An Atypical Case of Hemolytic Uremic Syndrome Caused by Shiga Toxin Produced by Aeromonas spp
Soloman R Kreik

TL;DR
An elderly woman developed hemolytic uremic syndrome from a rare bacterial toxin, highlighting new causes in adults.
Contribution
Identifies Aeromonas hydrophila as a novel cause of HUS in an adult, expanding understanding of its etiology.
Findings
A 77-year-old woman developed HUS after consuming raw oysters contaminated with Aeromonas hydrophila.
Stool antigen testing and blood culture confirmed the presence of Shiga-like toxin and Aeromonas hydrophila.
The case highlights the need for broader clinical awareness of non-traditional HUS causes in adults.
Abstract
Hemolytic uremic syndrome (HUS), traditionally recognized in pediatric populations, is characterized by renal insufficiency, hemolytic anemia, and thrombocytopenia, often linked to Shiga-like toxin (SLT) exposure. While typically associated with enteric pathogens like Escherichia coli (E. coli) and Shigella, Aeromonas spp. has also been identified as potential SLT producers, posing a new challenge. This study presents an exceptional case of HUS in a 77-year-old female, implicating Aeromonas hydrophila as the causative agent. The patient's clinical trajectory, marked by acute kidney injury post-consumption of raw oysters, underscores the unorthodox manifestation of HUS in adults. Diagnostic confirmation via stool antigen testing and blood culture revealed the presence of SLT and Aeromonas hydrophila, respectively. This case underscores the evolving landscape of HUS etiology, stressing…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
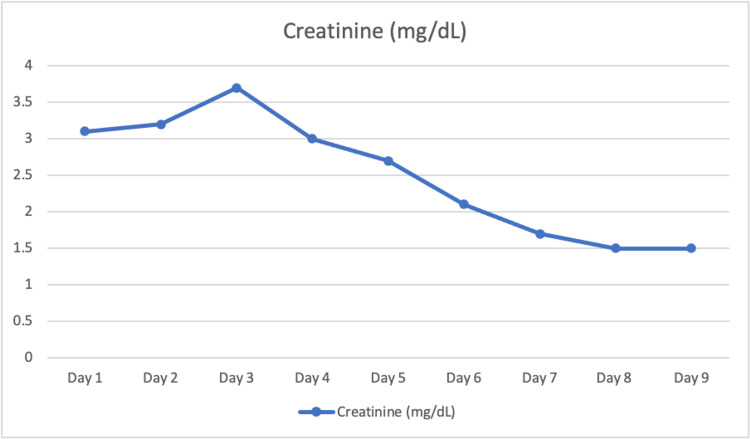 Figure 1
Figure 1 Figure 2
Figure 2| Component | Normal Range | Patient Values | Units |
| CBC | |||
| White Blood Cell Count (WBC) | 4,500 - 11,000 | 12,300 | cells/µL |
| Red Blood Cell Count (RBC) | Female: 4.2 - 5.4 | 3.8 | 10^6 cells/µL |
| Hemoglobin (Hgb) | Female: 12.1 - 15.1 | 10.1 | g/dL |
| Hematocrit (Hct) | Female: 36.1 - 44.3 | 33.5 | % |
| Platelet Count | 150,000 - 450,000 | 102,000 | platelets/µL |
| Mean Corpuscular Volume (MCV) | 80 - 100 | 82 | fL |
| Mean Corpuscular Hemoglobin (MCH) | 27 - 31 | 29 | pg/cell |
| Mean Corpuscular Hemoglobin Concentration (MCHC) | 32 - 36 | 32 | g/dL |
| Red Cell Distribution Width (RDW) | 11.5 - 14.5 | 16.1 | % |
| CMP | |||
| Glucose | 70 - 100 | 135 | mg/dL |
| Sodium (Na) | 135 - 145 | 133 | mmol/L |
| Potassium (K) | 3.5 - 5.1 | 4.1 | mmol/L |
| Chloride (Cl) | 98 - 107 | 102 | mmol/L |
| Carbon Dioxide (CO2) | 23 - 29 | 25 | mmol/L |
| Calcium (Ca) | 8.5 - 10.5 | 9.1 | mg/dL |
| Total Protein | 6.0 - 8.3 | 7.1 | g/dL |
| Albumin | 3.4 - 5.4 | 4.2 | g/dL |
| Total Bilirubin | 0.1 - 1.2 | 1.4 | mg/dL |
| Alkaline Phosphatase (ALP) | 44 - 147 | 162 | IU/L |
| Aspartate Aminotransferase (AST) | 10 - 40 | 27 | IU/L |
| Alanine Aminotransferase (ALT) | 7 - 56 | 32 | IU/L |
| Blood Urea Nitrogen (BUN) | 7 - 20 | 23 | mg/dL |
| Creatinine | 0.6 - 1.1 | 3.1 | mg/dL |
| Lactate dehydrogenase (LDH) | 140 – 280 | 346 | U/L |
| Haptoglobin | 41 - 165 | 28 | mg/dL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEscherichia coli research studies · Vibrio bacteria research studies · Complement system in diseases
Introduction
This article was previously presented as a poster presentation at the American College of Chest Physicians Annual Chest Meeting on October 9, 2023. Hemolytic uremic syndrome (HUS) is a leading cause of acute kidney injury in infants and young children, rarely affecting adults. It is defined as a triad of renal insufficiency, hemolytic anemia, and thrombocytopenia associated with a Shiga-like toxin (SLT). SLT is an antigen associated with diarrhea and plays a role in the pathogenesis of HUS. Typically, the toxin is generated by Escherichia coli (E. coli) or Shigella species. However, recent research indicates that Aeromonas species, which were previously known to cause infections mainly in immunocompromised individuals, can also produce active SLT [1,2]. We present an atypical case of HUS caused by SLT-producing Aeromonas hydrophila.
Case presentation
A 77-year-old female with a past medical history of hypertension presented with one day of worsening lethargy. The patient complained of bloody diarrhea and diffuse abdominal pain. She endorsed eating raw oysters a day prior. On examination, her abdomen was diffusely tender to palpation. Initial labs revealed a creatinine of 3.1 mg/dL, hemoglobin of 10.1 g/dL, and a platelet count of 102,000/µL. Complete blood count (CBC) and comprehensive metabolic panel (CMP) were otherwise unremarkable (Table 1, Figure 1).
Creatinine trend
A CT angiogram of the abdomen and pelvis showed patent celiac, superior mesenteric, and inferior mesenteric arteries (Figure 2). The patient was bolused with normal saline and started on vancomycin and flagyl after blood cultures were drawn. Peripheral blood smear returned with schistocytes, lactate dehydrogenase (LDH) was elevated at 346 U/L and haptoglobin was low at 28 mg/dL. The patient’s renal status worsened until day 3, at which time the stool antigens returned positive for Shiga toxin and the blood culture showed Aeromonas hydrophila bacteremia. At day 9 the patient’s renal function subsequently returned to baseline, and she was discharged.
CT angiogram of the abdomen The image is depicting patent celiac, superior mesenteric, and inferior mesenteric arteries.
Discussion
HUS is a microvascular occlusive disease that damages the glomeruli due to the accumulation of platelets and sheared red blood cells [1]. Isolation of *Aeromonas hydrophila-*produced SLTs is concerning, as these toxins are associated with HUS. Aeromonas spp. producing SLTs could be an emergent pathogen in the pathophysiology of HUS [2]. This was a rare phenomenon, which is now proven by PCR amplification of the stx1 and stx2 genes in many similar cases [3]. This case highlights the challenges in diagnosing atypical HUS. Our patient’s HUS diagnosis demonstrated a prodromal illness of diarrhea, thrombocytopenia, anemia, and development of renal failure. The pathophysiology of renal failure revolves around a cascade triggered by a direct insult of both SLT and the rupture of red blood cells. This process is believed to involve the toxin's journey through the bloodstream, targeting endothelial cells within the glomerular capillaries, mesangial cells, and tubular cells. The initial damage to endothelial cells sets off a series of events, including an increase in platelet aggregation and adhesion, ultimately leading to the formation of micro-thrombi [4]. This prothrombotic state exacerbates the injury, contributing to the progression of renal damage. Roughly two-thirds of individuals diagnosed with HUS need renal replacement therapy, and fortunately, most of them eventually recover renal function [5]. Conversely, around one-third of patients experience less severe renal complications and may not require dialysis treatment [6]. Early identification of HUS will allow prompt management and the prevention of long-standing renal failure.
Conclusions
In summary, our case report emphasizes the importance of identifying Aeromonas hydrophila as a potential contributor to hemolytic uremic syndrome (HUS). By delving into the underlying mechanisms of HUS, we've highlighted the significance of microvascular occlusion and the production of Shiga-like toxins (SLTs) by Aeromonas spp. This underscores the shifting landscape of infectious agents associated with HUS, emphasizing the emergence of Aeromonas spp. as a noteworthy pathogen. Our findings serve as a crucial reminder of the dynamic nature of infectious diseases and the necessity of remaining vigilant in identifying novel causative agents.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Aeromonas spp. clinical microbiology and disease J Infect Parker JL Shaw JG 1091186220112116329810.1016/j.jinf.2010.12.003 · doi ↗ · pubmed ↗
- 2Septic shock due to Aeromonas hydrophila bacteremia in a patient with alcoholic liver cirrhosis: a case report J Med Case Rep Yumoto T Ichiba S Umei N 402820142546498110.1186/1752-1947-8-402PMC 4289225 · doi ↗ · pubmed ↗
- 3Active Shiga-like toxin produced by some Aeromonas spp., isolated in Mexico City Front Microbiol Palma-Martínez I Guerrero-Mandujano A Ruiz-Ruiz MJ Hernández-Cortez C Molina-López J Bocanegra-García V Castro-Escarpulli G 1522720162772581310.3389/fmicb.2016.01522 PMC 5036386 · doi ↗ · pubmed ↗
- 4Atypical hemolytic-uremic syndrome: a case report and literature review Am J Case Rep Rafiq A Tariq H Abbas N Shenoy R 1091141620152570814610.12659/AJCR.892907 PMC 4341946 · doi ↗ · pubmed ↗
- 5Renal transplantation in HUS patients with disorders of complement regulation Pediatr Nephrol Zimmerhackl LB Scheiring J Prüfer F Taylor CM Loirat C 10162220071705805110.1007/s 00467-006-0210-7 · doi ↗ · pubmed ↗
- 6Treatment and outcome of Shiga-toxin-associated hemolytic uremic syndrome (HUS)Pediatr Nephrol Scheiring J Andreoli SP Zimmerhackl LB 174917602320081870450610.1007/s 00467-008-0935-6PMC 6901419 · doi ↗ · pubmed ↗