAS analysis is used for baseline data and validity analysis. The main efficacy indicators are will be analysed in the FAS and PPS data sets. However, the analyses of the FAS data set are considered primary. When analyses of the FAS and PPS reach consistent conclusions, confidence in the conclusions can be increased. For the FAS data set, the missing data after the fall are estimated using the last observation carried forward method.
The laboratory examination data and adverse events will be analysed using SPSS and Stata software.
Calculation of sample size
According to the results of previous studies, for patients undergoing lobectomy with tumour sizes of 2–3 cm, CTR≤0.5 and the 5 year DFS was 97.0% after surgery.13 In this trial, we assumed that the expected 5 year DFS for these patients undergoing segmentectomy is 95%. A sample size of 292 achieves 90.193% power to detect a non-inferiority proportion of 90% (5% as the non-inferior boundary) using a one-sided exact test with a target significance level of 0.0250. Considering a possible dropout rate of 5%, a total of 307 cases need to be included in this trial.
Data access
The Data Management Coordinating Centre will oversee the intrastudy data- sharing process, with input from the Data Management Subcommittee. All Principal Investigators will be given access to the cleaned data sets. Project data sets will be housed on the Project Accept website and/or the file transfer protocol site created for the study, and all data sets will be password-protected. Project Principal Investigators will have direct access to their own site’s data sets and will have access to other sites’ data by request. To ensure confidentiality, data dispersed to project team members will be blinded to any identifying participant information.
Patient and public involvement
None.
Ethics and dissemination
The protocol and informed consent form have been reviewed and approved by the Ethics Committee of Fudan University Shanghai Cancer Centre (reference 2212267-18) and by the institutional review boards of each participating centre. Only patients who can fully understand the risks, benefits and potential adverse events of this trial will be enrolled after voluntarily signing an informed consent form (online supplemental Material 1). Informed consent should be in line with the Declaration of Helsinki.
10.1136/bmjopen-2024-087088.supp1Supplementary data
The personal data collected and processed by the patients enrolled in this study will be limited to those necessary to complete the purposes of this study.
The results of the trial will be updated on ClinicalTrials.gov, published in peer-reviewed journals and presented at international academic conferences.
Supplementary Material
Reviewer comments
Author's manuscript
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Siegel RL , Miller KD , Fuchs HE , et al . Cancer statistics, 2022. CA A Cancer J Clinicians 2022;72:7–33. 10.3322/caac.21708 35020204 · doi ↗ · pubmed ↗
- 2Aberle DR , Berg CD , Black WC , et al . The National lung screening trial: overview and study design. Radiology 2011;258:243–53. 10.1148/radiol.10091808 21045183 PMC 3009383 · doi ↗ · pubmed ↗
- 3Li N , Tan F , Chen W , et al . One-off low-dose CT for lung cancer screening in China: a multicentre, population-based, prospective cohort study. Lancet Respir Med 2022;10:378–91. 10.1016/S 2213-2600(22)00047-9 35276087 · doi ↗ · pubmed ↗
- 4Ginsberg RJ , Rubinstein L . The comparison of limited resection to lobectomy for T 1N 0 non-small cell lung cancer. LCSG 821. Chest 1994;106:318S–319S. 10.1378/chest.106.6_Supplement.318S 7988253 · doi ↗ · pubmed ↗
- 5Suzuki K , Koike T , Asakawa T , et al . A prospective radiological study of thin-section computed tomography to predict pathological noninvasiveness in peripheral clinical IA lung cancer (Japan clinical oncology group 0201). J Thorac Oncol 2011;6:751–6. 10.1097/JTO.0b 013e 31821038 ab 21325976 · doi ↗ · pubmed ↗
- 6Aokage K , Suzuki K , Saji H , et al . Segmentectomy for ground-glass-dominant lung cancer with a tumour diameter of 3 cm or less including ground-glass opacity (JCOG 1211): a multicentre, single-arm, confirmatory, phase 3 trial. Lancet Respir Med 2023;11:540–9. 10.1016/S 2213-2600(23)00041-3 36893780 · doi ↗ · pubmed ↗
- 7Zhang C , Pan Y , Li H , et al . Extent of surgical resection for radiologically subsolid T 1N 0 invasive lung adenocarcinoma: when is a wedge resection acceptable. J Thorac Cardiovasc Surg 2024;167:797–809. 10.1016/j.jtcvs.2023.06.010 37385528 · doi ↗ · pubmed ↗
- 8Chan A-W , Tetzlaff JM , Gotzsche PC , et al . SPIRIT 2013 explanation and elaboration: guidance for protocols of clinical trials. BMJ 2013;346:e 7586. 10.1136/bmj.e 7586 23303884 PMC 3541470 · doi ↗ · pubmed ↗