Haemophilus parainfluenza-Associated Aortic Root Abscess and Septic Embolic Stroke Post-transcatheter Aortic Valve Replacement: A Case Study
Tirumala Nischal Jasty, Jaswanth R Jasti, Smit Shah, Jared Green

TL;DR
A rare case of aortic root abscess and stroke caused by Haemophilus parainfluenza is reported in a patient who recently had heart valve replacement.
Contribution
This case study highlights a rare complication involving H. parainfluenza post-transcatheter aortic valve replacement.
Findings
Haemophilus parainfluenza was identified as the causative agent of aortic root abscess and septic embolic stroke.
Intravenous antibiotics successfully resolved the infection and related symptoms without surgical intervention.
Abstract
We present a rare instance of aortic root abscess and septic embolic stroke due to Haemophilus parainfluenza in a 75-year-old male patient who had undergone a recent transcatheter aortic valve replacement. The patient initially presented with generalized weakness and altered mental status. Blood cultures grew Haemophilus parainfluenza. Brain imaging showed multiple infarcts with some areas of hemorrhagic conversion. Echocardiography demonstrated an aortic root abscess as well as vegetation on the tricuspid valve. Surgical correction was deemed high risk; hence, management involved intravenous (IV) antibiotics, resulting in the resolution of both symptoms and the abscess.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
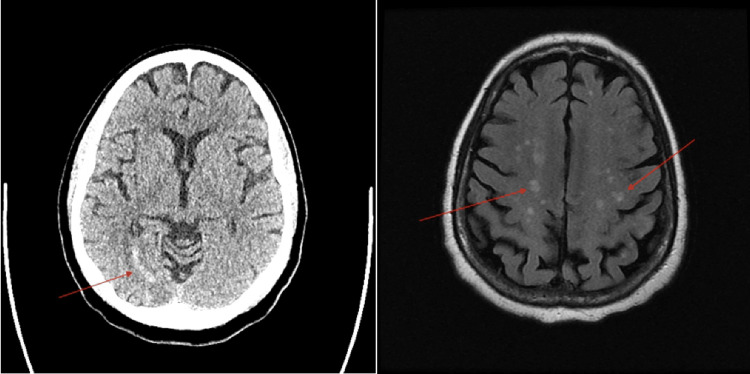 Figure 1
Figure 1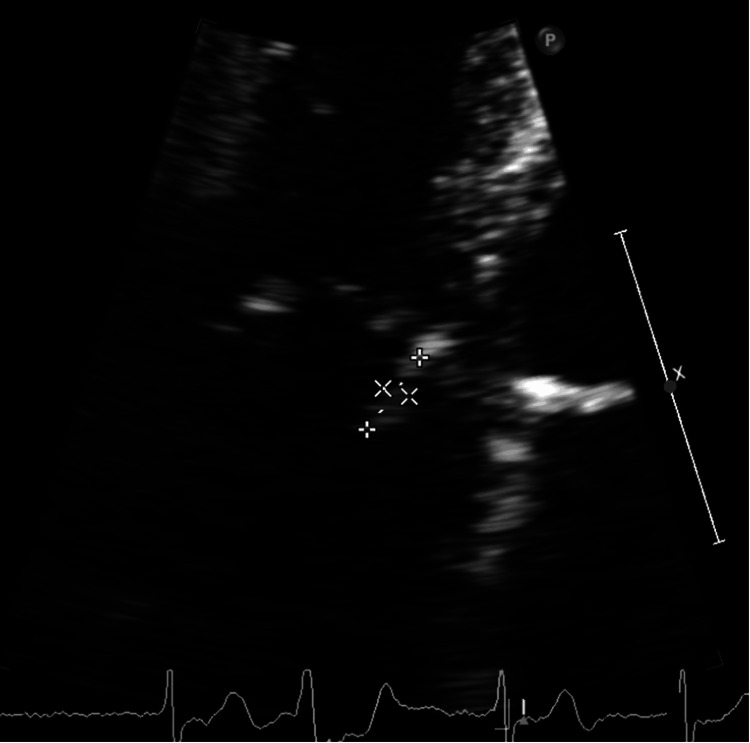 Figure 2
Figure 2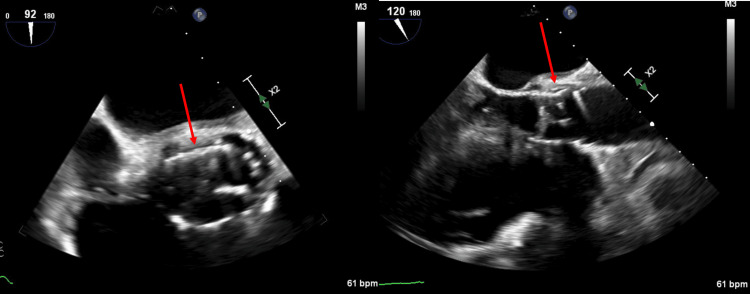 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfective Endocarditis Diagnosis and Management · Bacterial Infections and Vaccines · Central Venous Catheters and Hemodialysis
Introduction
Transcatheter aortic valve replacement (TAVR) is a minimally invasive procedure increasingly used in the treatment of aortic stenosis, especially in high-risk surgical patients [1]. While the procedure has revolutionized the management of this condition, it is not without complications, one of them being infective endocarditis (IE) leading to systemic embolization [2]. Haemophilus species, part of the Haemophilus, Aggregatibacter, Cardiobacterium hominis, Eikenella corrodens, and Kingella species group (HACEK group), are normal inhabitants of the oropharynx. While these organisms are commonly benign, they are rare but notable causes of IE [3]. Here, we report a rare case of Haemophilus parainfluenza aortic root abscess and septic embolic stroke following a recent TAVR procedure. This case highlights the importance of timely diagnosis and the challenges in managing post-TAVR infective complications.
Case presentation
A 75-year-old male with a history of coronary artery disease and aortic stenosis post-recent TAVR (two months ago) presented to our emergency department with generalized weakness and altered mental status. Four weeks earlier, he had an outpatient office visit when no clinical changes, electrocardiogram (EKG), or transthoracic echocardiogram (TTE) abnormalities were noted. At presentation, the patient was febrile with a temperature of 101.3°F (38.5°C) but hemodynamically stable on room air. With the patient being encephalopathic, history was limited; however, a review of past medical history was significant for other comorbidities, including chronic lymphocytic leukemia with anemia and thrombocytopenia, hypertension, and hyperlipidemia. The patient was only oriented toward self; physical examination was otherwise unremarkable. Complete blood count with differential showed a white blood cell count of 20,700 K/uL (baseline: 10000-11000 K/uL) with neutrophilic predominance, hemoglobin of 8 g/dL (at baseline), and a platelet count of 98,000 K/uL (at baseline). Serum chemistry was unremarkable. Lactic acid was elevated at 5.9 mmol/L (reference: 0.6-1.4 mmol/L). High-sensitivity troponin was within normal limits, and the EKG showed a normal sinus rhythm. A non-contrast computed tomography (CT) and magnetic resonance imaging (MRI) of the brain revealed multiple infarcts in the middle cerebral artery (MCA) and posterior cerebral artery (PCA) territories with hemorrhagic conversion, suggesting an embolic source (Figure 1).
CT scan of the head in axial section (left) reveals an infarction in the right PCA area (red arrow). MRI of the brain in axial section (right) shows numerous infarcts, suggesting an embolic cause (red arrows).CT: Computed tomography; PCA: posterior cerebral artery; MRI: magnetic resonance imaging
A stroke code was called; however, the patient was not a candidate for reperfusion therapies due to hemorrhagic conversion and a suspicion of septic embolic stroke. The sepsis protocol was initiated: blood cultures were obtained, and the patient was started on broad-spectrum antibiotic coverage with vancomycin and cefepime. TTE showed a well-seated Edwards SAPIEN bioprosthetic valve in the aortic area (Video 1) with normal gradients but noted a mobile echo density on the septal tricuspid valve leaflet (Video 2 and Figure 2) .
TTE showing a well-seated bioprosthetic aortic valve in short axis view.TTE: Transthoracic echocardiogram
TTE in apical four-chambered view (tricuspid valve zoomed in), exhibiting a 0.4 x 1 cm mobile echo density on the atrial side emerging from the base of the septal tricuspid valve leaflet.TTE: Transthoracic echocardiogram
Zoomed-in view of the tricuspid valve in apical four-chambered view, redemonstrating the mobile echo density as seen in Video 2 (pointers).
Two sets of blood cultures with polymerase chain reaction (PCR) panel identified Haemophilus parainfluenza, increasing the suspicion for valvular endocarditis. Transesophageal echocardiography (TEE) was pursued and revealed significant thickening and echolucency of the intervalvular fibrosa, suggesting an aortic root abscess (Figure 3).
Transesophageal echocardiogram short axis aortic view (left). Transesophageal echocardiogram long axis view focusing on the aortic valve (right).TAVR: Transcatheter aortic valve replacementHistory of TAVR. Note the well-seated prosthesis. Echo-free space noted (as shown by the arrow) adjacent to the mitral valve annulus in continuous with the intervalvular fibrosa. There is significant thickening and echolucency of intervalvular fibrosa suggestive of aortic root abscess
The patient was not deemed to be a surgical candidate given the high surgical risk. The patient's mental status improved with antibiotic therapy. Following final blood culture results and sensitivities, vancomycin was discontinued, and the patient was discharged with a peripherally inserted central catheter (PICC) to complete a six-week course of intravenous (IV) cefepime. Follow-up TTE in the clinic after completion of antibiotic therapy showed complete resolution of the aortic root abscess and the tricuspid valve vegetation.
Discussion
IE is an uncommon but serious complication following TAVR. In spite of major advancements in the TAVR procedure, the incidence of IE after TAVR remains stable, with 0.3 to 2 per 100 person-years similar to that after surgical aortic valve replacement (SAVR) [4]. Significant risk factors for IE following TAVR encompass a previous history of IE, diabetes, chronic obstructive pulmonary disease, chronic kidney disease, pulmonary hypertension, atrial fibrillation, and receiving blood transfusions during TAVR hospitalization [5,6]. These factors are notable but not all-inclusive. Generally, the most frequent initial symptom of TAVR-related IE (TAVR-IE) is fever, observed in about 80% of cases, followed by new-onset heart failure, which appears in roughly 40% of cases [7,8]. Additionally, around 13% of patients experience systemic embolic events [9]. It is important to mention that atypical and nonspecific symptoms are more commonly seen in patients with TAVR-IE.
IE after TAVR is a specific type of prosthetic valve endocarditis (PVE), posing significant challenges due to its distinct clinical and microbiological characteristics. In high-income countries, Staphylococci, particularly Staphylococcus aureus, are the primary pathogens for both native and prosthetic valve IE [9]. However, the most common microorganisms in TAVR-IE include Enterococci,* S. aureus*, and coagulase-negative Staphylococci [8]. Although infrequent, HACEK organisms, which normally reside in the oral and upper respiratory tracts, have also been identified in TAVR-IE cases. These are implicated in about 1-3% of all IE cases due to their ability to invade blood vessels following trauma or local infection [3,10]. HACEK endocarditis often has an insidious onset, and diagnosis is typically delayed in prosthetic valves because these slow-growing bacteria frequently lead to initially negative blood cultures. While the incidence of PVE is on the rise, HACEK-related PVE is uncommon but critical to address promptly due to its potential for severe outcomes.
IE following TAVR is linked with a high incidence of serious complications, affecting up to 70% of patients in certain studies [7]. The most frequent complications reported during the initial hospital stay include acute heart failure, acute renal failure, septic shock, acute myocardial infarction, and systemic embolism [9,11]. Additionally, paravalvular issues and abscesses are relatively common, with occurrences reported between 3.6% and 19.1% [9]. Regardless of the treatment approach, IE after TAVR is associated with extremely high mortality rates.
The Modified Duke’s criteria are less effective for diagnosing TAVR-IE than for native valve IE, mainly because of the higher frequency of negative blood cultures and ambiguous echocardiographic findings. A significant nationwide study highlighted the limited sensitivity of TTE and TEE in detecting TAVR-IE [12]. These echocardiographic studies were found to be normal or inconclusive in nearly half of the TAVR-IE cases, indicating a substantial diagnostic challenge. The American College of Cardiology and the American Heart Association have endorsed multidetector CT with a Class IIA recommendation for diagnosing TAVR PVE [13]. CT is particularly effective in identifying abscesses and pseudoaneurysms, offering diagnostic precision comparable to TEE.
Currently, there are no randomized trials comparing different antibiotic treatments or strategies for TAVR-IE, leaving treatment largely guided by general guidelines for PVE [14]. IV antibiotic therapy should be tailored based on the microorganism's profile and susceptibility tests. Initial empiric treatment should target Staphylococci, Streptococci, Enterococci, and Gram-negative bacteria. If an infection persists beyond one week, a reevaluation for potential alternative infection sources is necessary before considering surgery. Urgent surgical intervention for PVE may be needed for severe complications such as acute regurgitation leading to shock, heart failure due to severe obstruction, or persistent infections despite adequate therapy [15]. Despite indications for surgery in about 80% of TAVR-IE cases, surgical interventions remain exceptionally rare, with few studies reporting rates above 20% [15]. Antibiotic therapy for TAVR-IE should typically extend for at least six weeks, reflecting its classification as a subset of PVE [16]. However, the underrepresentation of TAVR patients in PVE studies means that findings from these studies might not fully apply to the TAVR-IE population. Overall, the management of TAVR-IE remains uncertain, with conservative treatment via antibiotics being the predominant strategy despite the potential benefits of surgical intervention observed in native valve endocarditis and PVE.
In this case, the patient exhibited acute mental status changes and generalized weakness due to a septic embolic stroke, driven by underlying TAVR-IE with an aortic root abscess. The presentation of sepsis after TAVR raised suspicions of PVE over other causes of embolic stroke. While TTE and TEE demonstrated aortic root abscess and tricuspid valve vegetations, indicating TAVR-IE, it is important to note that echocardiography can sometimes be less sensitive in diagnosing this condition. Nevertheless, in this instance, the echocardiograms were definitive. Blood cultures complemented with a PCR panel successfully identified Haemophilus parainfluenza as the causative agent, despite HACEK organisms typically being culture-negative. Although there was a clear indication for surgical intervention, the patient's multiple comorbidities placed him at high surgical risk. Consequently, the decision was made to manage the condition medically. The patient was treated with six weeks of IV antibiotics, leading to complete resolution of clinical symptoms and normalization of echocardiographic findings.
Conclusions
This case highlights the need for careful monitoring of TAVR patients for potential complications, such as IE. Unlike PVE or native valve endocarditis, TAVR-IE presents a unique and atypical profile. This necessitates individualized treatment plans tailored to address the specific challenges and complexities of this serious condition.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1ACC/AHA and ESC/EACTS guidelines for the management of valvular heart diseases: JACC guideline comparison J Am Coll Cardiol Coisne A Lancellotti P Habib G 721734822023
- 2Transcatheter aortic valve replacement associated infective endocarditis case series: broadening the criteria for diagnosis is the need of the hour BMC Cardiovasc Disord Lnu K Ansari S Mahto S 5592120213480099410.1186/s 12872-021-02364-0PMC 8606088 · doi ↗ · pubmed ↗
- 3HACEK infective endocarditis: characteristics and outcomes from a large, multi-national cohort P Lo S One Chambers ST Murdoch D Morris A 08201310.1371/journal.pone.0063181 PMC 365688723690995 · doi ↗ · pubmed ↗
- 4Prosthetic valve endocarditis following transcatheter aortic valve implantation J Cardiovasc Med (Hagerstown) Ali N Baig W Wu J Blackman D Gillott R Sandoe JA 5105162120203233238010.2459/JCM.0000000000000961 · doi ↗ · pubmed ↗
- 5Infective endocarditis after transcatheter aortic valve implantation: a nationwide study Eur Heart J Bjursten H Rasmussen M Nozohoor S Götberg M Olaison L Rück A Ragnarsson S 326332694020193143347210.1093/eurheartj/ehz 588PMC 6911164 · doi ↗ · pubmed ↗
- 6Risk of infective endocarditis after surgical and transcatheter aortic valve replacement Heart Cahill TJ Raby J Jewell PD 63964710820223505829510.1136/heartjnl-2021-320080 · doi ↗ · pubmed ↗
- 7Infective endocarditis after transcatheter aortic valve replacement: JACC state-of-the-art review J Am Coll Cardiol Del Val D Panagides V Mestres CA MiróJM Rodés-Cabau J 394412812023 https://doi.org/10.1016/j.jacc.2022.11.0283669714010.1016/j.jacc.2022.11.028 · doi ↗ · pubmed ↗
- 8TAVR-associated prosthetic valve infective endocarditis: results of a large, multicenter registry J Am Coll Cardiol Latib A Naim C De Bonis M 217621786420142545740610.1016/j.jacc.2014.09.021 · doi ↗ · pubmed ↗