A transversal cross-sectional study of factors related to HPV vaccination status and cancer screening participation among French women aged 25–40
Fanny Serman, Gabrielle Lisembard, Maxence Sahraoui, Christophe Berkhout, Michaël Rochoy, Anthony Haro, Matthieu Calafiore

TL;DR
This study examines HPV vaccination and cervical cancer screening participation among French women aged 25–40, identifying factors like medical information and gynecological follow-up as key influences.
Contribution
The study identifies specific risk factors for non-vaccination and non-screening, emphasizing the role of medical information and regular gynecological follow-up.
Findings
41% of women aged 25–40 in the Nord-Pas-de-Calais region were vaccinated against HPV in 2022.
Non-vaccination was strongly associated with eligibility periods in the early days of French vaccination and lack of medical information.
90% of women were screened for uterine cervical cancer, with lack of regular gynecological follow-up being the only consistent risk factor for non-screening.
Abstract
In 2020, uterine cervical cancer (UCC) was the 12th most common cancer among women in France and the 4th worldwide. French health authorities wanted to increase Human Papilloma Virus (HPV) vaccination and screening rates. There were still many barriers to these measures among young women, their families, and health professionals and teachers. Between 2014 and 2019, international studies found inconsistent effects of HPV vaccination on UCC screening. In 2022, a survey was conducted among women aged 25 to 40 in the Nord-Pas-de-Calais region to assess participation 1) in HPV vaccination and its barriers, 2) in UCC screening as a function of HPV vaccination status. Data were collected using an anonymous online questionnaire distributed by QR code in 80 general practices randomly selected in the Nord-Pas-de-Calais region between January and June 2022. Results were analyzed bivariately using…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
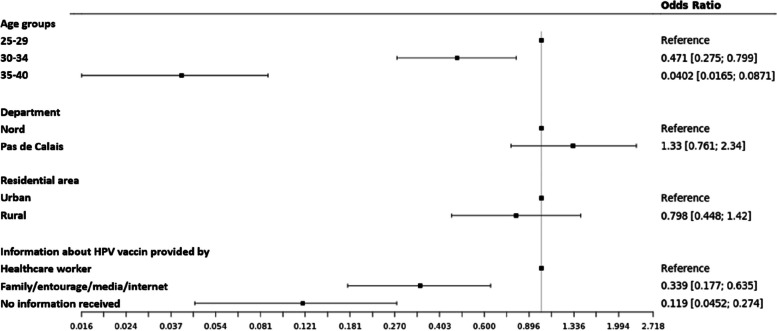 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCervical Cancer and HPV Research · Hepatitis B Virus Studies · Genital Health and Disease
Background
In 2020, uterine cervical cancer (UCC) will be the twelfth most common cancer among women in France and the fourth most common cancer worldwide [1], making it a major public health concern. Incidence and mortality rates for UCC have declined steadily in France since the introduction of cervical screening by cervical cytology (Pap smear) in the 1960s [2]. However, this decline has slowed, probably due to increased exposure to high-risk human papillomaviruses (HPV-HR) associated with changes in sexual behavior, such as a decrease in the age of sexual debut and an increase in the number of sexual partners [3, 4]. By 2020, 90% of new cases and deaths will occur in developing countries [1]. According to the World Health Organization (WHO), by 2022, UCC will be considered a preventable and eliminable cancer through preventive measures. These measures, vaccination, and cervical cytology screening, were more accessible in developed countries. The World Health Assembly adopted a strategy to eliminate UCC as a public health problem and set the "90–70-90" targets. By 2030, this would mean that 90% of girls should be fully vaccinated by age 15, 70% of women should be screened at ages 35 and 45, and 90% of women diagnosed with cervical disease (precancerous lesions or invasive cancer) should receive treatment [5].
In France, the history of HPV vaccination is complex. It started in 2007 targeting 14-year-old girls, with catch-up vaccination for women aged 15 to 25. In 2012, it was extended to girls aged 11 to 14, with catch-up for those aged 15 to 19. In 2019, vaccination was recommended for men under 26 who have sex with men. Since 2021, it is recommended for all genders aged 11 to 19. Cervical cancer screening in France was done by cytological examination of a cervical smear every three years for women aged 25 to 65 until 2019. The widespread adoption of HPV molecular detection changed this in 2019 for women aged 30 to 65, shifting to HPV testing on cervical smears every five years (remaining unchanged for those aged 25 to 30). Despite the availability of these two complementary preventive measures, vaccination coverage and screening rates remained insufficient. Acceptance and adherence to HPV vaccination have been described as a complex concept involving users, parents, and professionals, which is improved by talking about the vaccine and about sexuality [6]. In Italy in 2022, HPV vaccination coverage was clearly inadequate, as was adherence to screening, both far from WHO targets [7]. Studies have identified perceived barriers to vaccination among the student population[8] as well as among health care workers and teachers[9], including mistrust of the vaccine due to its perceived novelty, low knowledge, and misinformation about the vaccine. A Chinese study found in 2015 that educational intervention on HPV increased awareness regarding HPV and women’s intention to vaccinate themselves[10]. Several studies, including one from Belgium and one from France, have shown that young girls who are vaccinated are more likely to have a mother who is regularly screened. Preventive behaviors tend to cluster within families [11, 12]. Our first objective was to describe the HPV vaccination prevalence in the Nord-Pas-de-Calais departments in France and to assess potential risk factors for non-vaccination.
The second concern that could arise is participation in UCC screening, especially among vaccinated women, since even general practitioners in France in 2020 feared that vaccination would reduce participation in screening [13]. In Denmark and the United Kingdom, vaccinated women would be more likely to undergo screening [14, 15]. In a French study conducted in 2011 among women aged 25–65, 66.7% of respondents believed that vaccinated women should continue to undergo cervical screening by Pap smear, while 29.1% said they did not know. However, this study did not consider vaccination status [16]. Internationally, several studies have attempted to examine the association between HPV vaccination status and screening uptake. Most of these studies were conducted in Australia or Japan, where organized screening programs have been in place for several years, and in the United States. They showed statistically significant higher screening rates among vaccinated women compared with unvaccinated women [17–19]. European studies have also found similar results, including in Sweden and Italy [20, 21]. Only an Australian study from 2014 showed a statistically significant lower screening rate among vaccinated women [22]. To our knowledge, there have been no other studies in France, and particularly in Nord-Pas-de-Calais, where cervical cancer screening rates were barely 60%, on screening participation based on vaccination status in 2022. The primary objective was to determine if there was a significant association between HPV vaccination status and cervical cancer screening among eligible women in Nord-Pas-de-Calais.
The secondary objectives were to determine the sociodemographic and medical characteristics, the modalities of use of vaccination and screening, and the knowledge of these two means of prevention among the responding women according to their HPV vaccination status.
Methods
Design
The epidemiologic study was a retrospective analytical observational study conducted between February 1 and June 1, 2022. It was a multicenter study conducted in the Nord-Pas-de-Calais region (France) using an online self-administered questionnaire targeting women aged 25–40 years. The questionnaire was made accessible through a QR code placed in the waiting rooms of randomly selected general practitioners' offices.
Population
The study population consisted of French women aged 25–40 years who visited randomly selected general practitioners in Nord and Pas-de-Calais and completed the questionnaire. Exclusion criteria were: women under 25 or over 40 years of age, incomplete questionnaires, women who did not know their HPV vaccination status, women who did not know their cervical cancer screening status. We excluded women above 40 in 2022 as they had not had access to the vaccination (the French vaccination program began in 2007 for young women aged 9–25 years), and women under 25 since they were not targeted by the screening program. The minimum number of analyzable questionnaires required to achieve adequate power was 385.
GP’s were chosen for their centrality in the primary care network to ensure a broad and representative sample that was homogeneously distributed and practically feasible without additional resources. The authors' experience was that about 15% of their colleagues agreed to participate in clinical studies by displaying a survey request in their waiting room, resulting in 5 to 10 responses over a period of 3 months: a random sample of 400 GPs was selected from the exhaustive list of 3,780 general practitioners (GPs) in Nord and Pas-de-Calais. These GPs were contacted by telephone in January 2022 and 80 agreed to distribute the questionnaire. They displayed an A4 poster with a brief explanatory text and the QR code to access the online questionnaire (via Limesurvey), as well as A7 cards containing the QR code.
Questionnaire
The questionnaire was created in the most comprehensive way possible from a narrative literature review on risk factors for non-HPV vaccination and non-screening for cervical cancer. It was tested twice by ten women aged 25–40 years (not included in the study), with rewriting of any unclear or ambiguous questions, and logical organization into subsections. It was divided into the following parts: Part 1: Sociodemographic characteristics of the women; Part 2: Behaviors, history, and information received regarding HPV and non-HPV vaccinations; Part 3: Behaviors, history, and information received regarding gynecologic follow-up and cervical cancer screening with the Papanicolaou test; Part 4: About their primary health care provider; Part 5: Women's knowledge of vaccination and screening.
Definition of Variables
The variables 'vaccination' and 'participation in screening' were binary. Any woman who reported having received at least one dose of vaccine was considered vaccinated. Any woman who reported having had a Pap smear within the past three years or in the past three years was considered screened. Any woman who reported having had a Pap smear more than three years ago or who reported never having had a Pap smear was considered unscreened.
The variable "knowledge about cervical cancer screening" was a score (from 0 to 4) constructed as the sum of correct answers to 4 questions about screening: 1) In your opinion, is a woman who has been vaccinated against HPV protected against all types of human papillomavirus? [good answer: "no"] 2) In your opinion, is screening necessary if a woman is vaccinated against HPV? [good answer: "yes"] 3) In your opinion, is it recommended to be screened for cervical cancer with a Pap smear? [good answer among 5: "from the age of 25 to 65"] 4) In your opinion, the purpose of a Pap smear is? [2 answers required out of 5: "to detect abnormal cells in the pre-cancerous stage", "to detect the presence of human papillomavirus"].
Qualitative variables analysis
Reasons for non-participation in vaccination or screening were provided by participants in free text. Semantic analysis allowed for qualitative exploration of participants' responses.
Statistical methods
The population of women aged 25 to 40 in Nord-Pas-de-Calais was approximately 375,000 on January 18, 2022. The minimum number of analyzable questionnaires required to achieve adequate power was 385, with a selected alpha risk of 5%. Standard errors for descriptive statistics of the entire population were calculated at the 95% confidence level [23]
Categorical variables were expressed as frequencies and percentages. Independence (or correlation) between two qualitative variables was tested using chi-squared tests. Fisher's exact test was used when theoretical frequencies were less than 5. Descriptive statistics were performed with Excel®. Bivariate statistical analyses were performed using jamovi 2.4.11.0 [24, 25] with a selected alpha risk of 5%.
Multivariable analyses for HPV vaccination status were performed using logistic regression, with the outcome variable "HPV vaccination status" and the explanatory variables "HPV information provider" and "area of residence". Candidate covariates were included in a penalized Least Absolute Shrinkage and Selection Operation (LASSO) model in order to provide a more robust logistic regression. The penalty coefficient (lambda) was chosen to provide an estimation error less than one standard deviation of the minimum error obtained by tenfold cross-validation, while being as parsimonious as possible. No variable had a coefficient different from 0 with this lambda coefficient [26].
Ethics
This study was the subject of a declaration to the Data Protection Officer of the University of Lille with an agreement received on January 12, 2022 (n° 2022–013) corresponding to the start of the study. The participation of physicians and women was voluntary. All data were collected anonymously and in accordance with the recommendations of the data protection officer. This work received no public or private funding.
Results
Sociodemographic characteristics
- - Study centers: 80 general practitioners (out of 400 randomly selected) agreed to be study centers. Of these, 62.5% were in the Nord department and 37.5% in the Pas-de-Calais department. Of these, 62.5% were men and 17.5% were university trainers of general practice residents. Study centers were homogeneously distributed on the territory.
- -Study population: Of the 80,000 patients in general practices in Nord-Pas-de-Calais, 602 women responded. Excluded were 98 incomplete questionnaires, 64 participants under 25 or over 40, 32 questionnaires (5,3%) where HPV vaccination status was unknown, 1 questionnaire (0,2%) where cervical cancer screening status was unknown.
Table 1 presents the sociodemographic descriptive statistics of the 407 participants enrolled. Table 1. Respondent characteristicsCharacteristics of respondentsn%Age ranges 25–29 years14435,4 30–34 years12129,7 35–40 years14234,9Socioprofessional category Farmers00,0 Craftsmen, shopkeepers, company managers153,7 Executives and higher intellectual professions14435,4 Intermediate professions4410,8 Employees146 35,9 Manual workers 10 2,4 Inactive who have already worked 35 8,6 Never worked 13 3,2 Location In town28971,0 In the country11829,0Department Nord28570,0 Pas-de-Calais12230,0Marital status Single5814,3 Cohabiting10325,3 Civil union9122,4 Married14134,6 Separated61,5 Divorced71,7 Widowed10,2Sexual relations Hetero37792,6 Homo112,7 Bi112,7 No sexual relations82,0Referring physician Men22544.7 Female18255.3 Performing pap smears10425.6 Not performing pap smears15036.9 Unknown15337.6 Working alone15939.1 Practicing in a group23357.2 Not known153.7
Comparison of the characteristics of vaccinated and unvaccinated women
40.8% of respondents were vaccinated against HPV viruses. Table 2 compares the characteristics (theoretically prior to their HPV vaccination) of vaccinated and unvaccinated participants. Table 2. Comparison of respondent characteristics by HPV vaccination status. HBV Hepatitis B virus. Fisher test when theoretical numbers < 5; Chi2 test CharacteristicsVaccinatedn (%)Unvaccinatedn (%)p valueTotal n**= 407**166 (40,8)241 (59,2)Age ranges 25–29 years98 (68,1)46 (31,9)< 0,001 30–34 years60 (49,6)61 (50,4) 35–40 years8 (5,6)134 (94,4)Location City128 (44,3)161 (55,7)0,02 Countryside38 (32,2)80 (67,8)Department Nord119 (41,8)166 (58,2)0,54 Pas-de-Calais47 (38,5)75 (61,5)HBV vaccination status Vaccinated120 (40,1)179 (59,9)0,15 Unvaccinated13 (28,9)32 (71,1)Information on HPV vaccination by Healthcare professional138 (58,7)97 (41,3)< 0,001 Entourage/Media/Internet21 (21,6)76 (78,4) No information7 (9,3)68 (90,7)
Vaccinated and unvaccinated women had similar characteristics except for age (i.e., year of vaccination), place of residence, and source of information about HPV vaccination. Women in the 35–40 age group (targeted for HPV vaccination in 2007–2010) were the least vaccinated (5.6%). Women in the 30–34 age group targeted for vaccination in 2007–2011 were less vaccinated (49.6%) than women in the 25–29 age group targeted for vaccination in 2007–2016 (68.1%). This difference was statistically significant (p < 0.001). Women living in cities were more likely to be vaccinated (44.3%) than women living in rural areas (32.2%), and this difference was also statistically significant (p = 0.02). Women who had received information about HPV vaccination from a health professional (124 from a general practitioner, 14 from a gynecologist) were significantly more likely to have been vaccinated.
Women vaccinated against HBV were more likely to be vaccinated against HPV, but this difference was not statistically significant (p = 0.15).
In multivariate analysis, women who had received information about HPV vaccination from a healthcare provider were significantly more likely to be vaccinated, after adjustment for age group and residence. Figure 1 shows the odds ratio of these three variables in relation to HPV vaccination status.Fig. 1. Multivariate analysis of risk factors for HPV non-vaccination
Reasons given for non-vaccination
The reasons given in the free fields ("not wanted" and "other") could be grouped into several categories: “I am over the age” 18 women; “no hindsight/doubt/start of vaccination” 15 women; “parents are against it” 14 women; “don't know what it is for/methods/not enough information” 8 women; “doesn't feel concerned” 7 women; “too late for sexual debut” 5 women; “vaccine not mandatory” 2 females.
Comparison of the characteristics of women taking part in UCC screening
Table 3 shows all the factors that characterize screened women compared to unscreened women. Table 3. Characteristics of women screenedCharacteristicsWomen screened n (%)p valueTotal n**=407364 (89,4)HPV vaccination status Vaccinated 141 (84,9)0,01 Unvaccinated223 (92,5)Age ranges 25–29 years117 (81,2)< 0,001 30–34 years113 (93,4) 35–40 years134 (94,4)Socioprofessional categories Farmers00,98 Craftsmen, shopkeepers,14 (93,3) Executives and higher intellectual professions128 (88,9) Intermediate professions40 (90,9) Employees131 (89,7) Manual workers9 (90,0) Inactive having already worked30 (85,7) Never worked12 (92,3)Location City255 (88,2)0,22 Countryside109 (92,4)Department Nord255 (89,8)0,97 Pas-de-Calais109 (89,3)Marital status Living together92 (89,3)< 0,01 Civil union partner 84 (92,3) Married130 (92,2) Single47 (81,0) Separated 4 (66,7) Divorced7 (100,0) Widowed0Sexual orientation** Hetero344 (91,2)< 0,001 Homo7 (63,6) Bi 9 (81,8) No sexual relations4 (50,0)Frequency of gynecological check-ups Every 6 months24 (96,0)< 0,001 Every year237 (95,6) Every 2 years75 (92,6) Every 3 years or more25 (67,6) No follow-up3 (18.8)Professional who performs gynecological check-ups MG18 (75,0)0,003 SF87 (91,6) Gynecologist256 (94,1)Information on cervical cancer screening by Healthcare professional240 (91,6)0,17 Surroundings/Media/Internet83 (87,4) No information41 (83,7)Attending physician Men196 (87,1)0,09 Female168 (92,3) Performing pap smears90 (86,5)0.53 Not performing pap smears136 (90,7) Working alone143 (89,9)0.48 Practicing in a group209 (89,7)Knowledge associated with screening (score) 0 No knowledge20 (87.0)0.21 167 (89.3) 2149 (93.7) 397 (85.1) 4 Excellent knowledge31 (86.1)
In bivariate analysis, screening rates were lower among women vaccinated against HPV viruses, younger women, single or separated women, and homosexual or asexual women. Vaccinated women screened less (15.1% nonparticipation) than unvaccinated women (7.5% nonparticipation), and this was statistically significant (p = 0.01). Women in the 30–34 and 35–40 age groups were significantly more likely to be screened (93.4% and 94.4%, respectively) than women in the 25–29 age group (81.2%) (p < 0.001). There was no significant difference according to socio-professional category (p = 0.99), department (p = 0.97), or place of residence (p = 0.22).
As the frequency of gynecologic follow-up decreased, the screening rate also decreased significantly (p < 0.001). The screening rate is significantly higher when the follow-up is performed by a midwife (91.6%) or a gynecologist (94.1%) than by a general practitioner (75%) (p = 0.003).
The low rate of unscreened women in our sample precluded multivariate analysis of the effect of vaccination status on screening rates. A sensitivity analysis was performed to assess whether the association remained significant in age subgroups (shown in Table 4). Table 4. Risk factors for non-screening of UCC by age subgroup. In each subgroup n provides the absolute number of screened women in one category and % provides the percentage of screened women in this category (for example 78 vaccinated women aged 25–29 were screened and they represent 79,6% of all 98 vaccinated 25–29 women)25–29 age group**(n= 144)Women screened30–34 age group****(n=121)Women screened35–40 age group****(n=142)Women screenedTotal n(%)117 (81,2)113 (93,4)134 (94,4)Characteristicsn (%)p valuen (%)p valuen (%)p valueVaccination status** Vaccinated78 (79,6)0,4655 (91.7)0.458 (100)0.48 Unvaccinated39 (84,8)58 (95.1)126 (94.0)Marital status In couple91 (84,3)0,1197 (94,2)0.41118 (95,2)0.28 Not a couple26 (72,2)16 (88,9)16 (88,9)Sexual orientation Heterosexual112 (85,5)** < 0,001106 (93,8)0.49126 (94,7)0.47 Bi/homo/a-sexual5 (38,5)7 (87,5)8 (88,9)Frequency of gynecological check-ups Every 6 months12 (92,3) < 0,0014 (100) < 0,0018 (100)< 0,001** Yearly70 (90,9)71 (95,9)96 (99) Every 2 years24 (82,8)28 (100)23 (95,8) Every 3 years or more9 (69,2)9 (75)7 (58,3) No follow-up2 (16,7)1 (33,3)0 (0)Professional who performs gynecological check-ups MG8 (80)0,588 (80)0.082 (50)< 0,001 SF32 (84,2)31 (96,9)24 (96) Gynecologist75 (89,3)73 (96,1)108 (96,4)
Sensitivity analysis showed that after adjusting for age, being screened was not significantly correlated with being vaccinated against HPV viruses. The only risk factor significantly correlated with non-screening regardless of age group was lack of regular gynecological follow-up.
Reasons given for not screening
20 women (4.9%) had never received pap smears. Of these, 95% were between the ages of 25 and 29. 23 women (5.6%) had received pap smears but were no longer up to date. Among the women who had never had a pap smear, the most common reasons for not having it were: “not wanted” (5 women, 3 of whom had been vaccinated), “not yet done because they were in their 25th year” (4 women, 3 of whom had been vaccinated), “problems with access to gynecological care” (3 women, 2 of whom had been vaccinated), “forgotten” (2 women, 1 of whom had been vaccinated), “not suggested by a health professional” (2 women, 1 of whom had been vaccinated).
Discussion
Vaccination against HPV
In 2022, 41 ± 5% of French women aged 25–40 years in the Nord-Pas-de-Calais region were vaccinated (at least one dose) against HPV viruses. This corresponds to the official epidemiologic figures for this age group in France [27]. The risk factors for non-vaccination, after adjustment, were the period of eligibility for vaccination in the early days of vaccination in France, information received from non-medical sources, or lack of information about vaccination. Qualitative reasons given by women who had not been vaccinated were mainly that they were older than the age for vaccination, that they doubted the safety of the vaccine, and that their parents were against vaccination.
In bivariate analysis, the HPV vaccination rate was lower in rural areas (32.2%) than in urban areas (44.3%), but this difference was no longer significant after adjustment. Several studies (international [28–30] and French [31, 32]) found that more women were vaccinated in urban areas. This could be explained by accessibility in terms of distance and frequency of medical centers, especially as a shorter distance between home and vaccination site was significantly associated with a better HPV vaccination rate in the Netherlands [33]. However, there appeared to be no difference in vaccine acceptance between rural and urban areas [34]. There was also no difference in vaccine recommendation between general practitioners practicing in rural and urban areas [35].
The main source of information about vaccination was medical (57 ± 5%), with GPs accounting for 80%. GPs were identified as the main source of information in 46% of cases, all sources combined. These results are similar in the general population, as shown by a survey conducted by INCa and HAS in 2019, in which 86% of parents identified their GP as their main source of information on this topic. Moreover, in the same study, 96% of GPs stated that they were in favor of vaccination, but only 40% systematically offered it, fearing a refusal that could lead to conflict [27]. Similarly, in our study, only 46% of women (themselves or their parents) were offered vaccination by their GP. The provision of information by the general practitioner seems essential to increase the knowledge of parents and young girls, to improve their understanding of the issues, and thus to increase their acceptance of the vaccination. This is confirmed by the first reason for non-vaccination, “not suggested by a health professional”.
Screening for UCC
In our sample, 90 ± 3% of French women aged 25–40 years in the Nord-Pas-de-Calais region had been screened for UCC by a Pap smear in the previous 3 years. In bivariate analysis, women at risk of not being screened were the youngest, HPV vaccinated, non-heterosexual, living alone, having gynecologic follow-up by their general practitioner, and not having regular gynecologic follow-up. Sensitivity analysis by age subgroup showed that the only risk factor that remained significantly correlated with non-screening regardless of age group was lack of regular gynecologic follow-up.
Regarding the association between vaccination and screening, the Australian studies showed both a negative [22] and a positive [19] effect of vaccination on screening. The data linkage process was different in the two studies, and the positive effect was mainly found in the most recent study (2019 vs 2014). Overall, a positive association between HPV vaccination and HPV screening has been reported in the literature from Sweden in 2015 [20], the United States [18, 36], Italy [21], Japan [37], and the United Kingdom and Denmark [14, 15]. In a Canadian study, participation in screening was significantly lower among vaccinated women than among unvaccinated women, but as in our study, this difference was no longer significant after adjustment for age [38]. For the time being, it seems difficult to obtain an answer in France, as HPV vaccination only started in 2007 and its indications are still evolving, first for women and then for the whole population. For example, to study a cohort of 35-year-old women (covered by screening for 10 years) potentially vaccinated in 2013–2015, we will have to wait until 2037.
Regarding participation in screening, in our study the overall screening coverage and the coverage by age group were higher than those reported at departmental and national level for the period 2017–2020 [39]. This could be explained by a bias in patient volunteering and an overrepresentation of women in couples. In addition, other studies that used a declarative method to assess participation in screening found high participation rates [16, 40] of around 90%.
Several sociodemographic factors are associated with screening in the literature. Women who live with a partner, have a higher income, have supplementary private health insurance, and have consulted a gynecologist in the past 12 months were most likely to undergo screening [41]. A significant association has been found between the socioeconomic level of the neighborhood surrounding the primary care practice and participation in UCC screening at that practice [42]. There was also a significant relationship between the density of gynecologists within 5 km and between 20 and 40 km of the GP practice, with a greater effect for less than five kilometers [43]. In our study, we only knew the socio-professional category, age, and department. Demographic and social data such as income, supplementary health insurance, distance to a general practitioner's office and distance to a gynecologist's office were not collected. However, we found the effect of gynecological follow-up on a declarative basis. Women in France are encouraged to have an annual gynecological follow-up consultation 1) to discuss contraception and sexually transmitted infections (STI), 2) to propose recommended screening. Self-sampling of STI is annually proposed for women under 25. Annual clinical breast monitoring is proposed from age 25. Cervical cancer screening is proposed every 3 years from age 25 and then every 5 years from age 30 to 65.
Knowledge of the women has been identified as a risk factor for poor screening in Ethiopian police officers [44] but was not a risk factor in our population, probably because women in our sample were predominantly screened.
Strengths and limitations
One of the strengths of this study was its originality and the fact that it was conducted in a primary care setting. To our knowledge, it was the first of its kind in France. The doctors were randomly selected, which allowed us to randomly distribute the questionnaire throughout the Nord and Pas-de-Calais regions. The fact that we distributed our questionnaire electronically was also a strength. Indeed, several studies have shown that the validity of methods based on an electronic format is equivalent to that of paper questionnaires [45, 46]. The posters and QR code cards allowed women to respond while waiting in the waiting room and later.
There was a selection bias because the doctors recruited were likely to be more sensitive to and interested in the topic of the study. There was also a voluntary selection bias because only motivated patients responded. This double selection bias could lead to an over-representation of health-conscious women amplified by an over-representation of voluntary doctors having a greater interest in cervical cancer. It could present an overly optimistic view of preventive measures. In addition, women who did not have a telephone or Internet connection and those with little or no access to health care were unable to respond, although these may be the most disadvantaged populations and those furthest from the health care system, with low vaccination and screening rates. There was a recall bias for both vaccination and screening due to the self-reporting mode, as reported in the literature [47]. There was a social desirability bias, particularly as the questionnaire was displayed in a doctor's surgery where anonymity was limited. For future research, we should consider stratified sampling, and using administrative date instead of self-reports.
Conclusion
In young women, participation in HPV vaccination and UCC screening is enhanced by medical information from the family doctor and regular gynecological check-ups. The internal validity of this study was strengthened by its multicenter design with random selection of practices, but limited by selection bias (recruitment was done in the practices by patients interested in the topic), recall bias (the questionnaire was retrospective), and survey bias (the questionnaire was anonymous). The main drawback is the relatively recent promotion of HPV vaccination in France. It would be advisable to repeat this study starting in 2037 to obtain robust results on the effect of vaccination on screening.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sung H Ferlay J Siegel RL Laversanne M Soerjomataram I Jemal A Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries CA Cancer J Clin 20217120924910.3322/caac.2166033538338 · doi ↗ · pubmed ↗
- 2Hamers FF Woronoff A-S Cancer du col de l’utérus en France : tendances de l’incidence et de la mortalité jusqu’en 2018 Bull Epidémiol Hebd 201922–23410
- 3Bajos N Bozon M Beltzer N Laborde C Andro A Ferrand M Changes in sexual behaviours: from secular trends to public health policies AIDS Lond Engl 2010241185119110.1097/QAD.0b 013e 328336 ad 5220299962 · doi ↗ · pubmed ↗
- 4Beck F, Richard J-B. Les comportements de santé des jeunes: analyses du Baromètre santé 2010. Saint-Denis: INPES éd; 2013. https://www.santepubliquefrance.fr/docs/les-comportements-de-sante-des-jeunes-analyses-du-barometre-sante-2010.
- 5Cancer du col de l’utérus. https://www.who.int/fr/news-room/fact-sheets/detail/cervical-cancer. Accessed 17 May 2022.
- 6Urrutia M-T Araya A-X Gajardo M Chepo M Torres R Schilling A Acceptability of HPV Vaccines: A Qualitative Systematic Review and Meta-Summary Vaccines 202311148610.3390/vaccines 1109148637766161 PMC 10536942 · doi ↗ · pubmed ↗
- 7Gorgone M Squeri A Cuffari S Fauci VL Giunta I Calderone S Rates of Primary and Secondary Prevention of Cervical Cancer: A Study in a Province in the South of Italy Vaccines 202311168810.3390/vaccines 1111168838006020 PMC 10675516 · doi ↗ · pubmed ↗
- 8Jin SW Lee Y Lee S Jin H Brandt HM Factors Associated with College Students’ Human Papillomavirus (HPV) Vaccination and Preferred Strategies for Catch-Up Vaccine Promotion: A Mixed-Methods Study Vaccines 202311112410.3390/vaccines 1106112437376513 PMC 10303150 · doi ↗ · pubmed ↗