Surgical Treatment of Pseudoaneurysm of the Right Hepatic Artery Following Cholecystectomy: A Case Report
Abdellah Nouri, Ahmed Bensaad, Youssef Ghaddou, Sair Khalid, Fadil Abdelaziz

TL;DR
A patient developed a pseudoaneurysm of the right hepatic artery after cholecystectomy and required surgical treatment due to unavailability of embolization.
Contribution
This case report highlights the rare complication of right hepatic artery pseudoaneurysm and the surgical management when embolization is not available.
Findings
Surgical resection and ligation of the pseudoaneurysm was performed due to hemodynamic instability.
MRI confirmed the presence of a large hematoma and pseudoaneurysm post-cholecystectomy.
Embolization unavailability necessitated surgical intervention as the primary treatment.
Abstract
Pseudoaneurysms of the right hepatic artery following cholecystectomy are caused by either vascular damage or erosion after a biliary leak. Symptoms often include haemobilia, melena, vomiting, jaundice, and hemodynamic failure due to aneurysm rupture. The ideal treatment is arterial embolization or, in rare cases, stenting. We present a case of pseudoaneurysm of the right hepatic artery post-laparoscopic cholecystectomy. The patient presented with abdominal pain, vomiting, and hemodynamic failure on postoperative day 45. Magnetic resonance imaging (MRI) showed a large hematoma and a pseudoaneurysm of the right hepatic artery. A laparotomy was performed, and a large hematoma was found and evacuated. After the pringle maneuver, the pseudoaneurysm was resected. The right hepatic artery was ligated with clips, and a sub-hepatic drain was placed. The non-availability of emergency…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
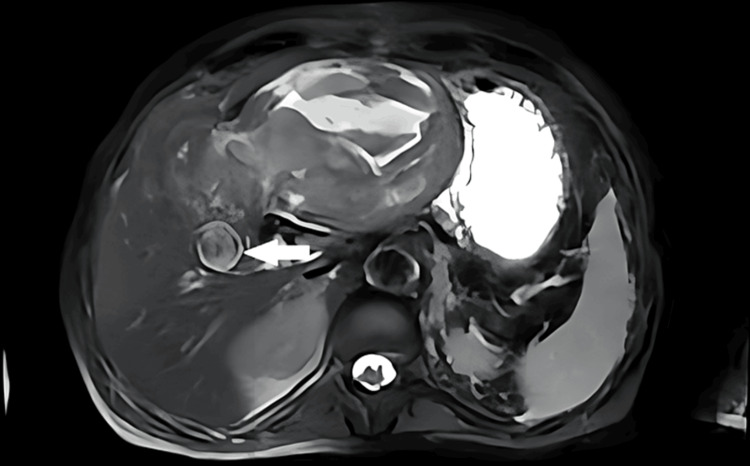 Figure 1
Figure 1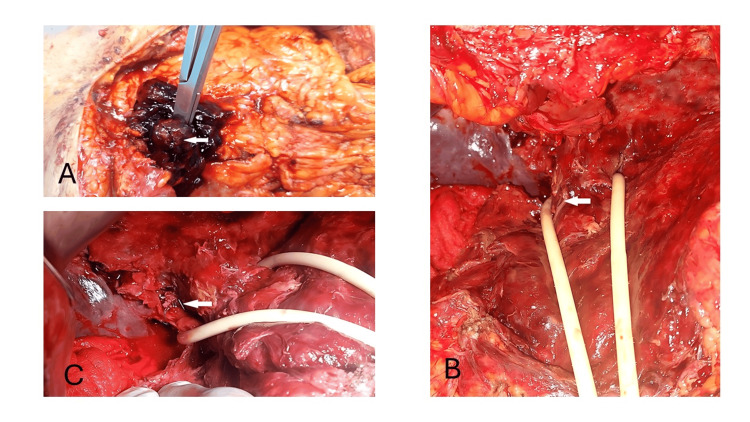 Figure 2
Figure 2| Parameter | Normal laboratory value | Value |
| Hemoglobin g/dl | 13-18 | 8 |
| Hematocrit % | 39-53 | 20.3 |
| Platelet 103 /uL | 150-400 | 310 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAbdominal vascular conditions and treatments · Gallbladder and Bile Duct Disorders · Liver Disease and Transplantation
Introduction
Cholelithiasis affects 10% to 15% of the Western population [1]. The standard treatment for symptomatic gallstones is laparoscopic cholecystectomy [1]. Biliary duct injury complicates 0.6% of cholecystectomies and is often associated with injury to the right hepatic artery, which manifests as a pseudoaneurysm. These patients may also present with haemobilia or hemoperitoneum [2].
Diagnosis is primarily based on angiography or magnetic resonance imaging (MRI). The ideal treatment is embolization, with surgical treatment involving ligation of the right hepatic artery reserved for cases when embolization fails or the patient is hemodynamically unstable. We present a case of pseudoaneurysm of the right hepatic artery following laparoscopic cholecystectomy, which was diagnosed by MRI, and treated by surgical ligation of the right hepatic artery.
Case presentation
A 48-year-old patient had a laparoscopic cholecystectomy 45 days ago, followed by a second operation for biliary peritonitis after four days of cholecystectomy and peritoneal cleansing with drainage of the biliary tract using a T-tube drain. The patient was discharged on postoperative day (POD) 5 and his drain was removed four weeks later.
On the 45th day post cholecystectomy, the patient presented to our center with abdominal pain, vomiting, and hemodynamic instability. After hemodynamic resuscitation, the MRI was performed and showed a large hematoma associated with a pseudoaneurysm of the right hepatic artery (Figure 1).
Magnetic resonance imaging showing pseudoaneurysm of the right hepatic artery (arrow) with large hematoma.
Initial laboratory investigations portrayed a hemoglobin of 8 g/dL, hematocrit value of 20.3%, and platelet count of 310 × 10^3^ cells/µL (Table 1).
A subcostal laparotomy was performed, and a large hematoma was found and evacuated, after the pringle maneuver, the pseudoaneurysm was resected, then the right hepatic artery was ligated with clips. A subhepatic drain was placed (Figures 2A-2C).
Per-operative findings. (A) Pseudoaneurysm (arrow) with large hematoma. (B) Injury of the right hepatic artery after dissection (arrow). (C) Ligation of the right hepatic artery with clips (arrow).
The patient spent 14 days in intensive care following a pneumopathy treated with broad-spectrum antibiotics and was discharged on POD 20. The drain returned 30 cc of bile in the first week, 10 cc during the next 18 days, and was removed once the bile drainage stopped.
Discussion
The right hepatic artery injury is a well-documented complication of cholecystectomy, it may be isolated in 7% of cases in an autopsy series of cholecystectomy patients or associated with an injury to the common bile duct in 20% to 40% of cases [3,4]. These vascular injuries are either iatrogenic or caused by erosion due to biliary leakage, which manifests itself as a pseudoaneurysm [4]. The time between cholecystectomy and clinical signs can range from six days to five years, with an average of 36 days [3,4]. Symptoms often include haemobilia (90%), melena, vomiting, jaundice due to compression of the bile duct caused by the hemoperitoneum [5,6], and shock often due to aneurysm rupture [7].
The ideal treatment for extrahepatic aneurysms is arterial embolization or, rarely, stenting to close the breach [2,8]. The advantage is easy access to the breach, which avoids the morbidity of surgery, and in the event of failure, the surgical excision of the aneurysm and ligation of the right branch of the hepatic artery are the most common procedures [8]. A preoperative study of anatomical variations and preoperative cholangiography can help prevent vascular lesions [8].
Our patient underwent surgery for biliary peritonitis on POD 4, following a biliary leak in which a T-tube drain was placed in the biliary tract and then removed four weeks later. On the 45th day post cholecystectomy, abdominal pain and vomiting prompted an MRI, which revealed a hematoma and a pseudoaneurysm of the right hepatic artery. Peritonitis or an intra-abdominal collection was suspected. This pseudoaneurysm was probably due to an unrecognized injury in the right hepatic artery or to erosion following the patient's biliary leak. Surgical ligation of the right hepatic artery was indicated due to the non-availability of emergency embolization and remains a first-line treatment in our situation.
Conclusions
Pseudoaneurysms of the right hepatic artery following cholecystectomy due to either injury or erosion of this artery following a biliary leak. This is a rare complication often neglected by surgeons, manifesting as vomiting, hemoperitoneum, and haemobilia. The ideal treatment is embolization, with surgery advised in cases of hemodynamic instability or embolization failure. To prevent this complication, it is important to conduct radiological studies, perform open surgery if necessary, and adhere to safety protocols.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Biliary lithiasis (Article in French)Presse Med Payen JL Muscari F Vibert E Ernst O Pelletier G 5675804020112139744810.1016/j.lpm.2011.01.024 · doi ↗ · pubmed ↗
- 2Management of post cholecystectomy complications Surg Clin North Am Feng XC Phillips E Shouhed D 88991010120213453715010.1016/j.suc.2021.06.012 · doi ↗ · pubmed ↗
- 3Cholecystectomy and hepatic artery injuries Arch Surg Halasz NA 1371381261991199299010.1001/archsurg.1991.01410260021002 · doi ↗ · pubmed ↗
- 4Management of a pseudo-aneurysm in the hepatic artery after a laparoscopic cholecystectomy Ann R Coll Surg Engl Senthilkumar MP Battula N Perera M 4564609820162758030810.1308/rcsann.2016.0182 PMC 5210007 · doi ↗ · pubmed ↗
- 5An unusual presentation of hepatic artery aneurysm as a complication of laparoscopic cholecystectomy Eur J Surg Hewes JC Baroni ML Krissat J Bhattacharya S 566568168200212666698 · pubmed ↗
- 6Post-laparoscopic cholecystectomy extra-hepatic arterial pseudoaneurysm: an uncommon complication Int J Surg Case Rep Ullah K Baig MA Jan Z Nazar MW Shardha HK Kumar G 1072219520223559834210.1016/j.ijscr.2022.107221 PMC 9127149 · doi ↗ · pubmed ↗
- 7Severe hemobilia from hepatic artery pseudoaneurysm Case Rep Gastrointest Med Sansonna F Boati S Sguinzi R Migliorisi C Pugliese F Pugliese R 925142201120112260643110.1155/2011/925142 PMC 3350305 · doi ↗ · pubmed ↗
- 8Complications de la cholécystectomie EMC - Techniques chirurgicales - Appareil digestif Barbier L Hobeika C 960402023